Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
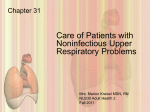
What is the most common site of origin of ocular sebaceous carcinoma? (A) Meibomian gland (B) gland of Zeis (C) lacrimal gland (D) caruncle (E) multicentric origin Answer A. Explanation: Sebaceous carcinoma, also called Meibomian gland carcinoma, represents an aggressive primary malignancy of the adnexal epithelium of sebaceous glands. About 75% of sebaceous carcinomas are ocular in origin, while the remaining 25% of tumors are considered extraocular. Ocular sebaceous carcinomas account for 1.5–5% of all malignant eyelid neoplasms. The tumor most frequently develops on the upper eyelid of elderly patients (Fig. 33-18). FIG. 33-18 Sebaceous carcinoma of upper eyelid in elderly female. Clinically, the lesion may present as a firm yellowish nodule, resembling a chalazion, or may mimic an inflammatory condition such as blepharoconjunctivitis or keratoconjunctivitis. Often, the diagnosis is delayed from 1 to 3 years. Between 51 and 70% of ocular sebaceous carcinomas originate from Meibomian glands of the tarsus. Less commonly, the tumor is either multicentric in origin or develops from the glands of Zeis, the lacrimal gland, or the caruncle. Histologically, the tumor appears as an infiltrative, nonencapsulated dermal Answer A. Explanation: Sebaceous carcinoma, also called Meibomian gland carcinoma, represents an aggressive primary malignancy of the adnexal epithelium of sebaceous glands. About 75% of sebaceous carcinomas are ocular in origin, while the remaining 25% of tumors are considered extraocular. Ocular sebaceous carcinomas account for 1.5–5% of all malignant eyelid neoplasms. The tumor most frequently develops on the upper eyelid of elderly patients (Fig. 33-18). FIG. 33-18 Sebaceous carcinoma of upper eyelid in elderly female. Clinically, the lesion may present as a firm yellowish nodule, resembling a chalazion, or may mimic an inflammatory condition such as blepharoconjunctivitis or keratoconjunctivitis. Often, the diagnosis is delayed from 1 to 3 years. Between 51 and 70% of ocular sebaceous carcinomas originate from Meibomian glands of the tarsus. Less commonly, the tumor is either multicentric in origin or develops from the glands of Zeis, the lacrimal gland, or the caruncle. Histologically, the tumor appears as an infiltrative, nonencapsulated dermal Depicted in Fig. 38-2 is an 18-year-old male whose left eye was struck with a baseball. He complains of double vision, a headache, and tenderness in his left cheek. The most likely injury is FIG. 38-2 (A) orbital floor fracture (B) intracranial hemorrhage (C) retinal detachment (D) LeFort III fracture Answer A. Explanation: This most likely represents an orbital floor fracture. A black eye finding on physical examination is not an innocuous finding. It must be followed through with a thoroughly directed head/neck examination including cranial nerves II through XII, palpation for tenderness, and an ophthalmologic consultation. A CT scan with coronal and axial scanning cuts is recommended (Figs. 38-41 and 38-42). Typically after localized trauma to the periorbital region, bony sheer forces create an orbital floor blowout fracture. Periorbital muscles and fat can become herniated and trapped in the fracture line along the orbital floor causing restriction of eye movement resulting in diplopia. Intraocular hemorrhage, such as hyphema, may accompany the bony injury. An orbital floor fracture can also be part of a series of fractures such as in the case of a zygomatical maxillary complex fracture. FIG. 38-41 FIG. 38-42 In this case, the physical findings do not represent a LeFort III fracture A 36-year-old female presents with pain and loss of vision in her right eye, worsening over 3 days. Her past medical history is significant for left TN treated with carbamazepime for 4 years and depression controlled with sertraline. On neurologic examination, her right eye vision in 20/400, left is 20/40. She has a Marcus-Gunn pupil (afferent pupillary defect) on the right. Her extraocular movements are intact although testing causes increased pain in the eye. Fundoscopic examination reveals no abnormality in either eye. The most likely diagnosis for this patient is (A) hysteria (B) carbamazepime toxicity (C) optic neuritis (D) amaurosis fugax Answer C. Explanation: This patient is suffering from optic neuritis. It has been described as a syndrome in which "the patient can't see anything and the doctor can't see anything," owing to a lack of findings on examination. This may lead the examiner to believe the patient is hysterical. The patient will have a relative afferent papillary defect (RAPD or Marcus-Gunn pupil), which is diagnosed with the swinging light test. The pupils are equal at baseline and constrict in the light; however, when swinging the light from the normal eye to the affected eye, the pupils will dilate. This is due to a relative decrease in afferent stimulation of the affected eye. Significant monocular vision loss does not occur without an RAPD. Optic neuritis is the initial presentation of MS in 15% of cases, and 50% of patients with MS will develop optic neuritis at some point in their course. MS is a chronic demyelinating disease that is usually diagnosed in young adulthood, and affects women twice as often as men. Its cause is unknown. The diagnosis is made based on the history of neurologic symptoms combined with MRI evidence of lesions explaining the deficits. Lumbar puncture for elevated IgG index and oligoclonal bands. It can be a relapsing-remitting or chronic-progressive disease. TN usually presents in the sixth decade. Its diagnosis in a young person should prompt a workup for MS. Amaurosis fugax is usually very transient (minutes), painless, and the vision loss if How many bones make up the orbit? (A) 7 (B) 8 (C) 9 (D) 6 (E) 4 Answer A. Explanation: The following seven bones make up the orbit: frontal, zygoma, maxilla, palatine, greater and lesser wings of the sphenoid, lacrimal, and ethmoid bones. Of note, the nasal and temporal bones do not contribute. Orbital anatomy is very intricate, and surgery on or around the eye requires thorough knowledge of it. The optic nerve passes through the optic foramen. The superior orbital fissure, located between the greater and lesser wings of the sphenoid, permits passage of cranial nerves III, IV, V1, and VI. The greater wing of the sphenoid is separated from the orbital floor by the inferior orbital fissure that provides passage of the infraorbital artery, V2, branches of the inferior ophthalmic vein to the pterygoid plexus, and branches of the sphenopalatine ganglion. The supraorbital vessels and nerve are transmitted through the supraorbital notch/foramen, while the infraorbital vessels and nerve travel via the infraorbital notch. Five orbital fat compartments exist in the eyelids: two in the upper lid and three in the lower lid. These are manipulated and/or removed during blepharoplasty, but excessive removal may cause a hollowed-out appearance. Hemostasis is key during a blepharoplasty as blindness is likely to ensue following an untreated hematoma. You may be called into the recovery room after a blepharoplasty because the patient is A 36-year-old female presents with pain and loss of vision in her right eye, worsening over 3 days. Her past medical history is significant for left TN treated with carbamazepime for 4 years and depression controlled with sertraline. On neurologic examination, her right eye vision in 20/400, left is 20/40. She has a Marcus-Gunn pupil (afferent pupillary defect) on the right. Her extraocular movements are intact although testing causes increased pain in the eye. Fundoscopic examination reveals no abnormality in either