Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
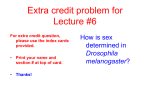
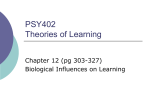
[CANCER RESEARCH 61, 7268 –7276, October 1, 2001] Multipoint Imprinting Analysis Indicates a Common Precursor Cell for Gonadal and Nongonadal Pediatric Germ Cell Tumors1 Dominik T. Schneider, Amy E. Schuster, Michael K. Fritsch, Jie Hu, Thomas Olson, Stephen Lauer, Ulrich Göbel, Elizabeth J. Perlman,2 the Pediatric Oncology Group, and German Pediatric Germ Cell Tumor Study Group Division of Pediatric Pathology, Department of Pathology, Johns Hopkins Medical Institutions, Baltimore, Maryland 21287 [D. T. S., A. E. S., M. K. F., J. H., E. J. P.]; Department of Pediatric Hematology and Oncology, Children’s Hospital, Heinrich-Heine-University, Medical Center, Düsseldorf, Germany D-40225 [D. T. S., U. G.]; Department of Pathology, University of Wisconsin-Madison, Madison, Wisconsin [M. K. F.]; Department of Genetics, University of Pittsburgh, Pennsylvania [J. H.]; and Pediatric Hematology and Oncology, Emory University School of Medicine, Atlanta, Georgia 30322 [T. O., S. L.] ABSTRACT Pediatric germ cell tumors (GCTs) commonly arise at extragonadal sites. It has been proposed that nongonadal GCTs arise from ectopic primordial germ cells that have aberrantly migrated during embryogenesis. During a time between their migration and development to mature gametes, primordial germ cells are characterized by their lack of imprinting, which can be assessed by the evaluation of allelic gene expression and DNA methylation in differentially methylated control regions. To elucidate the cellular origin of nongonadal GCTs, we evaluated the imprinting status of 21 gonadal and 21 nongonadal pediatric GCTs. Allele-specific H19 and IGF-2 expression was assessed with reverse transcription-PCR followed by digestion at polymorphic restriction sites. DNA methylation was evaluated after bisulfite modification, PCR amplification, and restriction digestion at a consistently methylated CpG dinucleotide within the 5ⴕ flanking region of the SNRPN gene. These results were compared with genetic gains and losses determined by comparative genomic hybridization. Seven of 15 informative tumors showed biallelic H19 expression, and 8 of 17 informative tumors showed biallelic IGF-2 expression. The frequency of biallelic gene expression was comparable in gonadal and nongonadal GCTs. Sixteen of 19 gonadal GCTs and 17 of 21 nongonadal GCTs showed absence of methylation of SNRPN consistent with loss of imprinting. One testicular GCT and three nongonadal GCTs showed a somatic methylation pattern. Two ovarian teratomas and one mediastinal teratoma showed only methylated SNRPN, consistent with entry into meiosis. Twenty-one of 22 non-GCT control samples showed a somatic methylation pattern. Gonadal and nongonadal germ cell tumors are derived from primordial germ cells that have consistently lost the imprinting of SNRPN and partly lost imprinting of H19 and IGF-2. Because the imprinting pattern of the latter genes differs from that found in testicular GCTs of adult patients, our data suggest that pediatric GCTs arise from a different stage of germ cell development. INTRODUCTION GCTs3 can develop at any age and site including the gonads as well as extragonadal midline sites such as the coccyx, the mediastinum, and the brain. They show a marked heterogeneity in their histologic appearance, which may vary from mature organoid differentiation patterns in teratoma to highly malignant and clinically aggressive tumors such as seminoma, YST (also known as endodermal sinus tumor), embryonal carcinoma, and choriocarcinoma. However, gonadal and nongonadal GCTs of all ages are grouped together and termed “germ cell tumors” in keeping with the theoretical concept of Received 4/10/01; accepted 7/26/01. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported by the American Cancer Society (RPG-97-113-01-CCE). D. T. S. receives a Dr. Mildred Scheel Grant from the German Cancer Aid (Deutsche Krebshilfe e.V.). 2 To whom requests for reprints should be addressed, at Division of Pediatric Pathology, Johns-Hopkins Medical Institutions, 600 N. Wolfe Street, Baltimore, MD 21287. Phone: (410) 614-1988; Fax: (410) 614-9386; E-mail: [email protected]. 3 The abbreviations used are: GCT, germ cell tumor; YST, yolk sac tumor; PGC, primordial germ cell; LOI, loss of imprinting; ICR, imprinting control region; SNRPN, small nuclear ribonucleoprotein polypeptide N gene; CGH, comparative genomic hybridization; RT-PCR, reverse transcription-PCR. Teilum (1) that all subtypes develop from a common precursor cell, the PGC. There are at least two lines of evidence that support this hypothesis. First, malignant nongonadal GCTs show genetic aberrations that resemble those of gonadal GCTs of the corresponding age group (2–5). Only the association between Klinefelter syndrome and GCTs appears to be unique to nongonadal GCTs (particularly mediastinal GCTs) of adults (6, 7). It is remarkable, however, that GCTs arising in infancy and those arising after the onset of puberty show profound differences in their molecular biology despite identical histology. Postpubertal malignant testicular, ovarian, and nongonadal GCTs are characterized by an isochromosome 12p in about 80% of cases and amplification of segments of 12p in most of the remaining cases (5, 8, 9). In contrast, nongonadal GCTs arising in infants and toddlers display different genetic aberrations such as imbalances of chromosome 1 and loss of 6q, and they lack amplification of 12p in most cases (3–5, 10, 11). In summary, genetic analysis distinguishes subgroups of GCT by age, rather than by tumor site or specific histological subentities (8). This raises the possibility that pre- and postpubertal GCTs may develop from germ cells at different stages of their development, or alternatively, some subsets may arise from embryonic stem cells. The second line of evidence supporting a germ cell origin of extragonadal GCTs comes from the analysis of early germ cell development and migration. Embryologic studies (12, 13) reveal that PGCs first appear in the extraembryonic mesoderm and actively migrate along the mesentery to the posterior hindgut, in very close proximity to the coccyx, before they enter the gonadal ridges. This migration is directed by the c-kit and stem cell factor receptor-ligand pair among others and requires the interaction with extracellular matrix [for review, see Wylie (14)]. In light of these findings, it has been proposed that nongonadal GCTs develop from PGCs that for some reason failed to enter the gonadal ridge. Fetal mice often contain extragonadal germ cells; however, these have never been seen in the mediastinum or brain and instead are more commonly found in such sites as the adrenal gland, sites where GCTs do not arise. Extragonadal germ cells have not been observed in human fetuses. It has been suggested that they may undergo apoptosis because of lack of growth factor support (12, 15–17). However, the possibility that extragonadal GCTs may instead arise from embryonal stem cells has also been raised and is supported by the midline location almost exclusively seen in these tumors. The above observations have led to yet another hypothesis regarding the origin of nongonadal GCTs that also takes into account their genetic similarity to gonadal tumors. Chaganti et al. (2, 8) proposed a model that mediastinal GCTs develop from early gonadal lesions, giving rise to cells that “recapitulate embryonal memory