Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
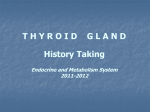
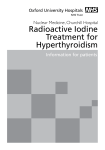
How To Decide Which Is The Best Therapy Option For Hyperthyroid Patients: Guidance For The Practicing General Radiologist and Nuclear Medicine Physician European Society of Radiology ESR 2011 Annual Meeting in Vienna, AT March 3-7, 2011 Educational Exhibit, ID Number: 5722 **** B Rodgers, MD University of Southern California, Los Angeles, CA Disclosure of Commercial Interest Neither I nor my immediate family members have a financial relationship with a commercial organization that may have a direct or indirect interest in the content. Learning Objectives After reviewing this presentation, General Radiologists and Nuclear Medicine Physicians should feel comfortable: 1. Discussing various modes of therapy for hyperthyroid patients. These include medical - pharmacologic management, surgery, and radionuclide therapy with 131 - Iodine 2. Working with Clinicians who refer hyperthyroid patients for radionuclide therapy 3. Taking the lead role in managing hyperthyroid patients, especially in locations where specialists in thyroid disease are not available. This will provide a highly valuable patient service. Background Information: Many physicians are not comfortable treating and managing patients with hyperthyroidism. In many parts of the world, physicians highly trained in the diagnosis and treatment of thyroid disease are not readily available, if at all. Even in the US, many areas do not have adequate Endocrine Medicine nor Nuclear Medicine / Radiologist coverage. In this light, we hope to educate General Radiologists and Nuclear Physicians about the treatment of hyperthyroid patients. In many parts of the world, Radiologists would have to treat these patients. Various options and methods will be reviewed in light of evidence based medicine. Only the treatment of Graves (diffuse, non-focal) hyperthyroidism will be reviewed in this presentation. For further information please contact: Brian Rodgers, M.D. LAC + USC Medical Center 1200 North State Street, D&T 3D321 Los Angeles, CA 90033 323 409 7257 via Residency program Co-ordinator [email protected] personal email This material is presented for the sole purpose of educating the reader and is not intended for copying nor downloading. Please contact the author if you wish copies of portions of this exhibit. Imaging Findings or Procedure This exhibit will review: - Clinical and biochemical identification of hyperthyroid patients - The differential diagnosis of hyperthyroidism - Types of hyperthyroidism - Imaging of hyperthyroid patients - Treatment options and their expected outcomes - How to assist in managing hyperthyroid patients both during medical therapy and after 131 - Iodine therapy - Links to more detailed procedural, informed consent, and regulatory information Also included are multiple examples of how to perform dose calculations (often an area of confusion to those unfamiliar with therapy) using example cases. Other information on practice patterns is also included. Example Case – Why We Need To Know How To Manage These Cases and a Great Case For Board Exams 17 year old female that has a 3 month history of: 10 lb weight loss/month Palpatations Muscle weakness Insomnia She weighs 73 kgs or 160 lbs and is 1.73 m or 5’8” tall. HR: 88 BP:130/90 The primary care provider asks you in the elevator what should be done to work up this patient. What do you suggest and why? Let’s Begin – With the Conclusion Remember: General Radiologists can be valuable members of a team treating and caring for patients with hyperthyroidism. Once you understand the principles (which follow), the following will seem like common sense: - Treat each patient individually based upon severity of hyperthyroidism when they present to you. This means offering patients with severe signs and symptoms a higher dose of 131-I and those patients with lower levels of clinical disease a more moderate dose. Low dose therapy might be reserved for patients with minor signs and symptoms and/or for those in whom maintaining euthyroidism is thought to be very important. The actual doses used can be based on the methodologies explained in the slides which follow. See table on the next page. 131-I Dosing Recommendations Low Dose 250 MBq 7 mCi Finnish method, others ~66-80% Tx success ~20-33% Tx failure Average Dose ~370-555 MBq ~15 mCi (typically ~10-15 mCi) ~1100 MBq Up to 29 mCi Based on Michigan, UK NHS, and Mass Gen’l methodologies ~ 85% ~15 % Tx success Tx failure Tx dose based on severe signs and / or symptoms Expect almost 100% tx success High Dose For Tx of Hypercomparison: tensive pts Only 1/3 tx success About 2/3 fail tx Remember tx success is often defined in the literature as those pts who become euthyroid or hypothyroid after tx. (Tx = treatment or therapy) Basic Principles of Pathophysiology These are reviewed elsewhere and are beyond the scope of this exhibit. Many Internal Medicine textbook chapters cover this well. Internet search engines will also yield well written web and journal articles, such as this one: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1787885&blobtype=pdf G. Davies, Thyroid Physiology, Scientific Basis of Clinical Practice, Medical Practice, BMJ: 1972 (2): 22 April 1972, pp 206-9. What concerns us here is when thyroid hormone overproduction is due to Graves’ Disease. TSH regulates thyroid hormone production. Graves Hyperthyroidism may be associated with elevated levels of TSH. However, long active thyroid stimulator (LATS) can also play a role. Incidence: Graves Disease is the most common etiology for hyperthyroidism in the US. It is an immune mediated / auto-immune disease process. It is 7 times more common in women than men. It is also more common over age 20. http://www.mayoclinic.com/health/graves-disease/DS00181 http://www.endocrineweb.com/hyper1.html Part 1: Clinical and Biochemical Identification of Hyperthyroid Patients Common signs and symptoms suggesting hyperthyroidism may include: Anxiety, disturbance of sleep patterns, fatigue, weight loss, increased perspiration, feeling hot, tacchycardia, fine tremor, change in menstrual cycle, blurred vision, and, exopthalmos. Levels of free and bound T3 and T4, along with TSH and anti-thyroid antibodies might need to checked as part of assessing patients with clinical hyperthyroidism. Thyroid-peroxidase antibodies (TPA) are elevated in 75% of Graves' disease patients. TPA is a marker of thyroid autoimmune activity. Nuclear medicine 4 and 24 hour uptake and scan are also used for this purpose. “In Graves' disease, your immune system mistakenly attacks your thyroid gland, but instead of destroying the gland, an antibody called thyrotropin receptor antibody (TRAb) stimulates the thyroid to make excessive amounts of thyroid hormone. “ http://www.mayoclinic.com/health/graves-disease/DS00181/METHOD=print and http://www.medifocushealth.com/ND004/Diagnosis-of-Graves-Disease_Diagnostic-Testing-for-GravesDisease.php Common Clinical Findings In Hyperthyroid Patients The following can found in Graves Disease. However, the same findings can also be seen in Toxic Multinodular Goitre, along with other causes; please see Part 2 of this exhibit for differential diagnosis. “Common symptoms and signs of hyperthyroidism: http://www.endocrineweb.com/hyper1.html Palpitations Fatigue Heat intolerance Fast heart rate Nervousness Trembling hands Insomnia Weight loss Breathlessness Muscle weakness Increased bowel movements Warm moist skin Light or absent menstrual Hair loss periods