Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
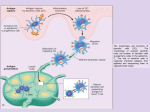
CD4 explosion after effective HAART in HIV people: the hidden meaning Miriam Lichtner Ricercatore Malattie Infettive Dipartimento Sanità Pubblica e Malattie Infettive Sapienza Università di Roma, polo pontino Background The number of circulating CD4+ T lymphocytes in patients with human immunodeficiency virus is the most robust predictive factor for: assessing HIV disease stage predicting progression to clinical AIDS and AIDS-related death determining antiretroviral treatment eligibility monitoring response to therapy The kinetic and the magnitude of CD4+ T recovery is extremely variable among ART treated subjects. 2015 Italian guidelines HIV Important Tools: • Absolute number CD4+ • % CD4+ • CD4/CD8 ratio Two particular populations can be described: 1) The ‘CD4-exploders’ (CD4e), defined as people gaining a large amount of cells under a defined time: a high amount of virgin T cells and a reduced T cells with a phenotype typical of lymphocytes with an increased tendency to undergo cell activation/death (Mussini et al. 2000) higher plasma levels of IL-7, a cytokine with a crucial importance for the generation and survival of T cells. BUT high amount of IL-7 has shown to be related to breast cancer, colon cancer, hematological malignancies, autoimmune diseases (such as multiple sclerosis, rheumatoid arthritis) (Kim et al., 2008). 2) The “CD4 peak achievers” (CD4a), who reach a very high level of CD4+ T cells: - Never studied as a separated population It could be important to further characterize these populations and investigate whether such extreme CD4 recoveries might modify persons’ risk of severe non-AIDS event (sNAE) or death. Aim of the study Incidence and clinical-demographic features of “CD4 exploder” (CD4e) and “CD4 peak achiever” (CD4a) over suppressive cART in ICONA cohort To evaluate the association between these conditions and the risk of sNAE/death and all cause mortality Methods Inclusion criteria: All Icona HIV+ patients enrolled before December 2015, who started cART from naïve and achieved/maintained VL<50cp/ml Arbitrary definition: CD4 exploders (CD4e) = gain/maintenance >600 cells/mm3 above precART after 2 years of ART CD4 peak achievers (CD4a) = achievement of absolute CD4>1000 followed by at least another consecutive >1000 value after 2 years ART 1. We aim to estimate the incidence of these 2 endpoints by 2, 5 and 10 years of suppressive cART and to identify factors independeently associated with the chance of being a CD4 explorer or absolute peak achiever using standard survival analysis (Kaplan-Meier curves, Cox regression). Unadjusted and adjusted HR will be calculated. 2. CD4 explorer and CD4 absolute peak achiever will be used as covariates in a survival analysis with time zero 2 years after viral suppression and endpoint time to severe non-AIDS events in those who were still free from non-AIDS cancer at that point. Kaplan-Meier curves and Cox regression analyses will be employed. Unadjusted and adjusted HR will be calculated after controlling for a number of factors that are associated with both CD4 explosion and risk of severe-non AIDS. Methods Endpoints: to be a CD4e; to be a CD4a Incidence by 2 years of suppressive cART; Kaplan-Meier curves/Cox regression model to identify factors independently associated; Endpoint: sNAE (malignancies, CCVD, renal, liver, pneumonia, sepsis)/death and all cause mortality Survival analysis with T0 2 years from the date of VL suppression comparing the risk of sNAE/death in the two populations. Incidence of CD4 exploders and CD4 peak achievers by years CD4 e n=879/7259 (12%) By 2 years CD4 a n=747/7259 (10.2%) By 2 