and reverse migrate to thymus and pineal where receptive environments permit their establishment as primary tumors.” In support of this hypothesis, the authors refer to the thymus as an organ that is well appreciated as an intermediate migratory site of other cell types such as T lymphocytes. In addition, the abundance of germ cells in the testis compared 7268 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS with the ovary might explain the fact that nongonadal GCTs predominantly develop in males. However, this is not true for nongonadal GCT in children, which show a female predominance (18). In summary, there is no evidence that nongonadal GCTs indeed derive from PGCs, and molecular markers are needed to evaluate the presumably common origin of gonadal and nongonadal GCTs. Immunological and genetic markers have been informative in tracing back the origin of some childhood neoplasms to the fetal period. For instance, in childhood acute lymphoblastic leukemia, monoclonal antigen receptor rearrangements and leukemia-specific chromosomal rearrangements were detected in neonatal blood samples, and the molecular genetic evaluation of identical twins with leukemia suggested a fetal origin of the leukemia (19, 20). Unfortunately, these methods cannot be applied to the analysis of solid neoplasms such as GCTs, because corresponding prenatal tissue samples are not available apart from rare fetal teratoma. Therefore, we used an alternative approach to study the cellular origin and time of origin of extragonadal GCTs. We examined GCTs for unique molecular features of their presumed cell of origin, the PGC. Others (21–25) have already proposed that LOI may serve as such a molecular marker of a defined stage of PGC development. However, insufficient data are available for nongonadal and pediatric GCTs to arrive at meaningful conclusions. The term imprinting refers to the phenomenon that in somatic cells the two alleles of some genes are expressed in an asymmetric pattern depending on the inheritance of the allele from either father or mother (26 –28). DNA methylation of 5⬘-CG-3⬘ (CpG) dinucleotides represents the most significant biochemical marker of imprinting and allows the distinction between the paternal and the maternal alleles. Among all of the imprinted genes, H19 and IGF-2 have been studied most extensively (22, 24, 29). They are part of an imprinted gene cluster on chromosome 11p15, and they share a common enhancer downstream of the H19 gene. Differential methylation of the ICR upstream of the H19 promoter controls imprinting of IGF-2 by interfering with the binding of the vertebrate enhancer-blocking protein CTCF, which prevents the activation of the IGF-2 promoter by its enhancer (boundary model; Fig. 1; Refs. 30, 31). In addition, imprinting of IGF-2 is controlled independently of H19 by a differentially methylated silencer element (32). The imprinted gene for the small nuclear ribonucleoprotein polypeptide N gene (SNRPN) is located within a region on chromosome 15q11–13, which is microdeleted in Prader-Willi syndrome or Angelman syndrome (33, 34). Evaluation of the SNRPN methylation pattern has been proposed as a diagnostic test for both syndromes, because the methylated maternal allele is lost in Angelman syndrome, whereas the unmethylated paternal allele is deleted in Prader-Willi syndrome (34, 35). Loci on both 11p15 and 15q11–13 have been reported to be deleted only rarely in pediatric and adult GCTs (10, 36). Therefore, it is unlikely that cytogenetic events will substantially alter the imprinting pattern of GCTs. During their development, PGCs erase their inherited imprint and establish a new sex-specific imprinting pattern. If one hypothesizes that GCTs preserve the original imprinting status of their cell of origin, one may assume that GCTs arising from PGCs before entry into the gonadal ridge and GCTs arising from premeiotic germ cells will show erased imprinting (biallelic expression of H19 and IGF-2; no methylation of the H19 ICR or the SNRPN gene). On the other hand, GCTs developing from PGCs that have entered meiosis should display a sex-specific gametic imprinting pattern. This study summarizes our analysis of the IGF-2, H19, and SNRPN imprinting status of 42 gonadal and nongonadal GCTs in children and adolescents. PATIENTS AND METHODS Tumor Samples, DNA Extraction, and RNA Extraction. Thirty-five fresh-frozen and seven archival germ cell tumor samples from children and adolescents were collected at the Pediatric Oncology Group- and MAKEI(German Maligne Keimzelltumoren Study Group) affiliated institutions. The histology of all of the tumors was reviewed centrally. Control specimens included 12 non-neoplastic tissue specimens and 12 pediatric tumors in which loss of imprinting has been reported previously (eight renal tumors and four hepatoblastomas) (28, 37). Before DNA and RNA extraction, specimens were analyzed histologically to confirm ⬎80% viable tumor cell content. Tissue sections were digested with proteinase K in SDS, and DNA was extracted with phenol/chloroform followed by ethanol precipitation. For RNA extraction, 0.1– 0.4 g of frozen tissue was minced, homogenized, and dissolved in 1 ml of TRIzol (Life Technologies, Inc., Rockville, MD). RNA was extracted with chloroform and precipitated with isopropanol. The extraction was repeated Fig. 1. Boundary model of the IGF-2 and H19 cluster on chromosome 11p15. IGF-2 and H19 share a common enhancer downstream of H19. On the maternal allele, the ICR upstream of H19 is unmethylated and binds the vertebrate enhancerblocking protein CTCF, which inhibits the activation of the IGF-2 promoter by the enhancer. On the paternal allele, the H19 promoter and ICR are methylated, thus silencing H19 and interfering with CTCF binding. The IGF-2 promoter is activated by its enhancer (30, 31). 7269 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS once. After incubation with 1 unit/l of DNase (Roche Molecular Biochemicals, Mannheim, Germany) for 20 min at 37°C, phenol/chloroform extraction, and ethanol precipitation, the amount of RNA was quantified by UV spectroscopy. RNA quality was assessed on an ethidium bromide-stained 1% agarose gel, which should reveal the 28 S and 18 S bands of rRNA. CGH. Nick translation, comparative hybridization, and image analysis were performed as described in detail previously (3). Briefly, DNA (1 g) from tumor and normal male control tissue was labeled with Spectrum-Green and Spectrum-Red (Vysis Inc., Downers Grove, IL) by nick translation. Equal amounts of labeled tumor and control DNA were cohybridized with Cot-1 DNA against normal male metaphase spreads. After posthybridization washes, slides were counterstained with 0.1 g/ml 4⬘,6-diamidino-2-phenylindole-2 HCl in antifade. Gray level images were acquired for each fluorescent dye using the dedicated Cytovision software and hardware of the Applied Imaging Corporation (Santa Clara, CA). Chromosomes were identified using reverse 4⬘,6-diamidino-2-phenylindole banding. At least 15 representative chromosomes were analyzed to generate a green:red ratio profile with mean and SE for each chromosome. A deviation above 1.2 and below 0.8 was considered gain or loss of chromosomal material, respectively. Allelic Expression of IGF-2 and H19. The polymorphisms at the ApaI restriction site in exon 9 of IGF-2 and at the AluI restriction site in exon 5 of H19 were analyzed (38). In a first step, the genomic polymorphism of each patient was evaluated for both sites (39). Tumors from heterozygous