Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
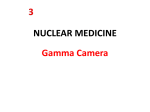
Source: STANDARD HANDBOOK OF BIOMEDICAL ENGINEERING AND DESIGN CHAPTER 27 NUCLEAR MEDICINE IMAGING INSTRUMENTATION Mark T. Madsen University of Iowa, Iowa City, Iowa 27.1 INTRODUCTION 27.1 27.2 SCINTILLATION CAMERAS 27.3 SPECT SYSTEMS 27.14 27.4 SUMMARY 27.20 REFERENCES 27.20 27.2 27.1 INTRODUCTION Nuclear medicine is a diagnostic imaging modality that is used to obtain clinical information about most of the major tissues and organs of the body. Diagnostic information is obtained from the way the tissues and organs process radiolabeled compounds (radiopharmaceuticals). The radiopharmaceutical is typically administered to the patient though an intravenous injection. The radiopharmaceutical is carried throughout the body by the circulation where it localizes in tissues and organs. Images of these distributions are acquired with a scintillation camera. Ideally, the radiopharmaceutical would go only to abnormal areas. Unfortunately, this is never the case and the abnormal concentration of the radiotracer is often obscured by normal uptake of the radiopharmaceutical in the surrounding tissues. Images of higher contrast and better localization can be obtained with tomographic systems designed for nuclear medicine studies (SPECT systems). These are described in detail below. The imaging of radiotracers in the body presents special challenges that are unique. The flux of gamma rays available for imaging is orders of magnitude less than that used in x-ray radiography or x-ray computed tomography (CT). In addition, the high energy of the gamma rays makes detection more difficult. As a result, the images produced in nuclear medicine studies are much noisier and have worse spatial resolution. In order to appreciate these problems and how they affect the design of nuclear medicine imaging devices, we will briefly review the physics of gamma ray interactions.1 The intensity of gamma rays traveling through material is gradually reduced by absorption or scattering. This loss of gamma rays is referred to as attenuation and is described by the exponential equation (27.1) where I0 = initial intensity †††††††I(x) = intensity of rays after traveling a distance x through the material ††††††††††µ = linear attenuation coefficient of the material 27.1 Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.2 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION Over the range of gamma ray energies used in radionuclide imaging, the two primary interactions that contribute to the attenuation coefficient are photoelectric absorption and Compton scattering. Photoelectric absorption refers to the total absorption of the gamma ray by an inner shell atomic electron and is the primary interaction in high-Z materials such as sodium iodide (the detector material used in the scintillation camera) and lead. In low-Z materials such as body tissues, its contribution to attenuation is relatively small. Compton scattering occurs when the incoming gamma ray interacts with a loosely bound outer shell electron. A portion of the gamma ray energy is imparted to the electron and the remaining energy is left with the scattered photon. The amount of energy lost in the event depends on the angle between the gamma ray and scattered photon. Compton scattering is the dominant interaction in body tissues. High attenuation is desirable in detecting and shielding materials. Ideally materials used for these purposes would absorb every gamma ray. In the body, attenuation is very undesirable, but unfortunately, unavoidable. Attenuation reduces the intensity of gamma rays available for detection and scattered radiation that reaches the detector causes a significant loss of contrast. 27.2 SCINTILLATION CAMERAS The scintillation camera is the primary imaging instrument used in nuclear medicine and is often referred to as a gamma camera. 2 The scintillation camera is a position-sensitive gamma ray imager. Although the entire field of view is available for detection, it processes one event at a time. The spatial resolution is approximately 10 mm and it yields a count rate of 200 to 300 cpm/µCi in the field of view (cpm = counts per minute). The field of view covers a large portion of the body and is typically 40 ◊ 50 cm, although other sizes are available. The rectilinear scanner was the first practical nuclear medicine imaging device and it was still in use through the 1970s. It was invented by Benedict Cassen in 1950. The rectilinear scanner used the detected count rate of a radiation detector to control the brightness of a small light bulb masked to expose a small area of a film. The movement of the radiation detector and the bulb were linked so that, as the detector moved in a raster pattern over the patient, the bulb tracked a corresponding path over the film. The developed film revealed the internal distribution of the radiopharmaceutical sampled by the scanning probe. While the invention of the rectilinear scanner was a major step forward, it had several shortcomings that were inherent in its design. Because