years Total population Characteristics N= 7259 Gender, n(%) Female 1705 (23.5%) AIDS diagnosis, n(%) Yes 468 (6.4%) Median (IQR) 37 (32, 43) Age, years HCV positivity 867 (11.9%) Risk factors Eterosexual 2925 (40.3) IDU 1149 (15.9%) 1,35 1,06 0,77 0,2 1,04 0.00 Time since HIV diagnosis <0.001 CD4 nadir 0,015 cART with PI 0, 065 AIDS 1,11 CMVIgG+ vs. CMVIgG- 0,038 HCVAb+ vs. HCV Ab- 1,07 Hetero vs. MSM 0,8 Hetero vs. IVDU p<0,001 Female vs. male Age, +10 year AHR 95%IC Adjusted Hazard ratio of being a CD4 exploder (Cox regression) 5 0,074 1,48 1,22 1 0,2 <0.001 1 <0,001 Time since HIV diagnosis 0,8 CD4 nadir 0, 066 cART with PI 1,03 AIDS 0,75 0,87 CMVIgG+ vs. CMVIgG- 0,006 HCVAb+ vs. HCV Ab- 1,12 Hetero vs. MSM 0,8 Hetero vs. IVDU p<0,001 Female vs. male Age, +10 year AHR 95%IC Adjusted Hazard ratio of being a CD4 peak achiever (Cox regression) 5 0,021 1,35 1,34 1,33 1,25 1,02 Adjusted Hazard ratio of being a CD4 peak achiever AND a CD4 exploder =HIV people who gained more than 600 and achieved 1000 or more CD4 • Higher CD4 nadir • Female gender • cART with PI • Younger age • HCV (AHR:0.65, p=0.018) PROSPECTIVE ANALISYS Prospective analysis Study populations: CD4 e n = 338/3935 CD4 a n = 303/3935 CD4 e + CD4a n= 187 Events during 5 years: 176 SNAE 42 death Type of SNAE and death includes both composite endpoints Survival analysis End point: SNA event and all cause death log rank p=0.030 CD4 exploders log rank p=0.09 CD4 peak achievers 1,63 1,36 1,16 0,98 0,2 0,059 0,945 0,98 Time from cART initiation to baseline 0,53 CD4 peak achiever 0,16 CD4 exploder 0,015 cART with PI 0, 029 AIDS 1 CMVIgG+ vs. CMVIgG- p<0,001 HCVAb+ vs. HCV Ab- CD4 nadir 1,62 Female vs. male Age, +10 year AHR 95%IC Hazard Ratio of composite SNA or all cause mortality (95% CI) p-value 5 0,024 0,97 1,09 Conclusions 1 • A high CD4 recovery after 2 years effective cART , have been observed in 12% and 10%, but the cumulative incidence continue to increase over 10 years of FU without a “plateau effect” • Female gender and young age augment the risk to obtain a CD4 expansion and, or a CD4 peak (>1000) underling the importance to consider gender and age in approaching HIV subjects • Interestingly AIDS at presentation doesn’t seem to be an obstacle for achieving CD4 peak, but could increase the possibility to have a high delta suggesting a “survival selection bias” or a specific enhance of immunity during OI • Considering coinfections, only HCV seems to decrease the chance to obtain the two endpoints, even if with a marginal p value and HCV-RNA has not been considered • PI based therapy seems to be associated to about 40% higher possibility to obtain the two endpoints confirming data that has been observed in clinical practice but not always in case control study Conclusions 2 • Regarding the clinical impact, CD4 expanders seem to have a significant lower risk for SNAE/all cause death, while achieving CD4 peak seems to play a minor role. • Adjusting for other known confounders, CD4 expansion was associated with 50% decreased risk of SNAE/all cause death, while older age, HCV positivity and a longer time of cART initiation to virological suppression increase the risk. • These results suggest that not only a “standard” immune recovery should be induced by cART, but high expansion of CD4 is needed to reduce morbidity and mortality in HIV population. • To increase the proportion of CD4 exploders that is about 10%-30% special strategy should be used. Initial use of PI seems to be important, together with a rapid suppression of HIV replication and other immune intervention (IL-2, IL-7) Further analysis • A better characterization of the cause of death should be done in order to understand the role of CD4 expansion