patients were further analyzed by RT-PCR for allele-specific gene expression. RNA was reverse-transcribed with Superscript reverse transcriptase (Life Technologies, Inc.) and random hexamers (Perkin-Elmer, Branchburg, NJ). PCR amplification was performed on a Perkin-Elmer 2400 PCR thermocycler using 2.5 M of each primer (Table 1), buffer 3 (IGF-2) or 9 (H19; Stratagene, La Jolla, CA), 2 mM of each deoxynucleotide triphosphate, and AmpliTaq (H19) or AmpliTaq Gold (IGF-2; Perkin-Elmer). PCR conditions for IGF-2 were 94°C for 10 min, 30 cycles of 94°C for 30 s, 60°C for 1 min, and 72°C for 30 s, followed by final extension at 72°C for 10 min. PCR and RT-PCR of IGF-2 both resulted in a 292-bp product. PCR included water blanks as negative controls. For each sample analyzed by RT-PCR, a negative control without reverse transcriptase was included to monitor for contamination with genomic DNA. PCR products were ethanol precipitated, dissolved in distilled water, and digested overnight at 25°C with 20 units of ApaI, according to the manufacturer’s instructions (New England Biolabs, Beverly, MA). Digestion products were separated on a 2% ethidiumbromide-stained agarose gel. Samples showing both a 292-bp and a digested 227-bp DNA fragment were considered heterozygous for DNA or biallelic RNA expression, respectively. The 65-bp fragment was not reliably detected on the agarose gels. H19 was amplified with nested PCR under the following conditions: 94°C for 5 min, 20 cycles of 94°C for 1.5 min, 56°C for 1 min, and 72°C for 1.5 min. One l of the first PCR was transferred to a new tube with fresh reagents, and nested PCR was performed under identical conditions for another 20 cycles. The amplification of genomic DNA resulted in a 833-bp product. Because of introns between the exons 3 and 4, as well as 4 and 5, RT-PCR resulted in a 672-bp product, and the absence of the 833-bp product served as an additional control for contamination with genomic DNA. Amplification products were ethanol precipitated and digested overnight with 20 units of AluI, according to the manufacturer’s instructions (Life Technologies, Inc.). The 833-bp PCR product amplified from genomic DNA was digested with AluI into 261-, 153-, 147-, 91-, 76-, 49-, 41-, 10-, and 5-bp fragments. The restriction site at nucleotide 10380 (GenBank accession no. AF087017) is polymorphic, and as a consequence, the digestion may result in a 300-bp fragment instead of the two 153-bp and 147-bp fragments. RT-PCR products were digested into 261-, 147-, 76-, 72-, 60-, 41-, 10-, and 5-bp fragments. Polymorphism at the AluI restriction site results in a 219-bp fragment. Therefore, biallelic gene expression results in 261-bp, 219-bp, and 147-bp bands. Monoallelic expression, however, results either in 261-bp and 219-bp bands or in 261-bp and 147-bp bands. Methylation of the SNRPN Gene. Rather than expression analysis, methylation analysis was performed to determine the imprinting status of the SNRPN gene, because this approach does not depend on genetic polymorphism and therefore allows examination of all of the available tumor samples. The restriction site for CfoI in the 5⬘ flanking region of the SNRPN gene is methylated on the maternal chromosome in more than 96% of normal individuals and unmethylated on the paternal chromosome (33, 35). DNA modification was performed by overnight incubation with sodium bisulfite and hydrochinone according to the manufacturer’s instructions (Intergen, Purchase, NY). This modification was followed by a DNA extraction step with glass beads. Bisulfite-modified DNA (250 ng) was added to a 50-l PCR reaction mix, which consisted of 100 mM Tris-HCl (pH 9.2), 35 mM MgCl2, 250 mM KCl, 0.2 mM of each nucleotide, 1 M of each primer (Table 1), and 2.5 units of Taq DNA polymerase (Taq Gold; Stratagene). The primers bind to bisulfitemodified DNA only, and the primer-binding sites include no potentially methylated CpG dinucleotides, thus allowing amplification of the imprinted and nonimprinted allele. A negative control with unmodified DNA was included in each experiment. PCR conditions were 94°C for 10 min (one cycle), 1 min at 94°C, 1 min at 51°C, 1 min at 72°C for 35 cycles, and 25 cycles for nested PCR, respectively. The resulting 340-bp PCR product was ethanol precipitated and digested overnight with 20 units of CfoI (Promega, Madison, WI). The reaction products were separated in an ethidium bromide-stained 2% agarose gel. To monitor for complete restriction digestion, the H19-PCR product from genomic DNA was added to each reaction. CfoI digests this 833-bp product into 386-bp, 260-bp, 130-bp, and 57-bp fragments. Samples, which showed incomplete digestion of H19, were excluded from the analysis of the SNRPN methylation status. PCR products from methylated and therefore unmodified SNRPN alleles are digested into two 224-bp and 116-bp fragments, whereas PCR products from unmethylated (modified) alleles are not digested (340-bp band only). In cases showing both bands, the relative band intensities of the ethidium bromide staining was accessed with the Eagle Eyes system (Stratagene). ⌽X174 DNA cut with HaeIII was run in parallel to ensure that the measurement was in a linear range. As a result of the size difference between the two SNRPN bands, a 1.5:1 ratio was consistent with identical molar concentrations of both bands. In contrast, a ratio above 4.5:1 was considered predominance of the unmethylated allele, and a ratio below 0.5:1 was considered predominance of the methylated allele. RESULTS Clinical and Histological Data. We analyzed 21 gonadal and 21 nongonadal GCTs. Among the gonadal tumors, there were five testicular and 16 ovarian GCTs (Table 2). Of the latter, one tumor (dysgerminoma with a gonadoblastoma component) arose in a phe- Table 1 PCR-primersa Gene IGF-2 H19 SNRPN (after bisulfite treatment) a Primer Sequence Forward Reverse Forward Reverse Forward–nested Reverse–nested Forward Reverse Forward–nested Reverse–nested 5⬘-CTTGGACTTTGAGTCAAATTGG-3⬘ 5⬘-GGTCGTGCCAATTACATTTCA-3⬘ 5⬘-AACACCTTAGGCTGGTGG-3⬘ 5⬘-TGCTGAAGCCCTGGTGGG-3⬘ 5⬘-CACTATGGCTGCCCTCTG-3⬘ 5⬘-TCGGAGCTTCCAGACTAG-3⬘ 5⬘-GGTTTTTTTTTATTGTAATAGTGTTGTGGGG-3⬘ 5⬘-CTCCAAAACAAAAAACTTTAAAACCCAAATTC-3⬘ 5⬘-GGTTTTAGGGGTTTAGTAGTTTTTTTTTTTTAGG-3⬘ 5⬘-CAATACTCCAAATCCTAAAAACTTAAAATATC-3⬘ Refs. 34, 35, 38, and 39. 7270 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS Table 2 Age, histology, CGH profiles, and SNRPN methylation of 21 gonadal germ cell tumorsa 1 2 3 4 5 6 7ab 7bb 8 9 10 11c 12 13 14 15 16 17 18 19 20 21 Age Sex Site Histology Chromosomal gains and losses 3 mo 5 mo 6 mo 7 mo 11 mo 9 yr 12 yr 12 yr 14 yr 14 yr 16 yr 17 yr 18 yr 22 yr 4 yr 8 yr 12 yr 15 yr 17 yr 24 yr 4 yr 21 yr M M M M M F F F F F F F F F F F F F F F F F T T T T T O O O O O O O O O O O O O O O O O YST YST YST YST YST DYS DYS DYS DYS DYS DYS DYS/GO DYS DYS MGCT MGCT YST MGCT MGCT YST IT IT ⫹17p, ⫹20q ⫹3, ⫺4p, ⫺6q, ⫹8q, ⫹13, ⫺14, ⫺20p, ⫹20q, ⫹22 ⫺4, ⫺16, ⫹17q, ⫹22, ⫹X ⫺1p, ⫺13q, ⫺16 ⫹1q, ⫹3p, ⫺4p, ⫺5q, ⫺6, ⫹7p, ⫹9q, ⫺8 ⫹20q ⫹6p, ⫹12p, ⫹21 ⫹7, ⫹12p, ⫹21 ⫹1q, ⫺4, ⫺7p, ⫺12 ⫺1p, ⫹1q, ⫹4q, ⫹7, ⫹8, ⫹12, ⫺13, ⫹15, ⫹21 ⫹8, ⫹12p, ⫹15, ⫹21 ⫺4, ⫹8, ⫹12p, ⫹X, ⫺Y ⫹3, ⫹12p, ⫺13q ⫹1q, ⫹8, ⫹21 ⫹8, ⫹12p ⫹12p, ⫹21 ⫺1p, ⫹1q, ⫺5, ⫹12p, ⫺13, ⫺18q, ⫹20 ⫺4, ⫹7, ⫹8, ⫺10, ⫹12p, ⫺18 ⫹1q, ⫹10, ⫹12 ⫺1p, ⫹7p, ⫹8, ⫺9, ⫺11, ⫹12p, ⫺13, ⫺15, ⫺20, ⫹21, ⫺22 Normal, XX ⫹14 H19 IGF-2 SNRPN Monoallelic U M⫹U U Monoallelic Monoallelic Monoallelic Monoallelic Biallelic Monoallelic Monoallelic Biallelic Biallelic Biallelic Biallelic Monoallelic Biallelic Biallelic Monoallelic