Staring gaze” Biochemical Identification of Hyperthyroid Patients Work up for suspected hyperthyroidism: -measure the thyrotropin (TP) and free thyroxine (F TX): -if both are normal, the patient is not hyperthyroid -low TP; normal F TX – measure the serum free triiodothyronine (F T3), if that is normal, consider subclinical hyperthyroidism such as early Graves Disease or Toxic nodular goitre. Excess or surreptitious use of T4 (as in the example case) can also do this. Illness not from the thyroid also possible. Synthroid ® is the trade name of T4 thyroid hormone commonly used in the US, made by Abbott Laboratories. Unlike many prescription medications, many physicians prefer the use of Synthroid over generic medication. From 2008 package insert Consider repeating these labs in 2-3 months with annual follow up if findings do not progress. -low TP; high F TX –hyperthyroid patient or if the F T3 is high (with NL F TX) T3 hyperthroidism. Here the differential diagnosis includes: Graves Disease; Toxic nodular goitre, including adenomas; thyroiditis; excess or surreptitious use of T4; gestational hyperthyroidism; thyroid cancer; struma ovarii; chorionic gonadotropin secreting tumors; Albright’s syndrome, and familial non-auto immune hyperthyroidism. -Nl or high TP and high F TX: consider a thryrotropin secreting adenoma of the pituitary gland or thyroid hormone resistance syndrome. suggested from: Anthony P. Weetman, M.D., D.Sc., Graves' Disease, NEJM, 343:1236-1248, October 26, 2000. Parts 2 and 3: Differential Diagnosis and Types of Hyperthyroidism Graves Disease / Hyperthyroidism needs to be separated from other etiologies for hyperthyroidism. If the thyroid gland is nodular on physical exam, ultrasound, and /or nuclear scan: --single nodule, consider autonomously functioning thyroid nodule (AFTN) or Plummer’s Disease (NB: Plummer did not distinguish between AFTN and TMNG in his original 1913 paper). --multiple nodules, consider toxic multi-nodular goitre (TMNG) These can be treated somewhat differently than Graves Disease and are therefore not discussed further here. The signs and symptoms for Graves Disease are non-specific, therefore we must also exclude: anxiety, surreptitious use of thyroid hormone, other drug abuse, some types of drug or medication withdrawal, pheochromocytoma, auto-immune thyroiditis – including Hashimoto’s thyroiditis, infection in the thyroid bed, signs of menopause, myopathy, and hypoglycemia. Both Hashimoto and Graves patients may have enlarged tender glands and have thyroid peroxidase antibodies. http://www.medifocushealth.com/ND004/Diagnosis-of-GravesDisease_Differential-Diagnosis-of-Graves-Disease.php Part 4: Imaging of Hyperthyroid Patients Ultrasound can be used to assess for nodularity either apparent or not apparent on physical exam and to find solid and cystic masses. When present, such nodules may require further assessment; for example, via fine needle aspiration (FNA). CT and MRI may find abnormalities of the thyroid gland on neck, chest, cardiac, or spine exams. However, the use of iodinated CT contrast may delay the use of nuclear imaging and / or therapy by 4-8 weeks, due to saturating the thyroid follicular cells with iodine. Nuclear imaging is usually performed about 4 hours post ingestion of 123-I or about 10 min post injection of TcO4. Grave’s patients demonstrate even uptake throughout the thyroid gland without hot spots nor cold defects. Uptake measurements are usually made at 4 and 24 hours post ingestion of 131-I or 123-I. Normal uptake values are 5-15% and 10-30% respectively. These values can also help support the diagnosis of clinically suspected Graves Disease – or even support the likelihood of an alternative diagnosis, such as Hashimoto’s Thyroiditis. However, the relative values obtained at 4 and 24 hours are often not similar. Most practices in the US which use an iodine uptake value as part of calculating a therapy dose, use the 24 hour value. For Graves patients, this is often around 40% in the authors practice; though numbers may vary widely (35-70%) around the world. Imaging of Hyperthyroid Patients – 2 Nuclear Medicine and Radiation Dose Information Nuclear medicine imaging of the thyroid is commonly done via 1 of 3 methods. Both uptake and scan are commonly performed at the same time using: both 131-I (for uptake) and 99m TcO4 (for scan). Lower cost method (but higher radiation dose to the patient). 123-I (for both uptake and scan). Higher cost, lower radiation dose method. 99m TcO4 washout (for both uptake and scan). Unlike the above, not commonly used. Poor reproducibility. 131-I (for uptake) and 99m TcO4 (for scan): Technetium is used for imaging; typically 185-370 MBq, 5-10 mCi. The very small amount of 131-I, about 0.2 MBq or 5 micro (µ) Ci, is roughly at the lower range of utility of the well counter used to check doses. However, the radiation dose from 131-I is quite high: Dose rate at 1m from 37 MBq or 1 mCi = 2.20 mSv/hr (~2.2 mGy). 123-I uptake and scan. Typical dose is about 12.3 MBq = 350 µCi or 1/3 mCi. 131-I ~1 rad/ µCi = 270 mGy/mBq 123-I ~1 rad/100 µCi, or 1% of the 131-I dose. (since about 70 x more µCi used, dose reduction is a minimum of about 30%. However, β particles of 131-I are more energetic than gammas or 123-I.) 99m TcO4 ~1 rad/5000uCi, or 1/5000th the 131-I dose Part 5: Treatment Options and Their Expected Outcomes 1. No TX, XRT, Surgery No Tx: The natural history of Graves Hyperthyroidism is for the thyroid to eventually “burn itself out”. However, this can exact a great toll on the body before this occurs. Cardiac and other effects can be debilitating and require alterations of lifestyle. For most patients, doing nothing is the worst option. External Beam Radiation Therapy (XRT): Was used many years ago as a primary therapy for hyperthyroidism. However, like surgery, XRT is rarely used as a primary therapy for Graves hyperthyroidism today. Surgery could be considered as a primary Graves therapy when significant tracheal compromise due to marked thyroid gland enlargement is present. Perhaps its one advantage over other any other therapy approach is the immediate removal of thyroid hormone reserves. (Circulating hormones have a half life of about 1 week and cannot be removed). Yet, at least 1 recent study found that this only cured ~90+% (reason for such a low cure rate not given, but might be due to the surgeon leaving significant tissue behind). Laurberg P. TSH-receptor autoimmunity in Graves’ disease after therapy with anti-thyroid drugs, surgery, or radioiodine: a 5-year prospective randomized study. European Journal of Endocrinology (2008) 158 69–75. Treatment Options and Their Expected Outcomes – 2 2. Surgery and Medical TX Success rate by surgical therapy will likely be directly related to the experience of the surgeon. Those that “commonly” perform thyroidectomies should get excellent results. Regardless of method used, patients with cardiac symptoms are often first placed on β blocker therapy, such as propranolol (dose range varies, but 20-80 mg/day PO in divided doses would be common). In Europe, medical therapy is most common. This works by preventing production of new thyroid hormone-but there is no effect on hormone already in the thyroid gland. These medications are usually not expensive. The most commonly used anti-thyroid drugs include: -Methimazole (MMI) or Tapazole, qD. Easiest to use due to single daily dose, works quickly, and side effects (at low dose) are less common. It may take 6 weeks for patient to reach a normal T4 value; often 8 weeks with PTU. It takes a long time to reduce the