it sampled only one small area at a time, image acquisitions took a long time (10 to 20 minutes). In addition, only static imaging was possible. Dynamic studies, such as those that followed the progression of a tracer through the body, required an imaging system with a large field of view where all areas are equally sampled, i.e., a scintillation camera. The first scintillation camera was developed by Hal O. Anger in 1958.3 Although this system was very crude, it contained the fundamental components of all future designs: NaI(Tl) as the primary detector and weighted signals from an array of photomultiplier tubes to determine the location of detected events. Table 27.1 gives typical performance values for a modern scintillation camera. The gamma rayñsensitive element of the scintillation camera is a large, thin piece of NaI(Tl). Although the crystals originally had a circular cross section, most scintillation cameras now use a rectangular crystal with dimensions as large as 40 ◊ 50 cm. The thickness of NaI(Tl) in most conventional cameras is 9.5 mm, but in systems that are used for coincidence detection, the crystal may be twice as thick. NaI(Tl) is a scintillator; It converts gamma ray energy into visible light. The amount of light generated is directly proportional to the absorbed energy. NaI(Tl) is very efficient at this and the absorption of one 140-keV gamma ray will yield 5000 visible light photons. There are a number of advantages associated with NaI(Tl) in addition to its high light output. It efficiently absorbs 140-keV gamma rays (with a photopeak efficiency of 85%) and it has a moderate energy resolution. Energy resolution is an important property since it provides the means to discriminate against scattered radiation. Gamma rays that undergo scattering within the patient degrade the quality of images. However, scattered gamma rays necessarily have less energy than unscattered gamma rays and can be selectively eliminated on that basis. Another positive feature of NaI(Tl) is that it can be Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.3 TABLE 27.1 Scintillation Camera Specifications manufactured in many shapes and sizes. There are disadvantages though. NaI(Tl) actively absorbs water vapor from the air and loses its transparency. It must be hermetically sealed, and loss of this seal results in irreparable damage. Another disadvantage is that the persistence of the scintillation is long enough that it limits the count rate that the crystal can accurately handle. Most nuclear medicine imaging is performed far below this limit. However, some first pass studies do result in significant count rate losses from this limit. The biggest problem is encountered in coincidence imaging. Converting the gamma ray energy to visible light is only part of the battle. In order for the information from the scintillation to be useful, it has to be converted into an electronic signal. This is accomplished with a photomultiplier tube (Fig. 27.1). The photomultiplier tube is a vacuum tube with a photoemissive surface called the photocathode. Visible light hitting this surface knocks off electrons. These electrons are accelerated to an electric terminal called a dynode. The first dynode has FIGURE 27.1 Photomultiplier tube. The photomultiplier tube converts the scintillation into an electronic pulse preserving the linear relationship between the magnitude of the scintillation and the energy of the interaction. The location of a source can be inferred from the magnitude of the signal change. The relationship between the signal magnitude and source position is nonlinear, and positioning errors occur both when the source is far from the PMT and when it is directly under it. The ideal response can be approximated with the use of a light pipe. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.4 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION a potential approximately 100 volts higher than the photocathode, and the electrons hit it with enough force to knock off about 4 more new electrons. The next dynode is another 100 volts higher, so the process is repeated. The same process occurs over a total series of nine dynodes resulting in a signal amplification of 1,000,000. Proportionality is maintained throughout this amplification so that the size of the electron pulse is directly proportional to the energy deposited by the gamma ray. A scintillation camera needs to be able to record gamma ray events over a large area. This requires uniform sampling by an array of photomultiplier tubes (PMTs). The PMTs are arranged in a close packed array that covers the entire surface of the NaI(Tl) crystal (Fig. 27.2). The PMTs used in scintillation cameras are usually 2 or 3 in across, so that as many as 120 PMTs may be used. PMTs have been manufactured in variety of different cross sections in order to maximize their areal coverage. Circular, hexagonal, and square tubes have all been used. The signals obtained from the PMTs will be used to determine two important properties about the gamma ray interaction: where did it occur and how much energy was deposited? At