Biallelic Biallelic Monoallelic Monoallelic U U U U U U U U U U U U U U U M M a CGH profiles of patient numbers 1 to 5 and 6 to 21 have been reported by Perlman et al. (Ref. 3) and Riopel et al. (Ref. 9) respectively. T, testis; O, ovary; DYS, dysgerminoma; GO, gonadoblastoma; MGCT, mixed malignant GCT; IT, immature teratoma; M, methylated allele; U, unmethylated allele. b Patient 7a/7b, (a) tumor right ovary, (b) tumor left ovary. c Patient 11, gonadal dysgenesis with male pseudohermaphroditism. notypic female with a constitutional 46, XY karyotype and streak gonads (number 11). Among the nongonadal tumors, 11 developed at the sacrococcygeal region, eight in the mediastinum, and two in the central nervous system (Table 3). Fifteen nongonadal tumors developed in infants or children, and five developed in adolescents. Six patients were female, and 15 patients were male. In infants and prepubertal children, the only histological subtypes identified in both gonadal and nongonadal GCTs were YST and teratoma. After the onset of puberty, we also observed dysgerminoma, YST, immature teratoma, and mixed malignant GCTs, which showed a composite histology including germinomatous and nongerminomatous elements such as embryonal carcinoma, YST, choriocarcinoma, or teratoma (Tables 2 and 3). CGH. This analysis included 10 pure teratomas (six mature and four immature teratomas). All of the mature teratomas and three immature teratomas showed normal CGH profiles (Tables 2 and 3). One immature ovarian teratoma showed gain of chromosome 14. All of the malignant GCTs showed chromosomal imbalances on CGH analysis (Tables 2 and 3). Specific CGH profiles did not correlate with histological differentiation or tumor site. However, two distinct CGH patterns could be distinguished by age. Regardless of site, malignant GCTs in infants and children younger than eight years (n ⫽ 16) most commonly showed imbalances at chromosome 1 (loss 1p and/or gain 1q), gain of 3p, loss of 4 and 6q, and gain of 20q. Only one ovarian malignant GCT in a four-year-old girl showed gain of 12p. Conversely, gain of 12p was the most consistent aberration found in GCTs arising after eight years of age and was found in 11 of 16 tumors. Other recurrent aberrations in adolescents were gain of 1q, gain of chromosome 8 and 21, and loss of chromosome 13. One tumor (number 19) showed loss of chromosome 11 and 15. Because this tumor showed biallelic expression of IGF-2, the tumor is most probably polyploid. Four other tumors showed gain of chromosome 15. Otherwise, no chromosomal imbalances of the chromosomes 11 and 15 were detected with CGH. Methylation Pattern of the 5ⴕ Flanking Region of the SNRPN Gene. In 40 patients, DNA was available for analysis of the methylation of the 5⬘ flanking region of the SNRPN gene. In 16 of 19 Table 3 Age, histology, CGH analysis, and SNRPN methylation of 21 nongonadal germ cell tumorsa 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Age Sex Site Histology Chromosomal gains and losses 1d 1 wk 1 mo 2 yr 14 yr 14 yr 15 yr 16 yr 3 yr 14 yr 11 mo 1 yr 2 yr 2 yr 2 yr 3 yr 3 yr 4d 10 d Infant 1 yr M M M M M F F M M M F M M M M M M F M F F Med Med Med Med Med Med Med Med CNS CNS Co Co Co Co Co Co Co Co Co Co Co IT IT MT YST, IT MGCT MT MT YST MGCT GER YST YST YST YST YST YST YST IT, YST MT MT MT Normal, XY Normal, XY Normal, XY ⫺1p, ⫹2p, ⫹3, ⫺4, ⫺5q, ⫺13, ⫹18q, ⫹21 ⫹8, ⫹12p, ⫺18, ⫹X Normal, XX Normal, XX ⫹2p, ⫹3p, ⫹8q, ⫹12p, ⫺13, ⫹14q, ⫹17q, ⫹20, ⫹21 ⫹1q, ⫹2p, ⫹3p, ⫺20q ⫹17q ⫹1q, ⫺4q, ⫹15, ⫹20q ⫺1p, ⫹1q, ⫹3p, ⫺4q, ⫺6q, ⫹10, ⫹14q, ⫹17q, ⫹20q ⫺1p, ⫹3p, ⫹6p, ⫹13, ⫹14q ⫺1p, ⫹1q, ⫹3q, ⫺6q, ⫺8q, ⫹11q, ⫹12q, ⫹19p, ⫹20q ⫹3p, ⫺4, ⫹6p, ⫹10, ⫹15, ⫹20 ⫺1p, ⫹2p ⫺5q, ⫺6q, ⫹20 ⫹1q Normal, XY Normal, XY Normal, XX H19 IGF-2 Biallelic Monoallelic Monoallelic Biallelic Monoallelic Monoallelic Biallelic Biallelic Monoallelic Biallelic Monoallelic Biallelic Biallelic SNRPN M U U U U U U U U U U U U U U U⫹M U U⫹M U U U⫹M a CGH profiles of patient numbers 34 and 35 have been reported by Perlman et al. (Ref. 3); Med, mediastinum; Co, coccyx; IT, immature teratoma; MT, mature teratoma; MGCT, mixed malignant GCT; GER, germinoma; M, methylated allele; U, unmethylated allele; CNS, central nervous system. 7271 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS Fig. 2. Analysis of the methylation status of the 5⬘ flanking region of SNRPN. One control sample, five gonadal GCTs, and five nongonadal GCTs. Agarose gel electrophoresis after bisulfite DNA modification, PCR amplification, and restriction digestion at a monoallelically methylated CpG dinucleotide. The 833-bp PCR product for H19 is included in the reaction to monitor for complete digestion. DYS, dysgerminoma; MGCT, mixed malignant GCT; IT, immature teratoma; MT, mature teratoma; Test., testicular; Ov., ovarian; Med., mediastinal; Cocc., coccygeal. gonadal GCTs, only the unmethylated allele was present in the tumor, as demonstrated by the presence of the 340-bp band and absence of the 224-bp band (Table 2; Fig. 2). One testicular YST (number 3) showed both bands at the exact 1.5:1 ratio for ethidium bromide fluorescence, consistent with a somatic imprinting pattern in this tumor. Contamination with non-neoplastic tissue was excluded by histological evaluation of an adjacent section, and CGH analysis of the same DNA vial showed characteristic aberrations. Both ovarian immature teratomas showed the 224-bp but no 340-bp band, indicating the presence of a methylated SNRPN and absence of unmethylated SNRPN. Both tumors also showed monoallelic expression of IGF-2. This constellation is consistent with a maternal pattern of methylation. In 15 of 21 nongonadal GCTs, the analysis yielded only the 340-bp band of the unmethylated SNRPN allele. Among these, there were six teratoma and nine malignant GCTs. In two additional sacrococcygeal YSTs (Table 3; numbers 33 and 36), the 340-bp band was significantly more intense than the 224-bp band. The assessment of the relative ethidium bromide fluorescence intensities yielded a 4.9:1 ratio and a 13.6:1 ratio, respectively, indicating that more than half of the cells showed loss of SNRPN methylation. All of the tumors showing gain of chromosome 15 on CGH analysis demonstrated only the unmethylated SNRPN allele. Another sacrococcygeal YSTs (Table 3; number 37) showed a 3.9:1 ratio, consistent with loss of SNRPN methylation in 44% of cells. Lastly, one malignant GCT with a predominant immature teratoma component and about 25% YST component (number 39) showed a 2.4:1 ratio, consistent with loss of the methylated SNRPN in approximately 22% of cells. In this tumor, expression of both H19 and IGF-2 was biallelic. One teratoma (numbers 42 and 43) showed both bands but with a predominance of the unmethylated allele (ratio, 2.9:1). In contrast, one immature mediastinal teratoma of a neonate (Table 3; number 33) exclusively showed the 224-bp band, indicating that the unmethylated allele is absent in the tumor or that both alleles are methylated. The analysis of 12 non-neoplastic tissue samples and of 11 of 12 pediatric tumors yielded both bands at the expected 1.5:1 ratio (range, 1.3 to 1, 2.7 to 1). Only one hepatoblastoma showed no 224-bp band, indicating loss of SNRPN methylation (no chromosomal loss was detected with CGH). Allele-specific Expression of IGF-2 and H19. In 39 patients, fresh frozen tumor samples were available for the evaluation of IGF-2 and H19 expression through RT-PCR. Eighteen of 39 patients were heterozygous for IGF-2. Nine tumors showed monoallelic expression of IGF-2, and