circulating amount of thyroid hormone due the thyroid gland’s large reserves. http://www.medifocushealth.com/ND004/Treatment-Options-for-Graves-Disease_Drug-Therapy-for-Graves-Disease.php, http://www.medifocushealth.com/ND004/Treatment-Options-for-Graves-Disease_Drug-Therapy-for-Graves-Disease2.php Treatment Options and Their Expected Outcomes – 3, Medical TX -Propylthiouracil (PTU), tid. For people who cannot tolerate MMI. Also less likely to cross placenta and less likely to be part of breast milk. -Carbimazole, commonly used in Europe, but not available in the US. MMI and PTU can be given either: Short term - to prepare the patient for another treatment such as surgery or radioiodine treatment Long term - for definitive treatment of Graves' disease. Having patients on medication for over a year is not unusual. Yet, even here 60% of patients may fail after 2 years of medical therapy. Remission rate appears to be higher if thyroid antibody levels fall. “If levels of TSH receptor antibodies are normal at 6 months post treatment, the rate of relapse is approximately 8-10%.” http://www.medifocushealth.com/ND004/Treatment-Options-for-Graves-Disease_DrugTherapy-for-Graves-Disease.php, http://www.medifocushealth.com/ND004/Treatment-Options-for-Graves-Disease_DrugTherapy-for-Graves-Disease2.php Treatment Options and Their Expected Outcomes – 4, Medical TX However, medical therapy only yields a medium to long term remission in 2590% of patients. The wide range of results here may be due to duration of use of medications. Lucas A. Medical Therapy of Graves’ Disease: Does Thyroxine Prevent Recurrence of Hyperthyroidism? The Journal of Clinical Endocrinology & Metabolism 1997, 82:8, 2410-2413. and Raber W. Medical therapy of Graves’ disease: effect on remission rates of methimazole alone and in combination with triiodothyronine. European Journal of Endocrinology (2000) 142 117–124. Disadvantages of medical therapy: permanent cure is not likely; patients must take meds for a year or more; some patients have significant side effects from the meds (for example, PTU induced liver failure, reported from the US Food and Drug Administration (FDA) in June 2009) FDA ALERT [06/04/2009]: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ DrugSafetyInformationforHeathcareProfessionals/ucm162701.htm Case 1 Small masses seen at CT not noted on planar thyroid scan. This is a 43 year old male with a diagnosis of small thyroid masses by CT and Hyperthyroidism secondary to Graves disease and has failed medical therapy with PTU. The patient has persistently elevated LFT’s. Please see FDA advisory on PTU induced liver failure (6/4/2009). Surgery was advised in order to exclude any malignancy in the thyroid masses. 10-30% He was scheduled for a total thyroidectomy. In selected pts including those with both thyroid masses (or goiter) and Graves Disease, this can be the optimal tx. Post operatively the patient has been doing well and taking Synthroid and Calcium supplementation. Case 1 This is a 43 year old male with a diagnosis of small thyroid masses by CT and Hyperthyroidism secondary to Graves disease and has failed medical therapy with PTU. The patient has persistently elevated LFT’s. Please see the FDA advisory on PTU induced liver failure (6/4/2009). Surgery was advised in order to exclude any malignancy in the thyroid masses. This case highlights the fact that not all patients should be offered the same treatment. This patients has 3 major issues: thyroid masses, Graves Disease, and a reaction to medical therapy for Graves Disease. The patient did not wish to have multiple fine needle aspirations (FNAs) to assess his multiple thyroid nodules for possible cancer, due to discomfort and the chance of a false negative cytology result. Also, surgery can “cure” both any local malignancy (via thyroidectomy and compartmental lymph node dissection) and his Graves Disease at the same time. He had a bad experience with medical therapy too. He simply wanted to be “done with it”. He was scheduled for a total thyroidectomy. In selected pts including those with both thyroid masses (or goiter) and Graves Disease, this can be the optimal tx. Post operatively the patient has been doing well and taking Synthroid and Calcium supplementation. Treatment Options and Their Expected Outcomes – 5 Variance of Practice Patterns Standards of practise vary around the world. For example, as noted in a study from Germany, medical therapy for hyperthyroidism is tried first. Patients had to be over 30 years old to be eligible for 131-I therapy. In patients 30-40 years old, failure of either medical therapy or surgery had to occur before using 131-I. In patients over 40 years old 131-I could be a primary therapy for hyperthyroidism. In this paper treatment success was the elimination of hyperthyroidism, regardless of how many patients were made hypothyroid due to treatment. H. PETERS, C. FISCHER, U. BOGNER, C. REINERS H. SCHLEUSENER , Radioiodine therapy of Graves' hyperthyroidism: standard vs. calculated 131 iodine activity. Results from a prospective, randomized, multicentre study. European Journal of Clinical Investigation 1995, 25:3,186 - 193. Although it is uncommon to use 131-I for children and young adults as the standard of care in Germany, in the US, even children are treated with 131-I. There was a dose dependent success rate in this study from Yale. For example, 8.14 MBq/g = 220 µCi/g or 200 Gy yielded hypothyroidism in 70% at 1 year. Rivkees SA and Cornelius EA. Influence of Iodine-131 Dose on the Outcome of Hyperthyroidism In Children. Pediatrics 2003; 111; 745-749. Practice patterns in the US are often determined by the methods learned in residency and local expertise. Thus, even in the US, treatment methods for hyperthyroidism may vary greatly – even in the same city. Treatment Options and Their Expected Outcomes – 6 Some Areas of Controversy The potential need for using a b blocker, such as propranolol, is common to all forms of therapy. This may provide symptomatic relief for cardiac issues. In the US and UK, iodine deficient diets are not common. But elsewhere in the world this may not be the case. In iodine deficient patients, the 131-I dose may need adjusting. Patients from regions of low iodine availability may have larger glands. Controversies persist regarding when to discontinue use of anti thyroid medication (ATM) -both in general and before use of 131-I therapy; how much ATM to use; dose of 131-I; risk and effect of mild post treatment hyperthyroidism. A recent Swedish study did randomize patients with hyperthyroidism to surgery, medical therapy, and 131-I. But the purpose of this study was to assess thyroid antibody levels post treatment and their potential effects on the patients. At 4 years follow up, under 10% of the surgically treated group remained hyperthyroid. In the medically treated group, about 40% remained hyperthyroid at 4 years, as did 21% treated with 131-I. Of course, all of these results are influenced by the details of the therapeutic regimens used. Laurberg P. TSH-receptor autoimmunity in Graves’ disease after therapy with antithyroid drugs, surgery, or radioiodine: a 5-year prospective randomized study. European Journal of Endocrinology (2008) 158 69–75. Case 2 This is a 35 year old female with a history of infertility and progressive symptoms of hair loss, fatigue, palpitations, heat intolerance, and a pruritic rash. Patient wishes to have a child. The patient was placed on PTU and had a reaction to it. So, for this patient optimal therapy would be surgical or methimazole treatment. 