first blush, it may seen that even 2-in PMTs are too coarse to determine the event location. However, we will see that magnitude of the PMT output is fairly sensitive to the location of a source. FIGURE 27.2 Photomultiplier tube array. The photomultiplier tubes are arranged in a close-packed array to cover the back surface of the NaI(Tl) crystal. If a PMT is mounted to an NaI(Tl) crystal and the signal output is plotted as a source is moved from left to right, the result shown by the solid line (Fig. 27.1) will be obtained. When the source is positioned far from the PMT, the signal is weak and the location of the source is not certain. When the source is directly under the PMT, the signal is strong, but the dependence on the position is modest. However, when the source is just to the left or right of the PMT, the signal change with source location is large. Over this region, the location of the source can be accurately tracked. With only a single PMT, we could not tell if the source was on the left or right (or front or back), but by considering the signals from other surrounding PMTs, that can be determined. The main problem is what to do about the poor response near the center of PMT. What can be done to transform the measured PMT output into the ideal signal shown in Fig. 27.1? The early solution to this was to displace the PMTs from the NaI(Tl) crystal with a light pipe. A light pipe is a transparent material such as lucite or quartz that is interspersed between the crystal and PMT array. The displacement of the PMTs causes the light from the scintillations to spread out, yielding a more favorable signal output. To achieve even better results, some manufacturers have used special mask patterns on the front surface of the light pipe along with sculptured grooves in the back. These efforts pay off in more accurate positioning of the event locations; however, there is a price to pay. The effort to scatter the light also results in higher light losses, leading to increases in statistical fluctuations and ultimately degradations in spatial resolutions. In the early gamma cameras, there was no way around this dilemma. However, digital electronics provides the capability of Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.5 nonlinear mapping, which greatly reduces the demands put on the light pipe. This has allowed light pipes to be made very thin and even eliminated. Figure 27.3 shows a schematic of an analog scintillation camera. The scintillation light from an absorbed gamma ray is transmitted through to the photomultiplier tube array. The energy of the event is determined by summing all the photomultiplier tube signals. As will be seen, the energy signal is used both for scatter discrimination and for normalizing the position signals. The position of the event is determined by summing weighted outputs from each photomultiplier tube. These weighting factors are determined by the location of the photomultiplier tube in the array. Separate weighting factors are used for determining the x and y signals. This process is referred to as Anger logic, since it is the scheme developed by Hal Anger in the first scintillation camera. In the initial designs, literally all the photomultiplier tubes participated in the energy and position signal summations. It was subsequently found that the signals from photomultiplier tubes located far from the event contributed mostly noise. In modern designs, the photomultiplier tube signal must exceed a threshold before it is included in the sum. Another point that should be made is that all the processing is performed on each detected event. The decision to include the event as a valid count is not made until the end of the processing when the pulse height analysis is done. If the event falls within the selected energy window, the normalized x and y signals are available for either an analog display or digital storage. FIGURE 27.3 Analog scintillation cameras. The signals from each photomultiplier tube are sampled to determine both the position and energy of the detected event. Separate weighting factors are used for the x and y signal determinations. The energy signal is used to normalize the position signals and discriminate against scattered radiation. The position signals determined from summing the weighted PMT signals vary with the brightness of the scintillation, which itself depends on the energy absorbed in the crystal. This means that an object imaged with a high-energy gamma ray like I-131 (364 keV) will be magnified when compared to the same object imaged with Tc-99m (140 keV). This magnification is a concern even when only one gamma ray energy is imaged because of the finite energy resolution of the scintillation camera system. The pulse heights from the absorptions of identical gamma rays vary enough to cause slight minifications and magnifications, ultimately degrading spatial resolution. The solution to this problem is to normalize the position signals with the measured energy signal. This removes the image size dependence with energy, thereby improving spatial resolution and allowing the simultaneous imaging of more than one radionuclide without distortion. This feature is the primary component for guaranteeing good multiwindow spatial registration. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.6 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION As has been previously noted, gamma rays that are scattered within the patient have distorted spatial information and degrade image contrast. Because scattered gamma rays necessarily lose energy, they can be selectively avoided by accepting only events that have pulse heights corresponding to the primary gamma ray energy. The pulse height analyzer provides this capability. A ìwindowî is centered to cover 15 to 20 percent of the photopeak. All energy pulses that meet this criterion generate a logic pulse that indicates to the system that a valid event has occurred. This output enables the recording of the x and y position information in a computer or display. The precision of locating gamma ray events by a scintillation camera is referred to as intrinsic spatial resolution. The original Anger camera had very poor intrinsic spatial resolution (~12 mm full-widthhalf-maximum). With the improvement in electronics and pulse processing methods, the spatial resolution of the scintillation camera has improved steadily, approaching 3 mm in modern systems.4 These improvements include: better-quality, low-noise PMTs; improvements in the Anger logic electronics including signal thresholding; smaller PMTs, and improved PMT quality control. The most recent improvement has been the replacement of most of the analog processing with digital electronics. With improvements in the speed of digitization electronics and decreases in component costs, the trend in scintillation cameras has been to digitize the PMT signals (Fig. 27.4).5 The analog-to-digital converters assign a numeric magnitude to the PMT signals. All subsequent determinations of energy and positions can then be done by computer algorithms that can accurately model the nonlinear behavior of the PMT signals with source position. The success of this approach has allowed the reduction and even total elimination of the light pipe. This moves the PMTs closer to the scintillation, thereby improving both the precision of the position determination (i.e., spatial resolution) and the energy resolution. FIGURE 27.4 Digital scintillation cameras. By digitizing the output of the PMTs, the analog weighting electronics can be replaced by a nonlinear positioning algorithm. This allows a more accurate correction, culminating with the elimination of the light pipe. Once there is an x and y coordinate that locates a valid event, this information has to be stored as image data. Although it is possible on some scintillation camera systems to store the individual coordinates sequentially (referred to as list mode acquisition), most systems store the information directly in histogram or matrix mode. With this method, an array of computer memory, typically 128 ◊ 128 or 256 ◊ 256, is reserved for each image frame. The matrix elements or pixels are initially set to 0. The coordinates for each event point to one of the pixels and this pixel is incremented by 1. When the acquisition-stopping criteria are met, the image is complete. The information in the matrix is either gray-scale or color encoded to display the image data. The entire process is shown schematically in Fig. 27.5. A gamma ray originating in the patient is absorbed in the NaI(Tl) crystal. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.7 FIGURE 27.5 Scintillation camera. The scintillation camera processes each detected event to determine the x, y, and energy. If an event falls within the selected energy range, the memory location pointed to by the x and y coordinates is incremented. This process continues until the stopping criteria (number of counts or acquisition time) are met. The light from the scintillation is sampled by the PMT array, which determines both the x and y coordinates of the event and its energy. If the energy signal falls within the window of the pulse height analyzer, the x and y coordinates are used to increment the appropriate pixel. This process is repeated for every detected event. In order to form images with a scintillation camera, a collimator must be placed in front of the NaI(Tl) crystal. The collimator (Fig. 27.6) is the image-forming aperture of the camera system, and it is necessary for the imaging process. The collimator projects the gamma ray pattern originating in the patient onto the NaI(Tl) crystal. It does this by selectively absorbing gamma rays. The collimator is a close-packed array of holes in a lead plate. Most often the holes are parallel, but fanbeam converging and diverging collimators are available. Gamma rays whose trajectory takes them through a hole get to interact with the NaI(Tl). All the others are absorbed. The design of collimators depends on the gamma ray energy and the ever-present trade-off between count sensitivity and spatial resolution.6,7 Collimators used for imaging Tc-99m typically have holes that are 1 to 1.5 mm across and are 20 