nine tumors showed biallelic IGF-2 expression (Table 4; Fig. 3). Twenty of 39 patients were heterozygous for H19, but in five patients, poor RNA quality did not allow for amplification. Seven of the remaining 15 tumors showed biallelic expression, and eight tu- mors showed monoallelic expression of H19 (Table 4; Fig. 4). The frequency of biallelic expression of H19 and IGF-2 was comparable among gonadal and nongonadal tumors and did not correlate with histological differentiation, sex, or age of the patients or with distinct CGH patterns (Table 4). Furthermore, there was no sex-dependent difference in the frequency of biallelic expression of IGF-2 or H19, respectively. Five patients were heterozygous for both H19 and IGF-2. One ovarian GCT showed biallelic expression of both genes, three tumors of female patients showed biallelic expression of H19 but monoallelic expression of IGF-2, and one tumor in a male showed monoallelic H19 but biallelic IGF-2 expression. DISCUSSION PGCs and Imprinting. The discussion of the biological significance of imprinting in mammals has focused on the impact of imprinted genes on the development of the offspring generation [parent offspring conflict hypothesis; for review, see Tilghman (26)]. Considered from a teleological perspective, it has been suggested that imprinting control mechanisms of fathers will support growth of their offspring, whereas mothers will try to limit and equally distribute their resources during pregnancy. This discussion very much reflects the ability of many imprinted genes such as H19 and IGF-2 to effectively alter cell growth and proliferation. On the other hand, the biological and evolutionary impact of other genes such as SNRPN is not as readily assessable, because these most probably control neurological maturation (26). Nevertheless, imprinted genes share common features. They are localized within several chromosomal clusters that include GC-rich sequences with differentially methylated CpG dinucleotides (DNA methylation sites). The allele-specific expression of imprinted genes is regulated by methylation of their promoters (40), silencer elements (32), or a shared imprinting control region, which interferes with Table 4 Allele-specific expression of H19 and IGF-2 with regard to tumor site, histology, and sex, and age Fifteen patients were informative for H19, and 18 patients were informative for IGF-2. H19 Site Histology Age Sex Total Gonadal Nongonadal Teratoma Malignant Infant Adolescent/adult Female Male IGF-2 Biallelic Monoallelic Biallelic Monoallelic 5 2 1 6 3 4 6 1 7 4 4 2 6 5 3 4 4 8 4 5 1 8 5 4 6 3 9 7 2 2 7 5 4 4 5 9 7272 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS Fig. 3. Allele-specific expression of IGF-2 of five gonadal and six nongonadal GCTs. Each lane of these agarose gels represents a RT-PCR product before (⫺) and after (⫹) restriction digestion of a polymorphic ApaI restriction site. Presence of both 292-bp and 227-bp bands proves biallelic expression. Abbreviations as above. promoter activation through an enhancer (Fig. 1; Refs. 30, 31). On the basis of the present knowledge, it appears that imprinting is controlled within these clusters, and different clusters are controlled independently. The presence of imprinted genes in mammals poses specific tasks to the developing germ cells. In contrast to somatic cells, which maintain the parent-specific imprinting pattern, germ cells have at some point to erase the imprint and establish a new, sex-specific imprinting pattern. At present, it is unclear whether the parental imprint is completely erased and by which biochemical mechanisms imprinting is erased and reestablished (26). Furthermore, the exact timing of erasure and establishment in germ cells has yet to be determined in more detail. Szabo and Mann (41) found biallelic expression of several imprinted genes (including IGF-2, H19, and SNRPN) in mouse PGCs that have already entered the gonads. In this study, biallelic expression was observed throughout gonadal germ cell development. In contrast, the comparison of allele-specific gene expression at the tip and the base of the allantois, where PGCs can first be appreciated as a distinct population, suggested that at least SNRPN may be expressed monoallelically in premigratory PGCs. However, one has to keep in mind that even somatic cells may show biallelic expression of imprinted genes at the single-cell level, suggesting that some post-transcriptional control mechanism may be of additional importance (42). Furthermore, biallelic expression of imprinted genes may be seen despite imprinting-specific DNA methylation (43, 44). However, the hypothesis that PGCs have erased their imprint by the time they enter into the gonadal ridge is supported by a recent study evaluating the methylation imprint of the imprinting control region of the human H19 (Fig. 1). The authors (25) found no methylation in fetal postmigratory PGCs but imprinting-specific methylation in adult male germ cells that enter into meiosis. In summary, these studies delimit a time frame in males ranging from at least the entry of PGCs into the gonadal ridge, maybe earlier, until meiosis entry, during which PGCs are void of imprinting. Evidence suggests the same boundaries for germ cells of females, al- though the actual time during which the PGCs are void of imprinting is considerably shortened because of entry into meiosis late in fetal life. Conversely, somatic cells and premigratory PGCs show somatic methylation patterns and monoallelic expression of imprinted genes. This suggests that imprinting is erased during PGC migration to the gonadal ridge. However, there are no data concerning the timely order of imprint erasure of different imprinted gene clusters during germ cell migration. LOI and Cancer. The role of imprinted genes and epigenetic changes in cancer biology was not elucidated until 1993, when LOI was reported in approximately 70% of Wilms’ tumors (45– 47). Other studies followed that reported LOI in a broad variety of carcinomas and pediatric embryonal cancers (29). In addition, LOI has been detected in normal tissue such as colonic mucosa and blood cells of patients with colon cancer (48). Therefore, LOI has to be considered not only a frequent event in tumorigenesis, but it may in some patients also constitute a predisposing factor for cancer development (49 –51). Its occurrence in somatic tumors may not be surprising, when one considers that many of the imprinted genes interfere with the regulation of cell growth and proliferation. In contrast, several studies of the SNRPN gene in cancer have not revealed a single case with LOI (29, 52, 53). These data are further supported by our analysis of 12 non-neoplastic and 12 neoplastic control samples, of which only one hepatoblastoma showed LOI. These data suggest that SNRPN is not involved in tumor development (26). This feature makes SNRPN an ideal candidate for the evaluation of the “native” imprinting pattern of the cell of origin of GCTs. Imprinting and Germ Cell Tumors. Van Gurp et al. (39) were the first to study the allele-specific expression of H19 and IGF-2 in adolescent testicular GCTs. They found biallelic expression of IGF-2 in 10 of 11 tumors and biallelic H19 expression in 12 of 14 informative tumors. They concluded that testicular GCTs develop from germ cells that have erased their imprint. LOI of IGF-2 and H19 appears to contribute to an increased expression of these genes in GCTs, as has Fig. 4. Allele-specific expression of H19; 672-bp RT-PCR product before restriction digestion, seven gonadal and five nongonadal GCTs, and one control. Agarose gel electrophoresis after RTPCR and restriction digestion of a polymorphic AluI restriction site. Presence of 261-bp, 219-bp, and 147-bp bands proves biallelic expression. Monoallelic expression results in either 261-bp and 219-bp bands or 261-bp and 147-bp bands. 