131-I is less optimal as the patient would be advised not to begin a family in the year following tx. Treatment Options and Their Expected Outcomes – 7 131-Iodine 131-I has been used in the treatment of hyperthyroidism since around 1941. CLARK T. SAWIN, DAVID V. BECKER, Radioiodine and the Treatment of Hyperthyroidism: The Early History. Thyroid. April 1997, 7(2): 163-176. However, early access to 131-I was limited to Berkeley, California, and the area near MIT in Boston. Wider use outside the academic setting only occurred by the 1960s. Concerns about 131-I causing cancer have been allayed in multiple studies. However, a slight increase in some cancers, whether due to the hyperthyroidism itself or due to 131-I or anti thyroid medications has been noted. The reasons for this remain unclear. Cooper, DS. Radioiodine for Hyperthyroidism Where Do We Stand After 50 Years? JAMA: 280, 4: 375-6, 1998 The low cost of 131-I, its low morbidity, few side effects, and the potential for a very high success rate favor its use. Use of 131-I is also considered safe in patients reporting iodine allergy, due to the miniscule amount of radioactive iodine present; 0.05-0.18 µg. Average daily intake, >150 µg/day. Royal College of Physicians. Radioiodine in the management of benign thyroid disease: clinical Guidelines. Report of a Working Party. London: RCP, 2007 The only absolute contraindications for 131-I use are pregnancy and breast feeding. Treatment Options and Their Expected Outcomes – 8 Graves Disease and Ophatlmopathy Controversy remains regarding 131-I therapy possibly worsening Graves Opthalmopathy. However, it is possible that hyperthyroidism and opthalmopathy run somewhat separate and independent courses, thought both may occur via auto-immune processes. Weetman, in referencing others notes concern for those with pre existing opthalmopathy or even causing it. Anthony P. Weetman CLINICAL PRACTICE UPDATE Radioiodine treatment for benign thyroid diseases Clinical Endocrinology 2007, 66:6, 757-764. This risk may be 4 X more likely in smokers. Although, this might be 1 factor favoring medical therapy in Europe, in the US there is no established practice pattern in this regard. Steroid protocol is given in Weetman’s article on p. 760. The RCP White Paper, suggests using ATDs and not 131-I therapy in newly diagnosed Graves’ patients with active opthalmopathy. Royal College of Physicians. Radioiodine in the management of benign thyroid disease: clinical Guidelines. Report of a Working Party. London: RCP, 2007 Treatment Options and Their Expected Outcomes – 9 Special Considerations: Children (131-I vs Surgery) and Dialysis Patients (Reduced Dose of 131-I) In pediatric Graves patients, most seem to favor 131-I therapy, though surgery is still advocated by some, even in the recent literature. as noted in: Anthony P. Weetman CLINICAL PRACTICE UPDATE Radioiodine treatment for benign thyroid diseases Clinical Endocrinology. 2007, 66:6, 757-764. Lucignani notes that some still believe that surgery is more ideal for pediatric hyperthyroid therapy. However, local expertise will usually decide which type of treatment will be used. Giovanni Lucignani Long-term risks in hyperthyroid patients treated with radioiodine: is there anything new? Eur J Nucl Med Mol Imaging (2007) 34:1504–1509, quoting a group in San Francisco, James A. Lee, Melvin M. Grumbach, and Orlo H. Clark CONTROVERSY IN CLINICAL ENDOCRINOLOGY The Optimal Treatment for Pediatric Graves’ Disease Is Surgery The Journal of Clinical Endocrinology & Metabolism 92(3):801–803 In dialysis patients the dose of 131-I needs to be greatly reduced; perhaps only using 1/7-1/4 the normal dose. Jennifer P. Holst, Kenneth D. Burman, Frank Atkins, Jason G. Umans, Jacqueline Jonklaas. Radioiodine Therapy for Thyroid Cancer and Hyperthyroidism in Patients with End-Stage Renal Disease on Hemodialysis. Thyroid. December 2005, 15(12): 1321-1331. Treatment Options and Their Expected Outcomes – 10 Thus we left trying to decide the best way to perform 131-I therapy. First: decide on the reason for and thus the goal of treatment. Often the goal of therapy is to quickly and permanently end hyperthyroidism. However, is euthyroidism required? Is post therapeutic hypothyroidism acceptable or even desirable? These are as yet unresolved controversies in the literature and clinical practice. Expected outcomes for the 4 methods of radio – iodine therapy are summarized in the table at the beginning of this exhibit (slide 8). Treatment Options and Their Expected Outcomes – 11 For patients with severe signs and symptoms of Graves Disease, a “high dose” therapy will lead ending hyperthyroidism with a higher degree of certainty and possibly sooner. However, the likelihood of hypothyroidism as a result of treatment will increase. Areas of further controversy include how to treat the patient prior to 131-I “curing” the hyperthyroidism and the possible significance of causing early post therapy hypothyroidism. Keep in mind that thyroid hormone replacement can usually be easily managed post therapy in nearly all hypothyroid patients – if they seek medical assistance. The problem here is that many hypothyroid patients might not feel bad - and thus might not seek further physician assistance; although many are symptomatic and seek further medical attention for this reason. Therefore, maintaining contact with previously treated patients is very important. For patients with “lesser” clinical degrees of Graves Disease a “lower dose” 131-I therapy may be acceptable. Keep in mind that lower doses of 131-I often correlate with lower treatment response. Part 6: How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I Currently, there are 4 methods of 131-I therapy for hyperthyroidism commonly reported in the literature: 1. Fixed dose per gram of thyroid tissue. Thyroid size is usually estimated by physical exam; sometimes by ultrasound. Accuracy of estimating thyroid size is a major problem with this method. Often 5.55 Mbq/gm (150 µCi/gm) of thyroid tissue multiplied by estimate of thyroid size is used. Common values for thyroid size: 20 gm-normal; 40 gm- 2x normal; 80 gm-very large gland. This value is then divided by the % uptake usually a recent 123-I 24 hour uptake value is used. As iodine uptake in hyperthyroid patients is variable, performing the 4 and 24 hour uptakes and scans within 1 week of therapy is strongly suggested. Van Isselt JW, et al. Iodine-131 uptake and turnover rate vary over short intervals in Graves’ disease. Nucl Med Commun. 2001:21; 609-616. For example (5.55 MBq/gm or 150 µci/gm * 40 gm thyroid gland size estimate, a moderately enlarged gland) = 222 MBq or 6000 µCi = 6 mCi Then divide this by the 50% 24 hour 123-I uptake. So, 222 MBq/50% or 6 mCi/50% = 444 MBq or 6/.5 = 6 * 2 = 12 mCi. How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 2 To repeat: For example (5.55 MBq/gm or 150 µci/gm * 40 gm thyroid gland size estimate, a moderately enlarged gland) = 222 MBq or 6000 µCi = 6 mCi Then divide this by the 50% 24 hour 123-I uptake. So, 222 MBq/50% or 6 mCi/50% = 444 MBq or 6/.5 = 6 * 2 = 12 mCi. (NB: in the US 24 hr 123-I uptake values of 40% are more common, thus a 555MBq or15 mCi 131-I dose would be commonplace via this method.) In this example, the patient would receive 444 MBq or12 mCi of 131-I to treat his hyperthyroidism. For lack of better terminology, this might be considered a “medium dose”. Various reports in the literature will quote widely varying response rates, as is true with the other methods described on the following slides. How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 3 1. Continued, Fixed dose per gram of thyroid tissue, slide 3. This is the method suggested by Dr. Beierwaltes at the University of Michigan from many years ago and favoured by the main author for most patients. reviewed in: Beierwaltes WH: The Treatment of Hyperthyroidism With Iodine131. Seminars in Nuclear Medicine. 