eye. The most likely diagnosis for this patient is optic neuritis. The most appropriate next step in the above patient's management is (A) psychologic evaluation (B) serum carbamazepime level and liver function testing (C) MRI of the brain and possible lumbar puncture (D) carotid duplex imaging Answer C. Explanation: This patient is suffering from optic neuritis. It has been described as a syndrome in which "the patient can't see anything and the doctor can't see anything," owing to a lack of findings on examination. This may lead the examiner to believe the patient is hysterical. The patient will have a relative afferent papillary defect (RAPD or Marcus-Gunn pupil), which is diagnosed with the swinging light test. The pupils are equal at baseline and constrict in the light; however, when swinging the light from the normal eye to the affected eye, the pupils will dilate. This is due to a relative decrease in afferent stimulation of the affected eye. Significant monocular vision loss does not occur without an RAPD. Optic neuritis is the initial presentation of MS in 15% of cases, and 50% of patients with MS will develop optic neuritis at some point in their course. MS is a chronic demyelinating disease that is usually diagnosed in young adulthood, and affects women twice as often as men. Its cause is unknown. The diagnosis is made based on the history of neurologic symptoms combined with MRI evidence of Which of the following statements about cholesteatoma is true? (A) It is a malignant tumor. (B) The primary symptom is tinnitus. (C) It is caused from eustachian tube dysfunction. (D) It is a disease of the inner ear. Answer C. Explanation: Cholesteatoma is an epidermoid cyst of the middle ear and/or mastoid, which causes bone destruction secondary to its expansile nature and through enzymatic destruction. Cholesteatoma develops as a consequence of eustachian tube dysfunction and chronic otitis media secondary to retraction of squamous elements of the tympanic membrane into the middle ear space. Squamous epithelium may also migrate into the middle ear via a perforation. Chronic mastoiditis that fails medical management or is associated with cholesteatoma is treated by mastoidectomy. (See Schwartz 8th ed., Chapter 17, Ear Infections.) Laryngoscopic findings after a superior laryngeal nerve injury include (A) Ipsilateral vocal cord in a paramedian position (B) Ipsilateral vocal cord in a middling position (C) Asymmetry of the glottic opening (D) Normal examination Answer C. Explanation: Superior laryngeal nerve injury is less debilitating, providing the patient's profession is not related to their vocal performance, as the common symptom is loss of projection of the voice. The glottic aperture is asymmetrical on direct laryngoscopy and management is based on clinical observation. (See Schwartz 8th ed., Chapter 11, Organ System Complications.) See all AccessSurgery content on: Which of the following statements about acute suppurative parotitis is NOT correct? (A) Decreased oral intake is a causative factor (B) Most patients are older than 70 years of age (C) Parotitis usually develops during the postoperative period (D) Poor oral hygiene is a contributing factor Answer C. Explanation: These infections develop in elderly individuals with poor oral hygiene and limited oral intake. The majority of infections are caused by staphylococci which invade Stensen's duct where there is minimal parotid secretion. Although these infections can occur in the postoperative period, the majority of cases are not related to an operation. (See Schwartz 7th ed.) Diagnosis of chronic sinusitis is best made by (A) Computed tomography scan (B) Magnetic resonance imaging (C) Nuclear medicine scanning (D) History, physical, and nasal endoscopy Answer D. Explanation: Nasal endoscopy is a critical element of the diagnosis of chronic sinusitis. Anatomic abnormalities, such as septal deviation, nasal polyps, and purulence may be observed. The finding of purulence by nasal endoscopy is diagnostic of sinusitis, regardless of whether other criteria are met. In a setting in which symptoms persist for at least 12 weeks, purulence on nasal exam represents an acute exacerbation of chronic sinusitis. Pus found on endoscopic exam may be cultured, and subsequent antibiotic therapy can be directed accordingly. The spectrum of bacteria found in chronic sinusitis is highly variable and includes higher prevalences of polymicrobial infections and antibiotic-resistant organisms. Overall, S. aureus, coagulase-negative staphylococci, gram-negative bacilli, and streptococci are isolated, in addition to the typical pathogens of acute sinusitis. (See Schwartz 8th ed., Chapter 17, Benign Conditions of the Head and Neck.) Which of the following statements concerning surgery for sleep apnea is true? (A) Surgery is indicated in all patients. (B) Most patients improve with time, and surgery is therefore not indicated. (C) The majority of patients are treated with tracheostomy alone. (D) The most common procedure performed is correction of soft palate collapse. Answer D. Explanation: Sleep disorders represent a continuum from simple snoring to upper airway resistance syndrome (UARS) to obstructive sleep apnea (OSA). UARS and OSA are associated with excessive daytime somnolence and frequent sleep arousals. In OSA, polysomnogram demonstrates at least 10 episodes of apnea or hypopnea per hour of sleep. The average number of apneas and hypopneas per hour can be used to calculate a respiratory disturbance index (RDI), which, along with oxygen saturation, can be used to grade the severity of OSA. These episodes occur as a result of collapse of the pharyngeal soft tissues during sleep. In adults, it should be noted that in addition to tonsil size, factors such as tongue size and body mass index are significant predictors of OSA. Other anatomic findings associated with OSA include obese neck, retrognathia, low hyoid bone, and enlarged soft palate. Surgery should be considered after failure of more conservative measures, such as weight loss, elimination of alcohol use, and continuous positive airway pressure, and should be tailored to the particular patient's pattern of obstruction. In children, surgical management typically involves tonsillectomy and/or adenoidectomy, because the disorder is usually caused by hypertrophy of these structures. In adults, uvulopalatoplasty is frequently performed to Trauma of the auricle of the ear with hematoma formation (A) Requires transcartilage sutures for approximation (B) Requires bolstering for most injuries (C) Can be treated conservatively with dressings only (D) Aggressive débridement is essential Answer B. Explanation: With laceration of the auricle, key structures such as the helical rim and antihelix must be carefully aligned. These injuries must be repaired such that the cartilage is covered. The principles of auricular repair are predicated on the fact that the cartilage has no intrinsic blood supply and is thus susceptible to ischemic necrosis following trauma. The suture should be passed through the perichondrium, while placement though the cartilage itself should be avoided. Auricular hematomas should be drained promptly, with placement of a bolster as a pressure dressing. A pressure dressing is frequently advocated after closure of an ear laceration. It also deserves note that the surgeon must avoid the temptation to perform aggressive débridement after injuries to the eyelid or auricle. Given the rich vascular supply to the face and neck, many softtissue components that appear devitalized will indeed survive. (See Schwartz 8th ed., Chapter 17, Trauma of the Head and Neck.) Le Fort II fracture entails injuries to all of the following EXCEPT (A) Medial wall of the orbit (B) Alveolus (C) Zygomaticomaxillary articulation (D) Nasofrontal buttress (E) Mandible Answer E. Explanation: Le Fort I fractures occur transversely across the alveolus, above the level of the teeth apices. In a pure Le Fort I fracture, the palatal vault is mobile while the nasal pyramid and orbital rims are stable. The Le Fort II fracture extends through the nasofrontal buttress, medial wall of the orbit, across the infraorbital rim, and through the zygomaticomaxillary articulation. The nasal dorsum, palate, and medial part of the infraorbital rim are mobile. The Le Fort III fracture is also known as craniofacial disjunction. The frontozygomaticomaxillary, frontomaxillary, and frontonasal suture lines are disrupted. The entire face is mobile from the cranium. It is convenient to conceptualize complex midface fractures according to these patterns; however, in reality, fractures reflect a combination of these three types. (See Schwartz 8th ed., Chapter 17, Trauma of the Head and Neck.) Which of the following is the preferred treatment of tracheal stenosis after prolonged intubation? (A) Observation (B) Balloon dilatation (C) Laser ablation of scar (D) Resection and primary anastomosis Answer D. Explanation: The treatment of tracheal stenosis is resection and primary anastomosis. In nearly all postintubation injuries the injury is transmural, and significant portions of the cartilaginous structural support are destroyed. Measures such as laser ablation are temporizing. In the early phase of evaluating patients, dilatation using a rigid bronchoscope is useful to gain immediate dyspnea relief and to fully assess the lesion as well as its length, position, and relation to the vocal cords. Rarely if ever is a tracheostomy necessary. For patients unable to tolerate general anesthesia because of comorbidities, internal stents, typically silicone T tubes, are useful. Wire mesh stents should not be used, given their known propensity to erode through the wall of the airway. (See Schwartz 8th ed., Chapter 18, Trachea.) The most common branchial cleft fistula originates from the (A) 1st branchial cleft (B) 2nd branchial cleft (C) 3rd branchial cleft (D) 4th branchial cleft Answer B. Explanation: Paired branchial clefts and arches develop early in the fourth gestational week. The first cleft and the first, second, third, and fourth pouches give rise to adult organs. The embryologic communication between the pharynx and the external surface may persist as a fistula. A fistula is seen most commonly with the second branchial cleft, which normally disappears, and extends from the anterior border of the sternocleidomastoid muscle superiorly, inward through the bifurcation of the carotid artery, and enters the posterolateral pharynx just below the tonsillar fossa. The branchial cleft remnants may contain small pieces of cartilage and cysts, but internal fistulas are rare. A second branchial cleft sinus is suspected when clear fluid is noted draining from the external opening of the tract at the anterior border of the lower third of the sternocleidomastoid muscle. Rarely, branchial cleft anomalies occur in association with biliary atresia and congenital cardiac anomalies, an association that is referred to as Goldenhar's complex. (See Schwartz 8th ed., Chapter 38, Neck Masses.) The most common area of the mandible to be fractured is the (A) Condyle (B) Ramus (C) Angle (D) Body Answer A. Treatment of a 3-mm displaced fracture of the anterior wall of the frontal sinus is (A) Observation (B) Antibiotics alone (C) Open reduction (D) Open reduction, demucosalization, and packing of fat into the sinus Answer C. Explanation: The most common surgical approach to the frontal sinus is through a coronal incision. Treatment of frontal sinus fractures is predicated on the number of walls involved and the status of the nasofrontal duct (Fig. 44-34). In nondisplaced anterior wall fractures, no treatment is indicated. If the anterior wall is displaced, then elevation and recontouring of the anterior table is executed. The patient should be observed for any sinus opacification or obstruction. If the nasofrontal duct is involved in the fracture, one can assume that this is a dysfunctional sinus. Therefore, the sinus must be demucosalized, the nasofrontal duct must be plugged with bone graft, and sinus cavity obliterated with cancellous bone or fat. The technique of frontal sinus exenteration or removal of the anterior table, with demucosalization plugging of the ducts, is an antediluvian procedure not routinely performed because of the significant contour deformity. (See Schwartz 8th ed., Chapter 44, Maxillofacial Trauma.) Three days after an accident in which a 25-year-old woman suffers a maxillary and mandibular fracture, she develops facial nerve palsy with oral incompetence and slurred speech. The facial nerve problem should be managed by (A) Facial nerve graft (B) Facial nerve suture (C) Nonoperative management (D) Transfer of part of the masseter muscle to the oral commissure Answer C. Explanation: When facial nerve palsy is incomplete or late in appearance, the nerve injury is partial. With observation, the palsy will regress over time, and intervention is not required. The operative techniques listed may be necessary with a complete nerve injury. (See Schwartz 7th ed.) Which of the following is the best treatment of a septal hematoma in a patient with a nasal fracture? (A) Observation (B) Aspiration of the hematoma (C) Closed reduction of the fracture and aspiration of the hematoma (D) Operative repair of the fracture Answer B. Explanation: The nose is the most commonly fractured facial region. The nose is either laterally or posteriorly displaced, and the fracture may involve the cartilaginous septum, or both the nasal bones and septum. Patients commonly present with swelling, nasal deformity, epistaxis, septal deviation, and/or crepitus on palpation. Intranasal inspection should be performed, and if a septal hematoma is noted, it should be percutaneously drained. Diagnosis by computed tomography (CT) scan is not obligatory but is implemented to rule out other injuries. Immediate treatment consists of reduction of both the pyramid and septum, followed by nasal splinting. In spite of early reduction, there is usually a residual deformity or deviations, which will require formal rhinoplasty in an elective setting after swelling and bruising have resided. (See Schwartz 8th ed., Chapter 44, Maxillofacial Trauma.) Which of the following is the most common nerve deficit after resection of a poststyloid compartment parapharyngeal neurilemmoma? (A) ptosis (B) painful shoulder syndrome (C) deviation of tongue to the operated side (D) voice change or hoarseness (E) corneal exposure Answer A. Explanation: The parapharyngeal space (PPS) can be thought of as an inverted pyramid. The boundaries of this space are the base of skull superiorly and the hyoid bone inferiorly. The space itself is deep to the pharyngeal mucosa and superficial to the carotid sheath and it communicates with the submandibular space. It can be divided into a prestyloid and poststyloid or retrostyloid space by the syloid muscles and a band of fascia from the tensor veli palatini. These spaces are important when discussing tumor pathology and surgical approaches. The prestyloid space contains fat, the mandibular branch of the facial nerve, the pterygoid venous plexus, whereas the poststyloid space contains cranial nerves IX– XII, the cervical sympathetic chain and the internal carotid artery and internal jugular vein (IJV). The differential of masses in the PPS is large but can be broken into four categories: salivary gland tumors, neurogenic tumors, lymph node enlargement, or miscellaneous tumors. Patients can present with symptoms