7273 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS been demonstrated with Northern blotting, RT-PCR, and in situ hybridization experiments (54, 55). A recent study of 11 GCTs in children, adolescents, and young adults included two testicular GCTs, which both showed LOI of H19 and IGF-2 (24). Three of five ovarian GCTs showed biallelic expression of both genes, and one showed monoallelic H19 but biallelic IGF-2 expression. Among four nongonadal GCTs, only one tumor showed biallelic IGF-2 expression, and three showed biallelic H19 expression. In summary, virtually all of the postpubertal testicular GCTs showed LOI, and a majority of ovarian GCTs also showed LOI. However, the data for nongonadal GCTs are heterogeneous and do not allow determining the cellular origin of nongonadal GCTs, which would be by far more significant than in gonadal GCTs, in which the germ cell origin is more obvious. This is the focus of our study. H19 and IGF2 Allelic Expression in Gonadal and Extragonadal Germ Cell Tumors. Three conclusions can be drawn from our data on the allelic expression of H19 and IGF-2. First, compared with testicular GCTs in adults studied with the same methodology, the frequency of LOI is lower in infantile testicular GCTs, adolescent ovarian GCTs, and pediatric nongonadal GCTs. Second, the frequency of LOI is comparable in pediatric gonadal and nongonadal GCTs. Third, these data alone do not provide reliable information regarding the germ cell origin of either gonadal or nongonadal pediatric GCTs. It is remarkable, however, that we observed three female patients with monoallelic IGF-2 and biallelic H19 expression. Ross et al. (24) found two additional female patients with nongonadal GCTs with the same imprinting pattern. This constellation is unique to female patients and different from somatic tumors such as Wilms’ tumors, which show LOI of IGF-2 but epigenetic silencing of the maternally expressed H19 allele by DNA hypermethylation. The latter pattern is consistent with the boundary model of an imprinting control region that in its methylated state silences H19 and allows activation of the IGF-2 promoter by its enhancer (Fig. 1; Refs. 30, 31). This hypothesis has been substantiated recently (56) by methylation analysis of the H19 imprinting control region. Conversely, the above-mentioned constellation observed in this report and by Ross et al. (24) would rather be consistent with an unmethylated state of the imprinting control region and of the H19 promoter on both alleles, thus allowing biallelic expression of H19 and silencing of IGF-2 by binding of CTCF (Fig. 1; Refs. 30, 31). This pattern has to be established during development of female gametes. SNRPN Methylation Analysis in Gonadal and Extragonadal GCTs. In this context, the SNRPN data provide important additional information. This analysis shows loss of methylation, consistent with LOI, in the vast majority of both gonadal and nongonadal GCTs. The frequency of LOI was comparable for gonadal and nongonadal GCTs, indicating that both arise from PGCs that have erased the SNRPN imprint. Although this has to be addressed critically, we consider it unlikely that different methodologies may account for the discrepancy between the SNRPN and the IGF-2/H19 data. The assay to detect allelespecific expression of H19 and IGF-2 is well validated and has been broadly used. In addition to a DNase digestion step, this assay includes control experiments such as exclusion of RT-PCR for monitoring for contamination with genomic DNA. In addition, because the primers span two introns, the H19 RT-PCR product can be distinguished from the PCR product of genomic DNA by its shorter size. Our experimental procedure to determine SNRPN methylation is based on an assay that relies on the monoallelic methylation of one CpG dinucleotide (35). Because this site is methylated in ⬎96% of normal individuals, it is unlikely that constitutional lack of methylation substantially contributed to our results (33). In addition, our assay has been optimized by the inclusion of an internal control to monitor for incomplete restriction digestion. The reliability of our approach is further demonstrated by the analysis of control samples and by performing repeated examinations, which always yielded identical results. Bussey et al. (57) have recently presented preliminary data of SNRPN methylation of pediatric GCTs, most of which were assessed after short-term cell cultures. This analysis was based on a different experimental approach that uses methylation-dependent restriction digestion and Southern blotting. This study also found loss of methylation at the SNRPN locus, but at a somewhat lower frequency, particularly in nongonadal GCTs. In our opinion, such data must be interpreted with caution. GCTs usually grow poorly in cell culture, often resulting in contamination or overgrowth with non-neoplastic somatic cells such as fibroblasts. This is of particular concern, because the SNRPN analysis was performed on samples that were also analyzed cytogenetically, and these demonstrated a high rate of karyotypically normal infantile malignant GCTs (13 of 20 tumors; Ref. 10). These data stand in contrast to all of the other studies of malignant GCTs in infants, which show virtually all of the malignant GCTs to have cytogenetic abnormalities by conventional cytogenetics, CGH, or fluorescence in situ hybridization analysis (3, 4, 11, 58). In addition, different cell culture conditions may significantly interfere with DNA methylation (59). Summary and Conclusion. The results of the current study provide evidence that both gonadal and nongonadal GCTs share a common cell of origin, which is a PGC that has already erased the SNRPN imprint. IGF-2 and H19, which are localized in a separate chromosomal cluster than SNRPN, are regulated by a different imprinting control mechanism (30, 31, 40). Therefore, one may assume that the erasure of SNRPN methylation may occur earlier during PGC migration than the erasure of imprinting of IGF-2 and H19. The incomplete erasure of H19 and IGF-2 reported here and by Ross et al. (24) suggests that the initiation of some childhood GCTs may occur during germ cell migration, whereas the initiation of testicular GCTs in adults occurs at a later stage of PGC development. This may be one possible explanation for the profound biological differences between prepubertal and postpubertal GCTs as summarized in the introduction. Alternatively, the failure to erase the imprint of IGF-2 and H19 in a physiological pattern during PGC migration may reflect an early step of tumor development. Lastly, ovarian teratoma must be considered a distinct biological entity, because these commonly develop from an error in meiosis II resulting in isodisomy (10). Hence, it is not surprising that both ovarian teratomas showed only the methylated allele of SNRPN and monoallelic IGF-2 expression, mimicking the imprinting status of female gametes (Table 2). The data are supported by Miura et al. (22), who also reported that in ovarian teratoma, the methylation imprint of H19 and SNRPN changes as the cellular origin of the tumor advances in its development. Remarkably, we