8 (1) Jan 1978, 95-103. Interestingly, it is quite similar to the earliest methods I have found reported, where errors of 50% in thyroid radiation were expected (in part due to errors in gland size estimation and the need for using a mixture of iodine isotopes). Hertz S, Roberts A: Radioactive Iodine In The Study of Thyroid Physiology. VII. The Use of Radioactive Iodine Therapy in Hyperthyroidism. JAMA: 131 (2) May 11, 1946, 81-6. Chapman EM, Evans RD: The Treatment of Hyperthyroidism With Radioactive Iodine. JAMA: 131 (2) May 11, 1946, 86-91. How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 4 1. Continued, Fixed dose per gram of thyroid tissue, slide 4. Millicurie doses from the 1940s are also different from today’s doses as nodular goiter was very common back then, and uncommon now in the US. Yet, even in Hertz’s article a dose range of 125.8-1036 MBq (3.4 – 28 mCi) was used. Chapman used much higher doses, 518-2913 MBq (14 – 79 mCi). Both authors had many patients requiring more than 1 130-I, 131-I combined isotope therapy. Inducing myxedema was 1 of Dr. Chapman’s goals. Many of these early patients had isotope therapy followed by surgery – which was standard therapy at this time How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 5 Methods 2 and 3: Offer a either a fixed amount (MBq or mCi ) for all patients (EG, 259 MBq or 7 mCi total amount, Finland) Saara Metso , Pia Jaatinen, Heini Huhtala, Tiina Luukkaala, Heikki Oksala and Jorma Salmi Long-term follow-up study of radioiodine treatment of hyperthyroidism. Clinical Endocrinology 61:5, 641 - 648, 2004. or adjust an otherwise fixed base amount contingent on the 24 hour 123-I uptake. (EG 296 MBq or 8 mCi, as the amount delivered to the thyroid gland. This method requires more than 296 MBq or 8 mCi as the oral dose (540.2 MBq or 14.6 mCi mean amount of 131-I. Thus mean 24 hour uptake was 54.8%). This is the method suggested by Alexander from Massachusetts General Hospital. (Also see last section for special cases). Erik K. Alexander and P. Reed Larsen High Dose 131I Therapy for the Treatment of Hyperthyroidism Caused by Graves’ Disease The Journal of Clinical Endocrinology & Metabolism 2002, 87:3, 1073-1077. Neither of these methods requires assessment of thyroid gland size. In this way we deliver a certain number of MBq or mCi to the entire gland, as opposed to method 1, where we deliver a certain number of MBq or mCi to each gram of thyroid tissue. How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 6 To review, in Methods 2 and 3, no assessment of thyroid gland size is used. In this way we deliver a certain number of MBq or mCi to the entire gland, as opposed to method 1, where we deliver a certain number of MBq or mCi to each gram of thyroid tissue - which requires measurement of gland size, no matter how imprecise. Method 4: Deliver a fixed radiation dose (Gy) to the thyroid gland. In this method (suggested by Peters) we use a calculated amount (MBq or mCi) in order to deliver about 200 Gy to the thyroid gland. Peters H et al. Radioiodine therapy of Graves' hyperthyroidism: standard vs. calculated 131 iodine activity*. Results from a prospective, randomized, multicentre study. European Journal of Clinical Investigation 1995, 25:3, 186 - 193. Per Figure 4, p.190. How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 7 4. cont. While there are some conversions available between MBq or mCi and Gy, in “typical” patients (555 MBq or 15mCi is about 200 Gy in Peters patients), there may be wide variations in individual patients. Only the review by Dr. Beierwaltes (For reference see Method 1, which included patients with multinodular goitre) contradicts the results found by others: the higher the 131-I dose, the higher the treatment success rate and the higher the rate of post therapy hypothyroidism. The following graphs are suggested by Peters H et al and demonstrate the point. Peters H et al. Radioiodine therapy of Graves' hyperthyroidism: standard vs. calculated 131 iodine activity*. Results from a prospective, randomized, multicentre study. European Journal of Clinical Investigation 1995, 25:3, 186 - 193. Per Figure 4, p.190. 555 MBq =15 mCi ~ 208 Gy 80% This 131-I dose would be in the commonly used range in typical Graves patients in the US (via Beierwaltes method). 50% 100 200 Success rate % vs Radiation Dose absorbed by the thyroid gland (Gy) 250 MBq ~ 7 mCi ~ 100 Gy would be more typical of a “low dose” therapy. How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 8 An Unresolved Factor: Residence Time of 131-I in the Thyroid Gland Most 131-I dosing calculations are based on 24 hour values, without determining the exact residence time of iodine in the gland. References for Iodine mean effective iodine t ½: - German patients, = 4.7d (+/-1.7d) Peters pp 188-9. - Sisson and Gross at the University of Michigan, quoting others, note that, “determinations of the effective half-life of 131-I in hyperthyroid glands have been reasonably consistent at 5 – 5.5 days….” Peters H et al. Radioiodine therapy of Graves' hyperthyroidism: standard vs. calculated 131 iodine activity*. Results from a prospective, randomized, multicentre study. European Journal of Clinical Investigation 1995, 25:3, 186 - 193. and James C. Sisson, Anca M. Avram, Domenico Rubello, Milton D. Gross. LETTER TO THE EDITOR, Radioiodine treatment of hyperthyroidism: fixed or calculated doses; intelligent design or science? Eur J Nucl Med Mol Imaging (2007) 34:1129–1130. Around the world, there is great variation in the amount of iodine available in the diet. Also, low iodine diets are usually recommended in the US prior to use of 131-I for therapy of hyperthyroidism or to treat thyroid cancer. However, many patients do not follow iodine restrictions. While beyond the scope of this presentation, both of these factors can influence the effectiveness of radio iodine therapy. How to Assist in Managing Hyperthyroid Patients Both During Medical Therapy and After 131 - Iodine Therapy 4 Methods Used to Determine Dose of 131-I - 9 Patients at Higher Risk for Treatment Failure, Part 6, slide 9 Alexander at MGH also notes groups at higher likelihood for 131-I treatment failure: Younger patients Larger thyroid glands Higher T4 Higher 24 hour uptake values Erik K. Alexander and P. Reed Larsen High Dose 131I Therapy for the Treatment of Hyperthyroidism Caused by Graves’ Disease The Journal of Clinical Endocrinology & Metabolism 2002 Vol. 87, No. 3 1073-1077. Worse opthalmopathy Prior use of antithyroid medication On this basis, they suggested using a target of 407 MBq or 11 mCi (not 296 MBq or 8 mCi) delivered to the thyroid gland in selected patients <20 gm, gland size > 4x nml, > 70% 24 hour uptake, or prior use of ATD for more than 4 months. Yet, they still expect failure rates at initial therapy of 5-10% (p. 1076) Expected Outcomes and How Long To Wait For These Results, Use of ATDs post 131-I Therapy Depending on the patient’s condition at the time of therapy, worsening of thyroid related signs and symptoms may occur in the weeks to months following 131-I therapy. In frail elderly patients and/or those with significant cardiac problems, close follow up and additional care might be needed. Use of ATDs post 131-I is controversial and might be