of airway obstruction from poststyloid masses, pain or cranial nerve palsies of nerves in the PPS. Patients can also present with a unilateral serous otitis media from Eustachian tube dysfunction. A CT scan and/or MRI would be the initial test(s) of choice to delineate between pre- All of these are part of the oral cavity except (A) floor of mouth (B) soft palate (C) base of tongue (D) upper gingivae (E) retromolar trigone Answer C. Explanation: The oral cavity is bounded by the vermilion border of the lips and the junction of the hard and soft palate and circumvallate papillae. It can be thought of having eight subunits: lips, buccal mucosa, floor of mouth, anterior two-thirds of the tongue (i.e., oral tongue), upper and lower alveolar ridges, hard palate, and retromolar trigone. The retromolar trigone is a triangular spaced area from the distal surface of the last molar tooth to the maxillary tuberosity. This area is important in cancer spread as the mucosa of the mandible is tightly adherent to the underlying periosteum and therefore a weak barrier to tumor extension. The vestibule is the area lateral to the alveolar ridges and the oral cavity proper the area medial to the teeth. The layers of the cheek itself from superficial to deep are as follows: skin, subcutaneous tissue, the buccinator muscle, the buccinator fat pad, the pharyngobuccal fascia, and the mucosa/lip complex. The salivary ducts traverse the mucosa to drain into the oral cavity. These include Stensen's duct of the parotid gland, the papilla of which is located lateral to the second molars; Wharton's duct of the submandibular gland which is found in the midline floor of mouth adjacent to the frenulum of the tongue; and ducts of Rivinius of the sublingual gland which drain into the floor of mouth or into Wharton's duct itself. The treatment of choice for cystic hygromas is (A) Observation (B) Antibiotics (C) Intralesional sclerotherapy (D) Surgical excision Answer D. Explanation: The diagnosis of cystic hygroma by prenatal ultrasound (US) before 30 weeks' gestation has detected a "hidden mortality," as well as a high incidence of associated anomalies, including abnormal karyotypes and hydrops fetalis. Occasionally, very large lesions can cause obstruction of the fetal airway. Such obstruction can result in the development of polyhydramnios by impairing the ability of the fetus to swallow amniotic fluid. In these circumstances, the airway is usually markedly distorted, which can result in immediate airway obstruction unless the airway is secured at the time of delivery. Orotracheal intubation or urgent emergency tracheostomy while the infant remains attached to the placenta, the ex utero intrapartum technique (EXIT) procedure, may be necessary to secure the airway. (See Schwartz 8th ed., Chapter 38, Neck Masses.) A 2-year-old child swallows a short straight pin and is brought to the emergency room (ER) by his parents. On examination, he is alert and able to control his secretions (i.e., saliva). He has not experienced any respiratory distress and is afebrile. What is the appropriate course of action? (A) see the child in the clinic again in 10 days (B) perform endoscopy if the pin is found in the stomach or esophagus on x-ray Answer E. Explanation: Young children make up the majority of patients suffering from foreign body aspiration: children under 3 account for between 70 and 80% of all foreign body aspirations. Children in this age group tend to explore with their mouths. Another factor is the lack of development of molars for grinding and lack of maturity of swallowing and airway protection processes. Boys outweigh girls by 2:1 in frequency. Whereas the most common airway foreign body is vegetable matter, esophageal foreign bodies are coins in 75% of cases. Others may include disc batteries, screws, tacks, nails, and other hardware items. Increasing in frequency are toy plastic parts. The esophagus has four layers: the mucosa, submucosa, inner circular layer of muscle, and outer longitudinal layer of smooth muscle. The upper 5 cm are skeletal muscle, the upper midsection is an overlap of striated (skeletal) and smooth muscle, and the lower half is smooth muscle. The myenteric plexus of Auerbach is found within muscle layers and the submucosal plexus of Meissner is found in the submucosa. Both plexi are parasympathetic in innervation. The mucosa of the esophagus contains stratified squamous epithelium with poor absortion and low level secretory functions. Because there is no serosa, the esophagus is relatively more A 19-year-old woman presents to the ER with few days history of fever and pain in the submandibular region. She says that over the last several hours she has been having more trouble speaking with pain in her tongue and is afraid to lie down. On oral examination, you see that the floor of mouth is indurated and swollen and very tender. The patient has very poor dentition but you do not appreciate an abscess. Her submandibular and submental regions are also tender and indurated with some fluctuance. What entity in the differential diagnosis are you most worried about? (A) Vincent's angina (B) Bezold's abscess (C) Ludwig's angina (D) a retropharyngeal abscess (E) submandibular and sublingual gland sialadenitis Answer C. Explanation: This scenario describes a neck space infection with abscess. Historically these types of infections were caused by pharyngeal or tonsillar infections with involvement of the PPC, but since the advent of antibiotics, these infections are treated early in their course. Most contemporary adult neck space abscesses are caused by odontogenic or salivary gland infections, although tonsillar and pharyngeal infections still account for the majority of pediatric neck space infections. Other etiologies include preexisting congenital anomalies (branchial cleft sinuses and the like), trauma, upper respiratory tract infections, iatrogenic causes, or spread from a superficial infection. The neck spaces are divided by fascial layers. The most superficial fascia is the superficial cervical fascia beginning at the zygomatic process and extending into the thorax. It envelops the platysma muscle and muscles of facial expression and is rarely involved in serious neck space infections. The next deeper layer is the superficial layer of the deep cervical fascia which covers the strap muscles, trapezius, SCM, major salivary glands, and muscles of mastication (temporalis, masseter, and pterygoids). This superficial layer of the deep fascia or "investing fascia" splits around the superior surface of the manubrium to form the suprasternal space of burns. A 14-year-old male is involved in a dirt bike accident in which he suffers a "clothesline" injury. On examination in the ER you see a 7 cm laceration in the anterior neck, subcutaneous emphysema, and a hematoma which does not appear to be expanding. He is unable to lay flat and has a muffled voice. On flexible laryngoscopy, you see diffuse but mild edema of the supraglottis and glottis, reduced vocal cord abduction, and bloody secretions in the subglottis. Initial management of this patient would involve (A) nasal intubation, laryngeal and cervical spine CT, exploration and repair with intraoperative tracheotomy (B) tracheostomy under local anesthesia, cervical spine series, endoscopy, exploration and repair (C) percutaneous tracheostomy, cervical spine series, exploration and repair with stenting (D) oral intubation, laryngeal and cervical spine CT, endoscopy, exploration and repair (E) tracheostomy under general anesthesia, CT of the larynx and cervical spine, endoscopy, exploration and repair with stenting over a T-tube Answer B. Explanation: External laryngeal trauma is diagnosed on the basis of history and physical