and peak achievement on the different pathology such us cerebro-cardiovascular disease and cancer • A more precise distinction of the two populations to better understand the role of peak achievers • To assess the degree of residual T and monocyte immune activation in CD4 e and CD4a (biological studies) • To evaluate the plasma level of IL7, IL7RA polymorphisms and apoptotic factors in the two populations (biological studies) • To study the role of the new INI-based therapy in determining CD4e and CD4a • To evaluate the impact of HCV eradication for the different endpoint. Authors Giulia Marchetti1, Alessandro Cozzi Lepri3, Serena Vita4, Annalisa Saracino5, Andrea Gori6, Cristina Mussini7, Giordano Madeddu8, Antonella d'Arminio Monforte1 for the ICONA Foundation Study 1Clinic of Infectious Dis, University of Milan, San Paolo Hospital, Milano, 2University of Rome Sapienza, Polo Pontino, Latina, 3UCL Medical School, Royal Free Campus, London, 4University of Rome Sapienza, Roma, 5University of Bari, Bari,6University of Milano-Bicocca, Milano, 7University of Modena and Reggio Emilia, Modena, 8University of Sassari, Sassari ICONA FOUNDATION STUDY COHORT BOARD OF DIRECTORS A d’Arminio Monforte (Vice-President), M Andreoni, G Angarano, A Antinori, F Castelli, R Cauda, G Di Perri, M Galli, R Iardino, G Ippolito, A Lazzarin, CF Perno, F von Schloesser, P Viale SCIENTIFIC SECRETARY A d’Arminio Monforte, A Antinori, A Castagna, F Ceccherini-Silberstein, A Cozzi-Lepri, E Girardi, S Lo Caputo, C Mussini, M Puoti STEERING COMMITTEE M Andreoni, A Ammassari, A Antinori, C Balotta, A Bandera, P Bonfanti, S Bonora, M Borderi, A Calcagno, L Calza, MR Capobianchi, A Castagna, F Ceccherini-Silberstein, A Cingolani, P Cinque, A Cozzi-Lepri, A d’Arminio Monforte, A De Luca, A Di Biagio, E Girardi, N Gianotti, A Gori, G Guaraldi, G Lapadula, M Lichtner, S Lo Caputo, G Madeddu, F Maggiolo, G Marchetti, S Marcotullio, L Monno, C Mussini, S Nozza, M Puoti, E Quiros Roldan, R Rossotti, S Rusconi, MM Santoro, A Saracino, M Zaccarelli. STATISTICAL AND MONITORING TEAM A Cozzi-Lepri, I Fanti, L Galli, P Lorenzini, A Rodano, M Shanyinde, A Tavelli BIOLOGICAL BANK INMI F. Carletti, S. Carrara, A Castrogiovanni, A. Di Caro, F. Petrone, G. Prota, S Quartu, S. Truffa. PARTICIPATING PHYSICIANS AND CENTERS Italy A Giacometti, A Costantini, C Valeriani (Ancona); G Angarano, L Monno, C Santoro (Bari); F Maggiolo, C Suardi (Bergamo); P Viale, E Vanino, G Verucchi (Bologna); F Castelli, E Quiros Roldan, C Minardi (Brescia); T Quirino, C Abeli (Busto Arsizio); PE Manconi, P Piano (Cagliari); B Cacopardo, B Celesia (Catania); J Vecchiet, K Falasca (Chieti); L Sighinolfi, D Segala (Ferrara); F Mazzotta, F Vichi (Firenze); G Cassola, C Viscoli, A Alessandrini, N Bobbio, G Mazzarello (Genova); C Mastroianni, V Belvisi (Latina); P Bonfanti, I Caramma (Lecco); A Chiodera, AP Castelli (Macerata); M Galli, A Lazzarin, G Rizzardini, M Puoti, A d’Arminio Monforte, AL Ridolfo, R Piolini, A Castagna, S Salpietro, L Carenzi, MC Moioli, C Tincati, G Marchetti (Milano); C Mussini, C Puzzolante (Modena); A Gori, G Lapadula (Monza); N Abrescia, A Chirianni, G Borgia, F Di Martino, L Maddaloni, I Gentile, R Orlando (Napoli); F Baldelli, D Francisci (Perugia); G Parruti, T Ursini (Pescara); G Magnani, MA Ursitti (Reggio Emilia); R Cauda, M Andreoni, A Antinori, V Vullo, A Cristaudo, A Cingolani, G Baldin, S Cicalini, L Gallo, E Nicastri, R Acinapura, M Capozzi, R Libertone, S Savinelli, A Latini (Roma); M Cecchetto, F Viviani (Rovigo); MS Mura, G Madeddu (Sassari); A De Luca, B Rossetti (Siena); P Caramello, G Di Perri, GC Orofino, S Bonora, M Sciandra (Torino); M Bassetti, A Londero (Udine); G Pellizzer, V Manfrin (Vicenza).