best limited to those patients with significant hyperthyroid related medical issues. Perhaps, as suggested by the RCP White Paper, using a B blocker, such as propranolol to treat mild to moderate symptoms could be considered in place of using ATDs. However, if an ATD is needed, waiting as long as possible after 131-I therapy is preferred. As the t ½ for 131-I is about 1 week, waiting at least 1 week after 131-I therapy before re-starting ATDs might be prudent. Effects of 131-I therapy typically occur very gradually. It is the author’s experience that those with only weekly (or more in-frequent) contact of the patient have the greatest likelihood of determining significant changes in the patient’s medical status. It may take 2 months or more for clinical changes to occur and/or be notable. Expected Outcomes – Opthalmopathy and Post – Tx Labs However, as stated earlier, opthalmopathy may run an independent course to 131-I therapy. Should the patient note findings suggesting a change in opthalmopathy in the week to months following 131-I therapy, dedicated opthalmology consult is suggested. However, very few practitioners have expertise in this area. The author councils patients not to buy expensive new contact lenses nor glasses in the weeks to months following 131-I therapy as visual acuity changes may also occur, and may vary over time as well. Buy inexpensive ones until the visual acuity has been stable for at least several months. (Then buy the expensive new designer lenses and frames.) Follow up thyroid hormone levels are often obtained no earlier than 4 weeks post 131-I therapy. Obtaining T4 and TSH levels at 8-12 weeks post therapy would seem reasonable in most patients. Further follow up labs can be obtained every 2 months or so during the first year if the patient is doing well clinically. If the patient is not significantly symptomatic nor hypothyroid, continued follow up clinic visits can take place at 1 year post 131-I therapy. Patients may become transiently hypothyroid within the first few months after 131-I therapy. Only continued follow up labs and/or clinic visits can tell if the hypothyroidism is temporary or permanent. Persistent hyperthyroid signs and symptoms or the occurrence of hypothyroidism demand further care. Expected Outcomes – Some Patients Need a Second 131-I Therapy, Others Will Need Synthroid Replacement Hyperthyroid patients might need a second 131-I therapy. A minimum 6 month wait is advised. Most practitioners would wait at least 12 months post initial therapy. Many practitioners will also use a purposely high dose in order to increase the likelihood of ending the patients hyperthyroid state, regardless of the principle of ALARA. All patients and/or their close friends and associates know when the patient remains hyperthyroid. Hypothyroidism post 131-I therapy is not necessarily a complication per se, as this may be the end result of untreated hyperthyroidism anyway (as the thyroid gland may eventually “burn itself out”). Of the 131-I treated patients who become euthyroid at 1 year, several percent per year will become hypothyroid. Thus, all patients treated with 131-I will need to have at least yearly checks of thyroid hormone levels. Many patients DO NOT KNOW when they become and remain hypothyroid. Thus, patient-physician interaction MUST be maintained – through the days, weeks, months, and years following 131-I therapy. Lifelong follow up and laboratory testing is required Case 3 11.4 MBq or 309 uCi 123-I LAO This is a 35 year old man with a 3 month history of emesis, diarrhea, palpitations, tremors with a TSH level of .004. The patient’s symptoms normalized upon taking propylthiouracil (PTU), propanolol, and hydrochlorothiazide, when compliant. 10-30% However pt was non compliant for 3 months. So, in this case 131 – I might be the best tx option. (Although pt may require Synthroid replacement at a later time.) Case 3 This is a 35 year old man with a 3 month history of emesis, diarrhea, palpitations, tremors with a TSH level of .004. The patient’s symptoms normalized upon taking propylthiouracil (PTU), propanolol, and hydrochlorothiazide, when compliant - which he has not been for 3 months. Optimal 131-I oral dose, by method used: Method 1: 5.55 MBq/gm or 150 µCi/gm * 30 gm thyroid gland (mildly enlarged) = 166.5 MBq or 4500 µCi = 4.5 mCi 131-I then divide by 24 hour % uptake, so 4.5 mCi / 0.74 = 225 MBq or 6 mCi 131 – I Method 2: 259 MBq or 7 mCi 131-I (all patients) Method 3: (for 296 MBq or 8mCi delivered dose: 296 MBq / 0/74 = 400 MBq or 8 mCi / 0.74 (the 24 hour uptake) = 10.8 mCi 131 –I) However, per Part 6, slide 9, this patient merits a dose escalation to 407 MBq or11 mCi delivered dose due to: prior use of ATDs and 24 hour uptake > 70% for 407 MBq or11 mCi delivered dose to the thyroid gland: 407 MBq / 0.74 = 550 MBq or 11 mCi / 0.74 = 14.9 mCi 131-I Case 3 This is a 35 year old man with a 3 month history of emesis, diarrhea, palpitations, tremors with a TSH level of .004. The patient’s symptoms normalized upon taking propylthiouracil (PTU), propanolol, and hydrochlorothiazide, when compliant - which he has not been for 3 months. Optimal 131-I oral dose, by method used: Method 4: Without additional calculations, in part based on residence time of 131-I in the thyroid gland (not done here), estimated dose would be (all pts) ~555 MBq or ~15 mCi 131-I Thus, in the 4 methods we have a wide range of recommended dose: 225-555 MBq or 6-15 mCi 131-I Due to compliance issues and the fear that the patient might not follow up properly post 131-I therapy, a lower dose of 222 MBq or 6 mCi 131-I was suggested. This would make post tx hypothyroidism less likely, although percent treatment success at 1 year would also be reduced. The patient can put back on PTU and blocker 1 week after 131-I oral therapy. Expectation of Resultant Eu- vs Hypo-thyroidism In an editorial, Ross McDougall at Stanford seems to provide a concise summary: “The optimal outcome after 131I therapy for hyperthyroidism is obviously euthyroidism without postablative hypothyroidism and the need for lifelong thyroid hormone replacement. It is now well accepted, however, that there is no single radioiodine dose or treatment method that can reliably accomplish that goal. This is not surprising considering the number of variables affecting the outcome, including characteristics of the patient (i.e. age, gender, and gland size); severity and duration of the underlying autoimmune thyroid stimulus; radiation delivered to the gland (i.e. 131I fractional uptake, homogeneity of distribution, and effective half-life); and preceding antithyroid drug therapy (i.e. whether thionamides were used, which one, and the time that the drug was stopped before radioiodine treatment) (7, 8, 9). Nonetheless, two facts are apparent. First, the higher the prescribed dose, the higher the fractions of patients who are cured and who develop postablative hypothyroidism (10, 11, 12). Second, some patients become hypothyroid after treatment with even small doses of 131I.” He also notes that the lowest effective 131-I dose to rid hyperthyroidism should be our goal, even if hypothyroidism would be a common outcome. This can be achieved via both fixed and calculated dose regimens. Judith E. Kalinyak and I. Ross McDougall. EDITORIAL: How Should the Dose of Iodine-131 Be Determined in the Treatment of Graves’ Hyperthyroidism? The Journal of Clinical Endocrinology & Metabolism 2003, 88:3, 975-977. Practice Patterns: Some UK Guidelines Weetman reviews the treatment practices for hyperthyroidism in the UK. While these are only