findings. A patient who presents with evidence of anterior neck trauma should be assumed to have upper airway trauma. This compounded with subcutaneous emphysema, voice changes, and orthopnea should arouse suspicion for disruption of the larynx or trachea. As in any trauma situation, the "ABCs" come first: airway, breathing and circulation. Although on fiberoptic examination this patient had "mild edema" it is presumable early after the trauma and the entire injury may have not evolved. There is potential for worsening of the edema and bleeding in the next 8–12 h. As a result, an awake tracheostomy is the best option. The addition of general anesthesia in this situation may cause laryngospasm and resultant complete airway obstruction. In addition, "clothesline" injuries are high risk for being associated with laryngotracheal separation. Any situation in which this is considered precludes oral or nasal intubation as intubation may worsen the existing damage or convert a partial laryngotracheal or cricotracheal separation into a complete separation. The pathophysiology behind blunt trauma to the larynx involves crushing of the laryngeal skeleton against the cervical spine. There is a shearing effect A 20-year-old man involved in an altercation presents to the ER with epistaxis and nasal airway obstruction. When inspecting his nose externally, you feel crepitus when moving the nasal bones and mild flattening of the dorsum; there is no active bleeding. On anterior rhinoscopy, you see an ecchymotic, swollen area on either side of the caudal septum (Fig. 14-6). The next step in management would be to (A) reduce the nasal fracture externally and employ an external nasal splint (B) place internal nasal splints to stabilize the fracture (C) drain the septal hematoma (D) place anterior nasal packing to treat the epistaxis (E) get facial x-rays if they were not already performed Answer C. Explanation: A history of trauma to the nose with epistaxis should raise concern for a nasal fracture. Signs of crepitus of the nasal cartilaginous and bony framework and obvious external deformity are virtually pathognomic for a nasal fracture. The nasal bone is the most frequently fractured facial bone. Diagnosis rests on the physical examination especially after topical decongestion; x-rays have not been helpful in adding to diagnostic accuracy. In nearly 50% of cases, nasal x-rays may not reveal a fracture when one is actually present. Photographic documentation is important, however. A careful rhinoscopic examination should be performed as there are few injuries and/or complications associated with nasal trauma to the nose that require immediate repair or attention. One of these is the septal hematoma (Fig. 14-6). A septal hematoma presents with nasal airway obstruction, usually bilaterally. Less often do patients with a septal hematoma present with epistaxis. The hematoma develops in the plane between the perichondrium of the septal cartilage and the cartilage itself. As the cartilage receives its blood supply from the perichondrium, the hematoma causes ischemic injury and eventually degeneration of the cartilaginous septum. A devastating cosmetic and functional consequence of this is the A 60-year-old male with a history of hypertension and coronary artery disease presents to the ER with steady bleeding from the right nare. He is on aspirin 325 mg a day as well as Plavix; he had a percutaneous transluminal coronary angioplasty (PTCA) with stenting 5 years ago. You first examine him and are not sure where the bleeding is arising from so you place an anterior nasal pack. He has no bleeding until 20 min later, but then Answer C. Explanation: Epistaxis or nosebleeding is one of the most common ear, nose and throat (ENT) emergencies. The role of the nose in humidification, filtration and warming of inspired air and its copious blood supply all put it at risk for bleeding. Epistaxis more commonly occurs in older individuals because of vessel wall aging with fibrosis and slower vasoconstriction and in the winter months because of cold, dry air exposure. Other risk factors include trauma (nose picking, most common in children), nasal sprays including nasal steroids, intranasal or sinus tumors, allergies, medications such as antiplatelet agents and anticoagulants, and anatomic deformities such as septal deviation. Systemic factors and diseases putting patients at epistaxis risk include hypertension, hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease, an autosomal dominant disease with associated mucosal telangiectasias and pulmonary AVMs), von Willebrand disease, hemophilia, nutritional deficiencies, alcohol abuse with associated hepatic disease, and lymphoreticular disorders or malignancies. Epistaxis most commonly occurs in the anterior portion of the nasal cavity, specifically the septum and the area known as Kiesselbach's plexus (in 90%). This area is particularly susceptible to trauma and drying effects. The first step in management of epistaxis is fluid resuscitation and control Nasal blood supply. Major nasal blood vessels and their relative positions are depicted. Note that the nasal sept um has been reflected superiorly. A, Anterior ethmoidal artery; B, Posterior ethmoidal artery; C, Posterior septal nasal artery; D, Lateral nasal artery; E, Sphenopalatine artery; F, Sphenopalatine foramen; G, Greater palatine foramen; H, Greater palatine artery; I, Incisive canal. A 47-year-old man is brought to the physician's office by his wife who is having difficulty sleeping because of her husband's extremely loud snoring. He does complain of headaches and daytime sleepiness as well as some irritability. On examination, his collar size is 18 in. and he is moderately obese. In addition you note a septal deviation to the right and an elongated redundant uvula and posterior pharyngeal mucosa. You obtain a polysomnogram because you suspect sleep apnea: the patient's RDI is 40 with a low saturation of 80%. Appropriate treatment options include all of the following except: (A) nasal continuous positive airway pressure (CPAP) (B) septoplasty with uvulopalatopharyngoplasty (UPPP) (C) encourage weight loss as the sole treatment (D) orthodontic devices in conjunction with CPAP (E) tracheostomy Answer C. Explanation: In the United States, OSA has a prevalence of 4% in men and 2% in women. There are several systemic consequences to sleep apnea including hypertension, myocardial infarction, and stroke. Patients with sleep apnea have three to seven times the risk of having motor vehicle accidents. As a result of these statistics, sleep apnea is being diagnosed earlier and treated aggressively. There is a continuum of sleep disordered breathing which ranges from sleep apnea to the Pickwickian's syndrome. OSA is caused by an obstruction at any level of the upper airway above the glottis. The muscle relaxation occurring in the deeper stages of sleep occurs in the upper airway as well and patients predisposed to OSA have excess tissue in the upper airway, causing an airway collapse during inspiration. The patient is then awakened by desaturation, signaled as a snorting or gasping noise, and then resumes the pattern. The RDI is the respiratory disturbance index which is obtained by polysomnography. An RDI of greater than 5 is abnormal. Apnea itself is defined as cessation of airflow for at least 10 s, and hypopneas are desaturations without complete cessation. The RDI is the number of apneas and hypopneas in 1 h. This measure allows stratification of Which of the following is an indication for tonsillectomy? (A) Patient's request (B) Chronic middle ear infection (C) Three or more infections per year (D) Missing more than one week of school per year Answer C. Explanation: Tonsillectomy and adenoidectomy