to 40 mm thick. Typical collimator design parameters are given in Table 27.2. Although a collimator is necessary for the formation of images, it represents the limiting factor in the both count sensitivity and spatial resolution of the scintillation camera. Because of the bruteforce absorption approach to forming images with collimators, they are very inefficient. Less than 1 in 5000 gamma rays that hit the front surface of the collimator get through to the crystal. To improve the count sensitivity, the collimator hole size could be increased and the hole length shortened. Unfortunately, these changes degrade the spatial resolution. The spatial resolution of the collimator is constrained by the geometry of the holes and is typically in the range of 6 to 8 mm at 10 cm when used with Tc-99m. This is the dominant factor in determining the overall system resolution, since the intrinsic spatial resolution is in the range of 3 to 4 mm. One very important property to remember about collimators is that the spatial resolution gets worse as the source-to-collimator distance increases. This is illustrated in the set of phantom images that were acquired from 5 to 30 cm from the collimator surface. To obtain the best-quality images, spatial resolution comes at the price of count sensitivity; therefore it is crucial to keep the collimator as close to the patient as possible. The modern scintillation camera has improved performance because of improvements in the components and electronics. The availability of digital electronics has allowed the elimination of the Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.8 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION FIGURE 27.6 Collimation. The collimator is the image-forming aperture of the scintillation camera. It projects an image of the radionuclide distribution onto the NaI(Tl) crystal by brute force absorption of all gamma rays except those whose trajectory takes them through the holes. The collimator is also the limiting factor of both spatial resolution and count sensitivity. The spatial resolution significantly degrades with source-to-collimator distance. light pipe, which improves both energy and spatial resolution. However, this requires additional corrections because of the nonlinear response of the PMT array to the scintillations. If a collimated point source were focused on a portion of the NaI(Tl) crystal located exactly on a photomultiplier tube center, the energy spectrum would be distinctly different than one that was acquired from a point between two tubes (Fig. 27.7). This difference reflects the efficiency for collecting all the TABLE 27.2 Collimator Specifications Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.9 scintillation light. When the source is located directly on a photomultiplier tube, more of the scintillation is sampled by the photomultiplier tubes, and the pulses are therefore somewhat larger on the average than at other points. This position-dependent shift in the energy spectrum causes an overall loss in energy resolution. It also means that portions of the crystal will be accepting proportionately more scattered radiation. The solution to this problem is to locally sample the energy spectra and regionally adjust the energy window for each area. Typically the camera field of view is divided into a 64 ◊ 64 matrix and energy window adjustments are made for each of the 4096 regions. FIGURE 27.7 Energy correction. Because of the spatial arrangement of the PMTs, the magnitude of the energy signal varies with location, degrading the overall energy resolution. This problem is overcome by setting multiple local energy windows across the field of view. This energy correction does not improve uniformity, but it does remove the dependence of the scintillation camera on scatter conditions. Figure 27.7 shows the effect of energy correction when the scintillation camera is exposed to a uniform flux of gamma rays. First, it should be noted that both the corrected and uncorrected images are highly nonuniform and are not adequate for imaging. The energy correction simply makes sure that each region of the crystal is contributing valid photopeak events to the image. This results in only a subtle improvement in uniformity at this stage. However, it makes the subsequent corrections more robust, since there will be much less dependence on the effects of scattered radiation, which can vary over a large range, depending on the imaging situation. Because of the nonlinear response of the photomultiplier tubes, detected events are not correctly positioned using Anger logic alone. This mispositioning of events has a profound effect on field uniformity. 