guidelines, as you can see the range of 131-I used varies. Anthony P. Weetman CLINICAL PRACTICE UPDATE Radioiodine treatment for benign thyroid diseases Clinical Endocrinology 2007, 66:6, 757-764. Table from p. 758. NB: 370 MBq = 10mCi, 555 MBq = 15 mCi, 800 MBq = 30 mCi, the maximum outpatient dose allowable in many states in the USA. These guidelines are meant to help provide more uniform treatment of patients, based on published data, while keeping overall costs low. Practice Patterns: Some Finnish Guidelines – Low Dose (vs Medium Dose) Therapy With 131-I In this Finnish study, which looked at 2043 patients from 1965-2002, with a median follow up of 9.8 years, a fixed dose of about 259 MBq or 7 mCi was used in most patients. Patient population included toxic nodular goitre. One infers that the quoted 80% “cure” rate is at 1 year post 259 MBq or 7 mCi 131-I therapy. Saara Metso , Pia Jaatinen, Heini Huhtala, Tiina Luukkaala, Heikki Oksala and Jorma Salmi Long-term follow-up study of radioiodine treatment of hyperthyroidism. Clinical Endocrinology 61:5, 641 - 648, 2004. It should be noted, that in some other studies the low dose amounts used often had similar or even better results than higher dose techniques. (Inferred from Leslie, McDougall, and others.) WILLIAM D. LESLIE, LINDA WARD, ELIZABETH A. SALAMON, SORA LUDWIG, RICHARD C. ROWE, AND ELIZABETH A. COWDEN. A Randomized Comparison of Radioiodine Doses in Graves’ Hyperthyroidism. The Journal of Clinical Endocrinology & Metabolism 88(3):978–983, 2003. Practice Patterns: Some Finnish Guidelines – Low Dose (vs Medium Dose) Therapy With 131-I In this author’s experience of almost 20 years in practice, I would estimate my average patient dose to be approximately 555 MBq or 15 mCi. This is in line with dosages of 131-I used in my community. I do not have the long term results data reported from Finland, nor do I expect to, given changes in practice location. Unpublished verbal communications to the primary author here, have indicated a low dose therapy response rate of only about 67% (in patients without goiter). This is less than the expected ~80% cure rate from the Finnish study. Perspective: EURATOM 97/43, a European Union Directive, published in 1997, states the importance of individualization of therapy in order to reduce dose exposures and increase specified targeting benefits of radiation therapy including the use of nuclear sources. Case 4 This is an 83 year old female with a history of thyrotoxicosis with hypercalcemia and impaired fasting glucose. The patient is to continue on 10 mg of methimazole every day. The patient has a diagnosed parathyroid adenoma. 10-30% So in this case, medical therapy worked well. 131-I therapy can follow at a later date, should this patient subsequently fail medical therapy. Case 4 This is an 83 year old female with a history of thyrotoxicosis with hypercalcemia and impaired fasting glucose. The patient is to continue on 10 mg of methimazole every day, as she is doing well on this regimen. The patient also has a diagnosed parathyroid adenoma – but this does not effect our hyperthyroid treatment, unless she needs surgery for treating the adenoma. If she subsequently fails medical therapy for Graves Disease, here are the calculations for optimal 131-I oral dose, by method used. Results vary widely: Method 1: 5.55 MBq/gm or 150 µCi/gm * 20 gm thyroid gland (not enlarged) = 111 MBq or 3000 µCi = 3 mCi 131-I then divide by 24 hour % uptake, so 11.1 MBq / 0.389 = 285 MBq or 3 mCi / 0.389 = 7.7 mCi 131 – I (***Remember – this is the only method which varies by thyroid gland size, so if her gland was enlarged at 40 gm, a 570 MBq or 15.4 mCi 131-I tx would be recommended.) Method 2: 259 MBq or 7 mCi 131-I (all patients) Case 4 This is an 83 year old female with a history of thyrotoxicosis with hypercalcemia and impaired fasting glucose. The patient is to continue on 10 mg of methimazole every day, as she is doing well on this regimen. The patient also has a diagnosed parathyroid adenoma – but this does not effect our hyperthyroid treatment, unless she needs surgery for treating the adenoma. If she subsequently fails medical therapy for Graves Disease, here are the calculations for optimal 131-I oral dose, by method used. Results vary widely: Method 3: (for 296 MBq or 8mCi delivered dose: 8 mCi / 0.389 (the 24 hour uptake) = 761 MBq or 20.6 mCi 131 –I) However, per Part 6, slide 9, this patient merits a dose escalation to 407 MBq or 11 mCi delivered dose to the thyroid gland due to: prior use of ATDs 11 mCi delivered dose: 407 / 0.389 = 1047 MBq or 11 mCi / 0.389 = 28.3 mCi 131-I Method 4: Without additional calculations, in part based on residence time of 131-I in the thyroid gland (not done here), estimated dose would be (all pts) ~ 555 MBq or ~15 mCi 131-I Thus, in the 4 methods we have a wide range of recommended dose: 259-1047 MBq or 7-28.3 mCi 131-I Relative Cost of Therapeutic Options In a recent review of hyperthyroid therapy looked at the cost of various methods used to treat hyperthyroid patients. Lucignani G Long Term Risks In Hyperthyroid Patients Treated With Radioiodine: Is There Anything New? Eur J Nucl Med Mol Imaging (2007) 1504-1509 $9,826.00: Surgical thyroidectomy $5,644.00: Medical (thionamides: Propylthiouracil (PTU) and methimazole (Tapazole®, MMI) are the thionamide drugs available in the United States ): $2,063.00: 131-I - by far, the lowest cost Perspective: With most radioiodine therapeutic methodologies used, a “cure” rate of over 2/3 would be expected. This is far greater than medical therapy, though lower than surgery. How does this compare to treating common diseases? Do we expect at least 2/3 of hypertensive patients to be well maintained on medication? Relatively High Success Rate for 131-I Therapy When Compared to Treatment for a Common Disease - Hypertension Context of patient therapy: As you can see, compared to treating hypertension (only 34% are controlled), we do a great job treating hyperthyroidism with 131-I. But remember, all patients, including those made hypothyroid need lifelong care and follow up. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Heart, Lung, and Blood Institute National High Blood Pressure Education Program The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure - Complete Report JNC 7 Complete Report: The Science Behind the New Guidelines NIH Publication No. 04-5230 August 2004 http://www.nhlbi.nih.gov/guidelines/hypertension/jnc 7full.pdf Pre 131-I Therapy Planning As with all nuclear medicine therapy procedures we need to make sure that: -Proper informed consent must be obtained from the patient or legal guardian. This requires knowledge of the relative strengths and weaknesses of other therapeutic modalities. Also review the possibility of hypothyroidism as a therapy result and the possibility of therapy failure. In those patients under age 18, parental consent is also required. -All female patients must be checked for possible pregnancy. If planning to have children, waiting 6 -12 months post 131-I therapy before attempting conception is encouraged. -Breast feeding is not allowed for a minimum of 3 months (approx 10 half lives of 131-I). Most would insist that breast feeding be halted permanently for that child. -For Graves Disease, doses used usually do not require hospitalization in the US. However, as regulations vary around the world, local practitioners might need to either adjust maximal dose usable in the outpatient setting or admit the patient until their total body burden of 131-I falls below certain levels (mR/hr). -ATDs need to be