are indicated for chronic or recurrent acute infection and for obstructive hypertrophy. The American Academy of Otolaryngology–Head and Neck Surgery Clinical Indicators Compendium (2000) suggests tonsillectomy after three or more infections per year despite adequate medical therapy. Some feel that tonsillectomy is indicated in children who miss 2 or more weeks of school annually secondary to tonsil infections. Multiple techniques have been described, including electrocautery, sharp dissection, laser, and radiofrequency ablation. There is no consensus as to the best method. In cases of chronic or recurrent infection, surgery is considered only after failure of medical therapy. (See Schwartz 8th ed., Chapter 17, Benign Conditions of the Head and Neck.) A 50-year-old man has a 2-day history of headaches and of proptosis with failing vision in the right eye. Vision has been reduced to light perception only and the globe is displaced inferior and laterally. Rhinoscopy shows swelling in the middle meatus with some purulence. The next step in management would be to (A) obtain a CT scan of the orbits and sinuses and immediate ethmoidectomy (B) IV aqueous penicillin G, 2 million U every 4 h (C) IV levaquin 500 mg every 24 h (D) immediate exploration of the orbits (E) oral dexamethasone, 4 mg daily for 1 week Answer A. Explanation: The most common complication of acute sinusitis necessitating immediate operative intervention involves the eye. All the sinuses can be culprits of orbital complications but the ethmoid is the most common because of its adjacency. The indication in this patient to operate immediately would be the visual acuity change as complications can lead to blindness. As the ethmoids are the culprit, decompressing the infection or abscess if present can be performed via the lamina papyracea, the medial wall of the orbit. Infections spread by direct extension and thrombophlebitis of ethmoidal veins. Other complications may include neurologic infections: subdural and epidural abscesses and meningitis. Orbital complications are stratified by the Chandler classification system. Stage I is simply inflammatory edema or preseptal cellulitis (orbital septum of the eyelid) of the lids and extraocular muscles are not involved. Stage II indicates orbital cellulitis with edema of the contents of the orbit. The first two stages should be aggressively treated with medical therapy with antibiotics against Streptoccocus pneumoniae and Haemophilus influenzae to prevent progression to stage III. Stage III is the subperiosteal abscess which is beneath the periosteum of the lamina papyracea; the globe is displaced inferolaterally and vision is affected. Stage IV is an Orbital complications are typically treated with an external approach rather than and endoscopic approach although the trend is changing. Since the ethmoid sinuses are the most frequently involved, at minimum, an external ethmoidectomy is performed with removal of a portion of the lamina papyracea. Acute bacterial rhinosinusitis is diagnosed by the symptomatology of nasal congestion and rhinorrhea lasting for 7–14 days. Other symptoms include facial pain or dental pain, headache, fever and malaise. Anterior rhinoscopy may reveal unilateral or bilateral purulent drainage and tenderness on palpation of soft tissue over the sinuses. Various processes may lead to acute or chronic sinusitis. The first is obstruction of sinus ostia which can be caused by anatomic factors (septal deviation), edema from allergens or polyps. The second process is ciliary dysfunction either primary or acquired such as after a viral upper respiratiory infection (URI). The last is changes in mucus quality or quantity systemic factors may include steroid use, diabetes or immune compromise in general. Nosocomial sinusitis may be caused by indwelling nasogastric catheters or nasotracheal intubation. A critically ill patient may present with a fever of unknown origin; acute rhinosinusitis should be given careful consideration, usually with an original or reconstructed coronal CT scan (optimal images for sinuses). These patients should be treated for gram-positive and gram- The most likely pathogen to be involved with supraglottitis (epiglottitis) is (A) Streptoccocus pneumonia (B) H. influenzae (C) influenza virus (D) parainfluenza virus (E) S. aureus Answer A. Explanation: Le Fort I fractures occur transversely across the alveolus, above the level of the teeth apices. In a pure Le Fort I fracture, the palatal vault is mobile while the nasal pyramid and orbital rims are stable. The Le Fort II fracture extends through the nasofrontal buttress, medial wall of the orbit, across the infraorbital rim, and through the zygomaticomaxillary articulation. The nasal dorsum, palate, and medial part of the infraorbital rim are mobile. The Le Fort III fracture is also known as craniofacial disjunction. The frontozygomaticomaxillary, frontomaxillary, and frontonasal suture lines are disrupted. The entire face is mobile from the cranium. It is convenient to conceptualize complex midface fractures according to these patterns; however, in reality, fractures reflect a combination of these three types. (See Schwartz 8th ed., Chapter 17, Trauma of the Head and Neck.) Le Fort II fracture entails injuries to all of the following EXCEPT (A) Medial wall of the orbit (B) Alveolus (C) Zygomaticomaxillary articulation (D) Nasofrontal buttress (E) Mandible Answer A. Explanation: Le Fort I fractures occur transversely across the alveolus, above the level of the teeth apices. In a pure Le Fort I fracture, the palatal vault is mobile while the nasal pyramid and orbital rims are stable. The Le Fort II fracture extends through the nasofrontal buttress, medial wall of the orbit, across the infraorbital rim, and through the zygomaticomaxillary articulation. The nasal dorsum, palate, and medial part of the infraorbital rim are mobile. The Le Fort III fracture is also known as craniofacial disjunction. The frontozygomaticomaxillary, frontomaxillary, and frontonasal suture lines are disrupted. The entire face is mobile from the cranium. It is convenient to conceptualize complex midface fractures according to these patterns; however, in reality, fractures reflect a combination of these three types. (See Schwartz 8th ed., Chapter 17, Trauma of the Head and Neck.) Le Fort II fracture entails injuries to all of the following EXCEPT (A) Medial wall of the orbit (B) Alveolus (C) Zygomaticomaxillary articulation (D) Nasofrontal buttress (E) Mandible Answer B. Explanation: Despite the advent and widespread use of the HIB vaccine, H. influenzae type b still remains the most common cause of epiglottitis. Historically, the disease was more common in children between ages 2 through 6; however, with vaccine use, the incidence in children has dropped from 3.5 in 100,000 to 0.6 in 100,000, whereas that in adults has remained the same or has risen slightly. Other bacteria that are found commonly include other types of H. influenzae, -hemolytic streptococci, Staphylococcus, Klebsiellae pneumoniae, Bacteroides melanogenicus, and Mycobacterium tuberculosis. The presentation in children is fever, sore throat of a rapid onset with inspiratory stridor; adults will also complain of odynophagia. The key is the rapid onset of pain with a paucity of oropharyngeal findings (such as lack of evidence of acute tonsillitis or peritonsillar abscess). Children may have trouble handling secretions and may drool and patients in general may have a muffled or "hot potato" voice all related to edema of the epiglottis. Patients sit forward and upright in a "sniffing" position to relieve some of the respiratory obstruction. Diagnosis is based chiefly on history and physical examination. Though a classic "thumbprint" sign of the epiglottis on lateral neck x-ray has been described in the setting of supraglottitis, the sensitivity of lateral neck films A 12-year-old female presents for evaluation of a neck mass. Which of the following pairs are correct? (A) branchial cleft cyst/sinus: most commonly involves the third branchial cleft remnant (B) thyroglossal duct cyst (TGDCs): mesodermal remnants that produce lateral swelling over neck (C) cystic hygroma: a salivary gland disorder related to a hypersecretory cyst (D) torticollis: unilateral shortening of trapezius muscle (E) medullary thyroid cancer: most common cause of death in multiple endocrine neoplasia (MEN) 2B Answer E. Explanation: Commonly encountered developmental neck abnormalities in children are of congenital origin yet may not cause problems or be detected until adulthood. While some of these neck lesions may appear asymptomatic at birth, they may precipitously become enlarged and disfiguring as a result of local or regional infection or hemorrhage. Developmental abnormalities of the branchial apparatus represent a common source of congenital lateral neck masses. Branchial anomalies may present as a cyst, sinus, or fistula. Branchial cleft anomalies arise most commonly (greater than 90%) from the second branchial cleft system. Eight percent arise from the first branchial anomaly whereas third and fourth branchial malformations are rare. Usually the second branchial cleft sinus or fistula presents with drainage from a small pit in the skin just anterior to the lower third of the sternocleidomastoid muscle. Treatment of choice is surgical excision due to the risk of infection (Fig. 34-27). Answer E. Thyroglossal duct cysts (TGDCs) represent the most common head and neck midline masses in children. It is reported that they account for about 70% of all congenital neck abnormalities. TGDCs are embryonic ectodermal rests that can present as midline structures as they follow the descent along the thyroid gland tract. Normally, the thyroglossal duct regresses once the thyroid gland reaches the anterior neck. Faulty thyroid migration or persistence of the thyroglossal duct can lead to the formation of lingual/ectopic thyroid tissue, pyramidal thyroid lobe, or a TGDCs. Since TGDCs are attached to the hyoid bone, clinical presentation typically shows a midline mass that moves with swallowing. Treatment is based on the Sistrunk procedure in which complete surgical excision of the cyst and tract up to the base of the tongue including the central portion of the hyoid bone is preformed (see Fig. 34-28). Answer E. Lymphatic malformations commonly referred to as cystic hygromas are developmental abnormalities of the lymphoid system that occur at sites of lymphatic-venous connection, most commonly in the posterior neck (Fig. 34-29). The cysts may become enlarged and disfiguring not only as a result of infection or hemorrhage but also due to increases in fluid and endothelial cell growth. Imaging by US, CT, and MRI (for complex and extensive lesions) is mandated to determine whether involvement of deeper airway structures is present. This also gives pertinent clues as to the planning of the operative approach. When these lesions are diagnosed prenatally, the overall prognosis is poorer than those diagnosed after birth. Treatment of these lesions is primarily surgical but another therapy is injection sclerotherapy with such agents as bleomycin, OK-432, sodium morrhuate, 22.5% glucose, and triamcinolone. Sclerotherapy is usually reserved for extensive disease or recurrences. Torticollis is a deformity characterized by the unnatural tilted or turned position of the head. The most common form is due to shortening of the sternocleidomastoid muscle, although a number of other conditions can potentially cause torticollis (cervical hemivertebrae, adenitis, fascitis, and oculomotor abnormalities). Birth trauma was once thought to contribute to the cause of torticollis by injury to the sternocleidomastoid or the spinal accessory nerve, but this is rarely the case. The mother or primary physician usually notes the classic presentation of an otherwise healthy 2–8-week-old infant who preferentially turns their head to one side. Compete resolution of untreated torticollis occurs in 50–70% of cases by 6 months of age, but because it is difficult to predict which infants will develop an irreversible deformity, a passive range-of-motion exercise regimen is advocated. In cases that present with or develop facial hemihypoplasia, surgery to divide the sternocleidomastoid on the affected side is indicated Answer E. Medullary thryroid cancer can occur sporadically, in association with MEN types 2A or 2B, or with the familial medullary cancer syndrome. A mutation in the ret protooncogene in individuals with MEN and the familial variant predisposes family members (autosomal dominant inheritance) to the development of medullary thyroid cancer at an early age. This tumor is the first to develop in MEN children and is the most common cause of death. In these children, early thyroidectomy is advocated after the genetic mutation has been confirmed. MEN 2A children should undergo thyroidectomy prior to 5 years of age; whereas children of MEN 2B require thyroidectomy prior to 1 year of age due to the more virulent nature of the disease. An 80-year-old woman who is a nursing home patient is brought to the hospital with a GI bleed. She ultimately undergoes a left hemicolectomy for diverticulosis and has a lengthy postoperative ileus. Postoperative day 5 she complains of a sour taste in her mouth and her right cheek feeling warm and very tender. You notice a swelling in the parotid area and that she is febrile at the time. All of the following would be part of the treatment of this disorder except: (A) IV antibiotics against S. aureus (B) heat application to the area over the parotid (C) IV hydration (D) lemon drops (E) cannulation of the right Stensen's duct with drainage Answer E. xplanation: This case is typical of acute bacterial parotitis or sialadenitis. This disorder occurs in individuals with dehydration from any cause. The dehydration may be a result of being NPO for an extended period of time or in the patient being in a relative state of anorexia after surgery and patients who have undergone abdominal procedures are at the most risk. Chronic and/or debilitating illnesses also may predispose a patient to development of acute parotitis such as in the case of a nursing home patient. Other causes may be radiation, chemotherapy or immunosuppression in general, medications with anticholinergic side effects, and Sjogren's disease. The incidence is reported at approximately 1 in 1–2000 operative procedures. Acute parotitis presents with symptoms of pain, erythema, and diffuse enlargement of the gland which is usually unilateral; gentle milking of Stensen's duct with manual pressure on the gland and intraorally causes purulent exudate to be expressed from the orifice. The pathophysiology of acute parotitis is retrograde bacterial infection through Stensen's duct. Mucoid saliva which has a high molecular weight glycoprotein and sialic acid has superior bacteriostatic activity because of the ability to trap bacteria. Mucoid saliva also has a higher lysozyme and Which of the following statements concerning cleft lip and cleft palate is true? (A) Cleft lip is a midline failure of lip closure. (B) Development of cleft lip is related to environmental factors and not to familial tendencies. (C) Deformities of the nose occur in approximately 50% of patients who have a cleft lip. (D) Middle ear infections are common Answer D. Explanation: The incidence of cleft palate, cleft lip, or both is variously reported as 1 in 1000 to 1 in 2500 live births in the United