8 The parameter that quantifies how well-detected events are positioned is called spatial linearity. The optimization of spatial linearity requires the acquisition of an image from a welldefined distribution (Fig. 27.8). Typically this is accomplished with a highly precise rectangular hole pattern that is placed directly on the NaI(Tl) crystal. A distant point source of radioactivity is used to project an image of the hole pattern onto the scintillation camera. The image of this pattern appears similar to the image on the left with distortions caused by the mispositioning of events. Because the actual and measured location of the holes is known, regional displacements to the x and y coordinates can be calculated for each hole. Displacements for regions in between holes that are not directly sampled are interpolated at a very high sampling frequency (1024 ◊ 1024). This information is stored and is available as a lookup table. This measurement is usually done by the vendor at the factory and may be repeated several times a year. When a valid event is detected, the initial x and y coordinates are modified by the appropriate displacements that are read from the lookup table. Using this approach, events can be accurately positioned to better than 0.5 mm. The improvement in spatial linearity has a profound effect on field uniformity. Both images show the response of the scintillation camera to a Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.10 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION uniform flux of gamma rays. With spatial linearity correction, the field becomes uniform to within ±10 percent of the mean image counts. This level of uniformity is adequate for most conventional imaging. FIGURE 27.8 Spatial linearity correction. Residual positioning errors are corrected by imaging a precision hole phantom. A correction factor table is generated with the appropriate x and y offsets to reposition events to their correct location. The application of spatial linearity correction has a profound effect on image uniformity. There are still some residual nonuniformities that exist in the scintillation camera even after energy and spatial linearity correction have been applied. These can be further reduced by applying uniformity correction (Fig. 27.9). Typically, a high count flood is acquired and a map of the nonuniformities is stored in a memory buffer. During acquisition, the number of valid events that is acquired is modulated by this map to ensure uniformity. With this additional correction, the field uniformity can be reduced to within ±3 percent of the mean image counts. It should be noted that field uniformity can be degraded by a number of factors, including the energy of the gamma ray. The most crucial factor for a system that is operating properly is the setting of the energy window. Figure 27.9 illustrates the dependence of uniformity with the energy window setting. Some scintillation cameras are more forgiving than others, but all show more nonuniformity when the energy window is displaced from the center of the photopeak.9 There is often a gamma ray energy dependence as well. Most scintillation cameras are optimized for the best performance for the 140-keV gamma rays of Tc-99m. In some systems, uniformity significantly degrades at other gamma ray energies. Photomultiplier tubes are relatively unstable components. Their performance changes as they age and is also sensitive to variations in temperature and humidity. In order for the energy, spatial linearity, and uniformity corrections to remain valid, there must be some way of maintaining the photomultiplier tubes at a constant operating point. Most scintillation camera systems have photomultiplier tube stabilization firmware that dynamically adjusts the photomultiplier tubes in response to a known reference signal. Some vendors use a constant-output light-emitting diode inside the electronics housing that flashes 10 times per second. The individual photomultiplier tube signals from these calibration flashes are sensed by electronics that can compare the measured output to the desired value, and then make appropriate adjustments to maintain the operating point. Another approach uses the ratio between the count rates in a photopeak and scatter window to maintain constant photomultiplier tube response. Photomultiplier tubes are also very sensitive to magnetic Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.11 FIGURE 27.9 Uniformity correction. Nonuniformities in the field that remain after spatial linearity correction are corrected from the acquisition of a high count reference flood image. In many cameras, the field uniformity degrades when the energy window is not centered on the photopeak. fields, and changes in the orientation of the camera with respect to the earthís magnetic field are enough to cause measurable changes in field uniformity.10 To reduce this effect, each photomultiplier tube is individually surrounded with mu-metal shielding. The emission of gamma rays from a radioactive source has an exponential distribution. This means that for any particular event rate, short intervals between events occur much more often than long intervals. Because the scintillation light persists for a finite time, there will eventually be light emitted from more than one event as the count rate increases. In a scintillation camera, pulse pileup becomes evident at count rates as low as 20,000 counts per second (cps), and it gets increasingly worse as the count rate increases. Since information about pulse height