also observed one male neonate with an immature mediastinal teratoma who showed an identical methylation pattern of SNRPN, consistent with entry into meiosis. One may speculate whether the extragonadal environment may have contributed to the establishment of an aberrant female gamete-specific imprinting pattern in a male. This hypothesis is strongly supported by studies (60) of the development of extragonadal germ cells in mice, which in both sexes develop into oocytes. In conclusion, gonadal and nongonadal germ cell tumors are derived from PGCs, and therefore, the terminology “germ cell tumors” is also appropriate for nongonadal tumors. The IGF-2 and H19 imprinting pattern is to some extent different from testicular GCTs in adult patients, suggesting that pediatric GCTs arise from a different stage of germ cell development. Ovarian and rare nongonadal terato- 7274 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS mas develop from germ cells that are more advanced in their development. Future studies of imprinting control mechanisms in GCTs, as well as the timely order and biochemical mechanisms of imprint erasure and reestablishment during germ cell development, will provide important information that will eventually elucidate the early steps of GCT development. ACKNOWLEDGMENTS We thank Prof. Dr. D. Harms, Institute for Pediatric Pathology University of Kiel, Germany, for reviewing and contributing specimens from the German Children’s Tumor Registry to this analysis. We also thank all of the clinical centers contributing clinical data to the Maligne Keimzelltumaren and Pediatric Oncology Group trials for GCT in children. REFERENCES 1. Teilum, G. Classification of endodermal sinus tumour (mesoblastoma vitellinum) and so-called “embryonal carcinoma” of the ovary. Acta Pathol. Microbiol. Scand., 64: 407– 429, 1965. 2. Chaganti, R. S., Rodriguez, E., and Mathew, S. Origin of adult male mediastinal germ-cell tumours. Lancet, 343: 1130 –1132, 1994. 3. Perlman, E. J., Hu, J., Ho, D., Cushing, B., Lauer, S., and Castleberry, R. P. Genetic analysis of childhood endodermal sinus tumors by comparative genomic hybridization. J. Pediatr. Hematol. Oncol., 22: 100 –105, 2000. 4. Perlman, E. J., Cushing, B., Hawkins, E., and Griffin, C. A. Cytogenetic analysis of childhood endodermal sinus tumors: a Pediatric Oncology Group study. Pediatr. Pathol., 14: 695–708, 1994. 5. Schneider, D. T., Schuster, A. E., Fritsch, M. K., Harms, D., Göbel, U., Lauer, S., Olson, T., and Perlman, E. J. Genetic analysis of mediastinal germ cell tumors in children and adolescents. Med. Pediatr. Oncol., 35: 257, 2000. 6. Nichols, C. R., Heerema, N. A., Palmer, C., Loehrer, P. J. S., Williams, S. D., and Einhorn, L. H. Klinefelter’s syndrome associated with mediastinal germ cell neoplasms. J. Clin. Oncol., 5: 1290 –1294, 1987. 7. Hasle, H., Mellemgaard, A., Nielsen, J., and Hansen, J. Cancer incidence in men with Klinefelter syndrome. Br. J. Cancer, 71: 416 – 420, 1995. 8. Chaganti, R. S., and Houldsworth, J. Genetics and biology of adult human male germ cell tumors. Cancer Res., 60: 1475–1482, 2000. 9. Riopel, M. A., Spellerberg, A., Griffin, C. A., and Perlman, E. J. Genetic analysis of ovarian germ cell tumors by comparative genomic hybridization. Cancer Res., 58: 3105–3110, 1998. 10. Bussey, K. J., Lawce, H. J., Olson, S. B., Arthur, D. C., Kalousek, D. K., Krailo, M., Giller, R., Heifetz, S., Womer, R., and Magenis, R. E. Chromosome abnormalities of eighty-one pediatric germ cell tumors: sex-, age-, site-, and histopathology-related differences–a Children’s Cancer Group study. Genes Chromosomes Cancer, 25: 134 –146, 1999. 11. Mostert, M., Rosenberg, C., Stoop, H., Schuyer, M., Timmer, A., Oosterhuis, W., and Looijenga, L. Comparative genomic and in situ hybridization of germ cell tumors of the infantile testis. Lab. Investig., 80: 1055–1064, 2000. 12. Witschi, E. Migration of the germ cells of human embryos from the yolk sac to the primitive gonadal folds. Contr. Embryol. Carnegie Inst., 32: 67– 80, 1948. 13. Anderson, R., Copeland, T. K., Scholer, H., Heasman, J., and Wylie, C. The onset of germ cell migration in the mouse embryo. Mech. Dev., 91: 61– 68, 2000. 14. Wylie, C. Germ cells. Cell, 96: 165–174, 1999. 15. Godin, I., Deed, R., Cooke, J., Zsebo, K., Dexter, M., and Wylie, C. C. Effects of the steel gene product on mouse primordial germ cells in culture. Nature (Lond.), 352: 807– 809, 1991. 16. Chiquoine, A. D. The identification, origin, and migration of the primordial germ cell in the mouse embryo. Anat. Rec., 118: 135–146, 1954. 17. Pesce, M., Farrace, M. G., Piacentini, M., Dolci, S., and De Felici, M. Stem cell factor and leukemia inhibitory factor promote primordial germ cell survival by suppressing programmed cell death (apoptosis). Development (Camb.), 118: 1089 –1094, 1993. 18. Göbel, U., Schneider, D. T., Calaminus, G., Haas, R. J., Schmidt, P., and Harms, D. Germ-cell tumors in childhood and adolescence. Ann. Oncol., 11: 263–271, 2000. 19. Gale, K. B., Ford, A. M., Repp, R., Borkhardt, A., Keller, C., Eden, O. B., and Greaves, M. F. Backtracking leukemia to birth: identification of clonotypic gene fusion sequences in neonatal blood spots. Proc. Natl. Acad. Sci. USA, 94: 13950 – 13954, 1997. 20. Wiemels, J. L., Cazzaniga, G., Daniotti, M., Eden, O. B., Addison, G. M., Masera, G., Saha, V., Biondi, A., and Greaves, M. F. Prenatal origin of acute lymphoblastic leukaemia in children. Lancet, 354: 1499 –1503, 1999. 21. Looijenga, L. H., Verkerk, A. J., Dekker, M. C., van Gurp, R. J., Gillis, A. J., and Oosterhuis, J. W. Genomic imprinting in testicular germ cell tumours. APMIS, 106: 187–195, 1998. 22. Miura, K., Obama, M., Yun, K., Masuzaki, H., Ikeda, Y., Yoshimura, S., Akashi, T., Niikawa, N., Ishimaru, T., and Jinno, Y. Methylation imprinting of H19 and SNRPN genes in human benign ovarian teratomas. Am. J. Hum. Genet., 65: 1359 –1367, 1999. 23. Ueda, T., Abe, K., Miura, A., Yuzuriha, M., Zubair, M., Noguchi, M., Niwa, K., Kawase, Y., Kono, T., Matsuda, Y., Fujimoto, H., Shibata, H., Hayashizaki, Y., and Sasaki, H. The paternal methylation imprint of the mouse H19 locus is acquired in the gonocyte stage during foetal testis development. Genes Cells, 5: 649 – 659, 2000. 24. Ross, J. A., Schmidt, P. T., Perentesis, J. P., and Davies, S. M. Genomic imprinting of H19 and insulin-like growth factor-2 in pediatric germ cell tumors. Cancer (Phila.), 85: 1389 –1394, 1999. 25. Kerjean, A., Dupont, J. M., Vasseur, C., Le Tessier, D., Cuisset, L., Paldi, A., Jouannet, P., and Jeanpierre, M. Establishment of the paternal methylation imprint of the human H19 and MEST/PEG1 genes during spermatogenesis. Hum. Mol. Genet., 9: 2183–2187, 2000. 26. Tilghman, S. M. The sins of the fathers and mothers: genomic imprinting in mammalian development. Cell, 96: 185–193, 1999. 27. Constancia, M., Pickard, B., Kelsey, G., and Reik, W. Imprinting mechanisms. Genome Res., 8: 881–900, 1998. 28. Feinberg, A. P. Imprinting of a genomic domain of 11p15 and loss of imprinting in cancer: an introduction. Cancer Res., 59 (Suppl.): 1743s–1746s, 1999. 29. Kondo, M., Suzuki, H., Ueda, R., Osada, H., Takagi, K., Takahashi, T., and Takahashi, T. Frequent loss of imprinting of the H19 gene is often associated with its overexpression in human lung cancers. Oncogene, 10: 1193–1198, 1995. 30. Hark, A. T., Schoenherr, C. J., Katz, D. J., Ingram, R. S., Levorse, J. M., and Tilghman, S. M. CTCF mediates methylation-sensitive enhancer-blocking activity at the H19/Igf2 locus. Nature (Lond.), 405: 486 – 489, 2000. 