States. If a parent or sibling has a cleft lip, the chance of a subsequent child's being born with the same defect is higher. Cleft lip may be unilateral or bilateral when the nasomedial and nasolateral processes fail to unite during embryologic development. Cleft palate is due to isolated failure of palatal process fusion. Almost all cleft lips, even minor ones, are associated with nasal distortions, and many plastic surgeons advocate rhinoplasty at the time of repair of the cleft lip. Malocclusion is a uniform problem, and all patients with cleft palates have drainage problems of the middle ear, which may lead to recurrent ear infections. Normal speech is achieved in more than 75% of cases of corrective surgery in which the cleft palate is closed entirely by the age of 12 to 14 months. (See Schwartz 7th ed.) What study is used to monitor response to therapy for malignant otitis externa? (A) technetium-99 scan (B) gallium-67 scan (C) CT scan (D) MRI (E) culture Answer B. Explanation: Malignant otitis externa (or necrotizing otitis externa, NOE) does not refer to a neoplastic process but rather a potentially lifethreatening infectious external ear infection. Though newer antibiotics have somewhat decreased the incidence, there are certain patient groups at risk. These at-risk groups are the elderly, diabetics, and the immunocompromised. In fact, up to 80% of cases are found in diabetics. NOE is associated with a skull base osteomyelitis which is the source of its lethal nature. Diagnosis rests on a few key symptoms and signs. These include a persistent and severe otalgia that has lasted for more than 1 month, purulent otorrhea with granulation tissue for several weeks, immunocompromised because of age, diabetes or other condition and a lower cranial neuropathy of nerves VII, IX, X, or XI. The granulation tissue is seen at the posteroinferior aspect of the external auditory canal at the tympanomastoid suture line. The granulation tissue seen in an AIDS patient is less exuberant but suspicion should be maintained, as these patients are usually severely immunocompromised. Granulation tissue can be seen in severe otitis externa when there is a tympanic membrane perforation. SCC can present in a similar fashion, so biopsies should be What structure passes through the foramen ovale? (A) infraorbital nerve (B) V3 (C) meningeal artery (D) sphenopalatine artery (E) V2 Answer B. Explanation: The skull base is a complex anatomical region which houses multiple vital structures. Any disease process in this region has the potential to affect the function of the various contents of the skull base foramina. The skull base can be simplified by separating it into an anterior, middle, and posterior cranial fossa (Fig. 14-27). FIG. 14-27 Skull base foramina from internal aspect. (Source: Reprinted from Lee, et al. Essential Otolaryngology Head and Neck Surgery, 8th ed., copyright 2003, with permission from McGraw-Hill). The anterior cranial fossa (ACF) is the most shallow. The main component is the frontal bone and the floor is chiefly composed of the orbital plates of the frontal bone and ends at the anterior border of the greater wing of sphenoid. The fovea ethmoidalis is the portion of the ethmoid sinuses that forms part of the ACF floor. The main foramina of the ACF are those in the cribriform plate which transmit the olfactory nerve axons. Other important foramina are those for the anterior and posterior ethmoidal neurovascular bundles. The optic nerve is located 5–6 mm behind the posterior ethmoidal artery. A vestigial foramen cecum is seen between the crista galli and frontal crest and in 1% it is open and transmits a nasal emissary vein. Answer B. Explanation: The skull base is a complex anatomical region which houses multiple vital structures. Any disease process in this region has the potential to affect the function of the various contents of the skull base foramina. The skull base can be simplified by separating it into an anterior, middle, and posterior cranial fossa (Fig. 14-27). FIG. 14-27 Skull base foramina from internal aspect. (Source: Reprinted from Lee, et al. Essential Otolaryngology Head and Neck Surgery, 8th ed., copyright 2003, with permission from McGraw-Hill). The anterior cranial fossa (ACF) is the most shallow. The main component is the frontal bone and the floor is chiefly composed of the orbital plates of the frontal bone and ends at the anterior border of the greater wing of sphenoid. The fovea ethmoidalis is the portion of the ethmoid sinuses that forms part of the ACF floor. The main foramina of the ACF are those in the cribriform plate which transmit the olfactory nerve axons. Other important foramina are those for the anterior and posterior ethmoidal neurovascular bundles. The optic nerve is located 5–6 mm behind the posterior ethmoidal artery. A vestigial foramen cecum is seen between the crista galli and frontal crest and in 1% it is open and transmits a nasal emissary vein. Pott's puffy tumor is seen most commonly with which of these conditions? (A) otitis media (B) frontal sinus fracture (C) ethmoid sinusitis (D) bacterial pharyngitis (E) cervical spinal infection Answer B. Explanation: Pott's puffy tumor is a term used to describe a soft tissue swelling because of a subperiosteal abscess over the region of the frontal sinus. This occurs when the anterior table of the frontal sinus is involved in an osteomyelitic process which is usually because of a sinusitis but may be a result of a mucocele from a fracture. The offending organism in many cases is S. aureus. A malignancy of the frontal sinus, though exceedingly rare, should be considered in the differential. The pathophysiologic of development of a mucocele with subsequent osteomyelitis is an obstructed frontal sinus outflow tract. This occurs by thrombophlebitis of the diploic veins of the frontal bone or via direct extension. The treatment of frontal sinus fractures depends on which table(s) of bone are fractured and the degree of displacement or comminution. Nondisplaced noncomminuted anterior table fractures can usually be observed unless CT scan shows persistent opacification, in which case endoscopic exploration or trephination of the sinus may be warranted. Displaced anterior table fractures produce obvious cosmetic deformity and can be reduced with low profile miniplates and preservation of as much native bone as possible. Nondisplaced posterior table fractures that do not cause CSF leaks can be observed with antibiotic treatment. Indications for Answer B. Mucoceles can develop several years after the initial fracture, the average being 7.5 years. Other complications of frontal sinus fractures include sinusitis, headache, forehead numbness (from supraorbital or supratrochlear nerve trauma), meningitis, brain abscess, cosmetic deformity, and diplopia and eye pulsations in the event of a carotid-cavernous fistula. Other intracranial complications of sinusitis in general include meningitis, epidural, subdural and intracerebral abscesses, and superior sagittal sinus thrombosis as well as Pott's puffy tumor. Pott's abscess is an eponym to describe tuberculosis of the spine and the other answer choices are merely distractors. The overall success rate of cervical myotomy for patients with a pharyngoesophageal swallowing dysfunction is (A) 20% (B) 35% (C) 65% (D) 90% Answer C. Explanation: The more liberal application of myotomy to problems of the oropharyngeal phase of swallowing has resulted in an overall success rate in the relief of symptoms of only 64%. When patients are selected using radiographic or motility markers of disease as outlined above, it is unusual for patients not to see benefit. (See Schwartz 8th ed., Chapter 24, Motility Disorders of the Pharynx and Esophagus.)