stopped prior to 131-I therapy? Well, not all agree. A 2008 article from the Netherlands look at practices in Holland and suggested that: G.S. Mijnhout*, A.A.M. Franken ATDs be withdrawn at least 4 days before use of 131-I Antithyroid drug regimens before PTU use should be stopped at least 15 days before 131-I and after 131I-therapy for hyperthyroidism: evidence-Resumption of ATD use post therapy should be limited to based? The Netherlands Jnl of high risk groups including those > 70 years old and those Med 2008; 66:6:238-241. with significant cardiac issues. Pre 131-I Therapy Planning - 2 Performing the therapy: -Before even ordering the dose, please make sure that the patient will be able to participate in taking the 131-I. Is the patient continent for urine? Patient must also be in a suitable home and work setting. This can be an issue; for example where young children are at home or work; use of public transport; when the patient provides care for total care need elderly relatives. After dosing the patient needs to comply with certain guidelines (see below). -Use of a low iodine diet prior to and following therapy is encouraged. -Use of radiologic (X-ray, CT) iodinated contrast must be avoided for a minimum of 4 weeks before 131-I therapy. The author prefers an 8 week or 2 month wait, in part due to the long circulating t ½ of thyroid hormone. MRI gadolinium based contrast is not an issue. -Effects of lithium are controversial. -Most countries have specific isotope training requirements beyond general medical training before one can be the “authorized user” of 131-I for therapeutic purpose. In the US, only an authorized user can be responsible for giving or dosing the 131-I for treatment purpose. Nuclear medicine physicians and many-most radiologists will qualify. However, many endocrinologists will not qualify without additional training. Pre 131-I Therapy Planning - 3 Performing the therapy, cont: -Assure that the 131-I dose is received intact. The nuclear medicine technologist usually does this. -Assay it in the hot lab to confirm the dose. It must be +/- 10% of the prescribed dose in the US. Although the technologist must do this, in the US, the physician is ultimately responsible for this too, so good form dictates that physicians are present during the assay in the well counter. In some places, both techs and doctors are required to sign off on this. Records of this must be maintained. -131-I comes in both liquid and solid (capsule) forms. As a liquid it is highly volatile. Therefore, all medical personnel involved in the therapy need to have their thyroid glands assayed for 131-I, both before and 1-2 days post therapy. This additional personnel assay is not needed when capsules are used in the US. Thus, most prefer using capsules. In the US, these regulations are part of 10 CFR 20, but require your radiation safety officer (RSO, often a physicist) to decipher. Records must also be kept of these measurements. Potential Complications of 131-I Therapy Early complications may include: - Day of therapy: a - nausea and vomiting. Not common, but if the patient vomits the dose in the hospital or clinic it must be properly cleaned up. There will also be all of the necessary record keeping for radioactive spills. Remember, making certain that the patient is stable comes first. If this occurs at home, most of the 131-I should have passed beyond the stomach by this time. b – anxiety. Not common as a major problem; though most patients have some anxiety about “nuclear” agents. This can be addressed per symptoms. Physician reassurance is helpful. - In the days to weeks following therapy: Sialadenitis – inflammation of the salivary glands, possibly including damage to or destruction of the salivary glands is along known potential complication of 131-I therapy. Temporary or permanent “dry mouth” may result. This is prevented by having the patient suck on sour candies that promote salivary flow. There is a recent paper on this subject. Edward B. Silberstein. Reducing the Incidence of 131I-Induced Sialadenitis: The Role of Pilocarpine THE JOURNAL OF NUCLEAR MEDICINE, April 2008, 49:4, 546-9. 131 – I Dose Used So, how much 131-I should we use to treat Graves Hyperthyroidism? This, in part, is the art of medicine. Based on the data presented here the following may be useful: --Patients with mild-moderate signs and symptoms and mildly enlarged thyroid glands: 259-555 MBq or 7-15 mCi. These patients might need retreatment, but the lack of a rapid end to their hyperthyroidism should not cause them significant harm. Retreatment might be needed. --Patients with some significant signs and symptoms and/or those with large thyroid glands: 555-740 MBq or 15-20 mCi. Yes, a larger dose and there is a greater likelihood of post 131-I treatment hypothyroidism. However, the likelihood of ending hyperthyroidism is greater. --Patients with severe signs and symptoms and/or those with very large glands: 740-1210 MBq or 20-30 mCi of 131-I. The higher dose, although it does not follow the concept of ALARA, should allow for the highest certainty of ending hyperthyroidism and thus alleviating signs and symptoms caused by it. Time to eradicate the hyperthyroid condition might be the same as in lower doses; often requiring several months following treatment. However, post therapy hypothyroidism is very likely. Part 7: Links to More Detailed Procedural, Informed Consent, and Regulatory Information - Regulations Regulations vary between states in the US (Agreement vs non-Agreement states) and between countries. Many states in the US allow a maximal outpatient dose of 3033 mCi. LA is an agreement state. In the US, per The Code of Federal Regulations, 10CFR35, “§ 35.75 Release of individuals containing unsealed byproduct material or implants containing byproduct material. (a) A licensee may authorize the release from its control of any individual who has been administered unsealed byproduct material or implants containing byproduct material if the total effective dose equivalent to any other individual from exposure to the released individual is not likely to exceed 5 mSv (0.5 rem).1” http://www.nrc.gov/reading-rm/doc-collections/cfr/part035/full-text.html http://www.nrc.gov/reading-rm/doc-collections/cfr/part035/part035-0075.html In practice, for 131-I, the maximum outpatient dose would be 1.2 GBq or 33 mCi, 0.07 mSv/hr or http://www.scdhec.gov/health/radhlth/ReleasePatients.pdf, 7 mrem/hr REGULATORY GUIDE Bureau of Radiological Health Division of Radioactive Material Licensing and Compliance February 2006 “Release of Patients Administered Radioactive Materials”, pp 8-9, Table 1. Activities and Dose Rates for Authorized Patient Release Ψ Don’t forget, there are record keeping requirements for use of radio isotopes in the US. Elsewhere in the world, regulations will vary, but may be even more strict. Practitioners will need to know the regulations in place at their location. Follow-up Management and Conclusion Hypothyroid patients are placed on Synthroid ® replacement therapy. Taken orally 3-7 times per week, this provides for maintenance of euthyroid thyroid hormone levels. Children, pregnant women, athletes, and average adults can be easily and successfully treated. But again, lifelong follow up and laboratory testing is required. General Radiologists and Nuclear Medicine Physicians can be valuable members of a team treating and caring for patients with hyperthyroidism. This concludes this presentation. Thank you for your attention. I hope you will enjoy being involved in the care of hyperthyroid patients as much as I am. FIN