31. Bell, A. C., and Felsenfeld, G. Methylation of a CTCF-dependent boundary controls imprinted expression of the Igf2 gene. Nature (Lond.), 405: 482– 485, 2000. 32. Constancia, M., Dean, W., Lopes, S., Moore, T., Kelsey, G., and Reik, W. Deletion of a silencer element in igf2 results in loss of imprinting independent of H19. Nat. Genet., 26: 203–206, 2000. 33. Zeschnigk, M., Schmitz, B., Dittrich, B., Buiting, K., Horsthemke, B., and Doerfler, W. Imprinted segments in the human genome: different DNA methylation patterns in the Prader-Willi/Angelman syndrome region as determined by the genomic sequencing method. Hum. Mol. Genet., 6: 387–395, 1997. 34. Zeschnigk, M., Lich, C., Buiting, K., Doerfler, W., and Horsthemke, B. A single-tube PCR test for the diagnosis of Angelman and Prader-Willi syndrome based on allelic methylation differences at the SNRPN locus. Eur. J. Hum. Genet., 5: 94 –98, 1997. 35. Velinov, M., Gu, H., Genovese, M., Duncan, C., Brown, W. T., and Jenkins, E. The feasibility of PCR-based diagnosis of Prader-Willi and Angelman syndromes using restriction analysis after bisulfite modification of genomic DNA. Mol. Genet. Metab., 69: 81– 83, 2000. 36. Rodriguez, E., Mathew, S., Reuter, V., Ilson, D. H., Bosl, G. J., and Chaganti, R. S. Cytogenetic analysis of 124 prospectively ascertained male germ cell tumors. Cancer Res., 52: 2285–2291, 1992. 37. Rainier, S., Dobry, C. J., and Feinberg, A. P. Loss of imprinting in hepatoblastoma. Cancer Res., 55: 1836 –1838, 1995. 38. Tadokoro, K., Fujii, H., Inoue, T., and Yamada, M. Polymerase chain reaction (PCR) for detection of ApaI polymorphism at the insulin like growth factor II gene (IGF2). Nucleic Acids Res., 19: 6967, 1991. 39. van Gurp, R. J., Oosterhuis, J. W., Kalscheuer, V., Mariman, E. C., and Looijenga, L. H. Biallelic expression of the H19 and IGF2 genes in human testicular germ cell tumors. J. Natl. Cancer Inst. (Bethesda), 86: 1070 –1075, 1994. 40. Shemer, R., Hershko, A. Y., Perk, J., Mostoslavsky, R., Tsuberi, B., Cedar, H., Buiting, K., and Razin, A. The imprinting box of the Prader-Willi/Angelman syndrome domain. Nat. Genet., 26: 440 – 443, 2000. 41. Szabo, P. E., and Mann, J. R. Biallelic expression of imprinted genes in the mouse germ line: implications for erasure, establishment, and mechanisms of genomic imprinting. Genes Dev., 9: 1857–1868, 1995. 42. Jouvenot, Y., Poirier, F., Jami, J., and Paldi, A. Biallelic transcription of Igf2 and H19 in individual cells suggests a post-transcriptional contribution to genomic imprinting. Curr. Biol., 9: 1199 –1202, 1999. 43. Lerchner, W., and Barlow, D. P. Paternal repression of the imprinted mouse Igf2r locus occurs during implantation and is stable in all tissues of the post-implantation mouse embryo. Mech. Dev., 61: 141–149, 1997. 44. Zhan, S., Zhang, L., Van, M., Young, C., and Helman, L. J. Biallelic expression of all four IGF-II promoters and its association with increased methylation of H19 gene in human brain. Brain Res., 792: 283–290, 1998. 45. Rainier, S., Johnson, L. A., Dobry, C. J., Ping, A. J., Grundy, P. E., and Feinberg, A. P. Relaxation of imprinted genes in human cancer. Nature (Lond.), 362: 747–749, 1993. 46. Ogawa, O., Eccles, M. R., Szeto, J., McNoe, L. A., Yun, K., Maw, M. A., Smith, P. J., and Reeve, A. E. Relaxation of insulin-like growth factor II gene imprinting implicated in Wilms’ tumour. Nature (Lond.), 362: 749 –751, 1993. 47. Steenman, M. J., Rainier, S., Dobry, C. J., Grundy, P., Horon, I. L., and Feinberg, A. P. Loss of imprinting of IGF2 is linked to reduced expression and abnormal methylation of H19 in Wilms’ tumour (Published erratum in Nat. Genet., 8: 203, 1994). Nat. Genet., 7: 433– 439, 1994. 48. Cui, H., Horon, I. L., Ohlsson, R., Hamilton, S. R., and Feinberg, A. P. Loss of imprinting in normal tissue of colorectal cancer patients with microsatellite instability. Nat. Med., 4: 1276 –1280, 1998. 49. Takano, Y., Shiota, G., and Kawasaki, H. Analysis of genomic imprinting of insulinlike growth factor 2 in colorectal cancer. Oncology (Basel), 59: 210 –216, 2000. 50. Kim, K. S., and Lee, Y. I. Biallelic expression of the H19 and IGF2 genes in hepatocellular carcinoma. Cancer Lett., 119: 143–148, 1997. 51. el Naggar, A. K., Lai, S., Tucker, S. A., Clayman, G. L., Goepfert, H., Hong, W. K., and Huff, V. Frequent loss of imprinting at the IGF2 and H19 genes in head and neck squamous carcinoma. Oncogene, 18: 7063–7069, 1999. 52. Nishihara, S., Hayashida, T., Mitsuya, K., Schulz, T. C., Ikeguchi, M., Kaibara, N., and Oshimura, M. Multipoint imprinting analysis in sporadic colorectal cancers with and without microsatellite instability. Int. J. Oncol., 17: 317–322, 2000. 53. Hashimoto, K., Azuma, C., Kamiura, S., Koyama, M., Nobunaga, T., Tokugawa, Y., Kimura, T., Kubota, Y., Sawai, K., and Saji, F. Maintenance of imprinting of the 7275 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. IMPRINTING ANALYSIS OF PEDIATRIC GERM CELL TUMORS insulin-like growth factor II gene (IGF2) and the small nuclear ribonucleoprotein polypeptide N gene (SNRPN) in the human uterus and leiomyoma. Gynecol. Obstet. Investig., 41: 50 –54, 1996. 54. Verkerk, A. J., Ariel, I., Dekker, M. C., Schneider, T., van Gurp, R. J., de Groot, N., Gillis, A. J., Oosterhuis, J. W., Hochberg, A. A., and Looijenga, L. H. Unique expression patterns of H19 in human testicular cancers of different etiology. Oncogene, 14: 95–107, 1997. 55. Engstrom, W., Hopkins, B., and Schofield, P. Expression of growth regulatory genes in primary human testicular neoplasms. Int. J. Androl., 10: 79 – 84, 1987. 56. Cui, H., Niemitz, E. L., Ravenel, J. D., Onyango, P., Brandenburg, S. A., Lobanenkov, V. V., and Feinberg, A. P. Loss of imprinting of insulin-like growth factor-II in Wilms’ tumor commonly involves altered methylation but not mutations of CTCF or its binding site. Cancer Res., 61: 4947– 4950, 2001. 57. Bussey, K. J., Lawce, H. J., Olson, S. B., Shu, X. O., Perlman, E., and Magenis, R. E. Determining the imprinting stage of germ cell tumors by SNRPN methylation patterns. Eighth International Workshop on Chromosomes in Solid Tumors, 46: (abstract 46), 2000. 58. Stock, C., Ambros, I. M., Lion, T., Haas, O. A., Zoubek, A., Gadner, H., and Ambros, P. F. Detection of numerical and structural chromosome abnormalities in pediatric germ cell tumors by means of interphase cytogenetics. Genes Chromosomes Cancer, 11: 40 –50, 1994. 59. Doherty, A. S., Mann, M. R., Tremblay, K. D., Bartolomei, M. S., and Schultz, R. M. Differential effects of culture on imprinted H19 expression in the preimplantation mouse embryo. Biol. Reprod., 62: 1526 –1535, 2000. 60. Upadhyay, S., and Zamboni, L. Ectopic germ cells: natural model for the study of germ cell sexual differentiation. Proc. Natl. Acad. Sci. USA, 79: 6584 – 6588, 1982. 7276 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research. Multipoint Imprinting Analysis Indicates a Common Precursor Cell for Gonadal and Nongonadal Pediatric Germ Cell Tumors Dominik T. Schneider, Amy E. Schuster, Michael K. Fritsch, et al. Cancer Res 2001;61:7268-7276. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/61/19/7268 This article cites 58 articles, 17 of which you can access for free at: http://cancerres.aacrjournals.org/content/61/19/7268.full.html#ref-list-1 This article has been cited by 15 HighWire-hosted articles. Access the articles at: /content/61/19/7268.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 2001 American Association for Cancer Research.