becomes compromised, the performance of the scintillation camera degrades at high count rates. In most conventional and SPECT imaging, the count rate is low enough that pulse pileup is not a major concern. However, high count rates are encountered in some first-pass studies, and it is the primary problem in coincidence imaging. Corrections can be made for pulse pileup, since the physics of scintillations is well known (Fig. 27.10). Pileup can be detected on the basis of pulse height analysis. If the pileup is the result of only two events, the contribution to the second pulse from the first can be accurately estimated and subtracted, thus preserving both events. Multiple pileups can be identified and discarded. The count rate performance of scintillation cameras has improved dramatically in recent years because of the demands of coincidence imaging. When a conventional scintillation camera is recording count data at 120,000 cps, it is losing about 20 percent of the valid events. This loss increases with increasing count rate. In addition to the loss of sensitivity, both uniformity and spatial resolution get progressively worse as the count rate increases. Finally, it should be recognized that Anger logic will produce artifacts at very high count rates. ìVirtualî sources will appear midway between real sources because of the signal averaging.11 This problem has been addressed in coincidence systems by using maximum likelihood estimation instead of the conventional Anger logic. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.12 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION FIGURE 27.10 Pulse pileup. The persistence of the scintillation causes pulse pileup when the event rate exceeds 50,000 counts/s. Techniques can be applied to recover some of the lost information. This is especially important for coincidence imaging. Note also that the Anger positioning algorithm causes ìghostî images when the count rate becomes high. The performance of scintillation cameras is often specified in terms of the spatial resolution. Spatial resolution is a measure of image blur and it is often specified by the width of the pointspread function. On a perfect imaging system, the image of a point has no dispersion so that all the counts fall at the same point. On a real imaging system the point is blurred and a count profile through it has a gaussian shape. The width of this count profile at the half-maximum level (FWHM) is a commonly used method for specifying the spatial resolution. The imaging system will more or less blur every point in a similar way, leading to a loss of contrast. There are two spatial resolution parameters that are of interest with scintillation cameras. The intrinsic spatial resolution describes how precisely the event location is determined when a gamma ray interacts with the crystal. The extrinsic or system spatial resolution combines the effect of the collimation with the intrinsic resolution. The intrinsic spatial resolution varies from about 3 mm FWHM on systems with thin crystals and 2-in PMTs to about 4.5 mm on systems with thicker crystals and 3-in PMTs. The system spatial resolution depends on a variety of factors including the gamma ray energy, collimation, the source to collimator distance, and the intrinsic spatial resolution. Higher-energy gamma rays require thicker septal walls, which limits the resolving power of the collimator. As indicated above, there is a strong dependence on the distance that the source is from the collimator. The collimator and intrinsic resolution combine in quadrature like the sides of a right-angle triangle to yield the system resolution. The collimator resolution is generally more than 50 percent larger than the intrinsic resolution and therefore is the dominant factor. The system resolution at 10 cm ranges from 6.5 mm for an ultrahigh-resolution collimator to about 9.5 mm for a general-purpose collimator. It should be noted that there is nearly a factor of 3 loss of count sensitivity with the ultrahigh-resolution collimator compared to the general-purpose collimator. Scintillation cameras have the capability of simultaneously imaging different-energy gamma rays. Most scintillation cameras handle at least three and many can handle six or more energy windows. It is important that there is no significant distortion of the images obtained at the different energies. The parameter that monitors the correspondence between images acquired at different energies is referred Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.13 to as multiwindow spatial registration. The multiwindow spatial registration should be less than 3 mm on a modern scintillation system. In the future there will be further improvements in scintillation camera technology. 12 These include photomultiplier tube replacements, new scintillators, and solid-state alternatives. Photomultiplier tubes are expensive, bulky, and susceptible to drifting. Avalanche photodiodes are a possible replacement for photomultiplier tubes (Fig. 27.11). The photodiodes use solid-state components that are very compact and rugged. Photomultiplier tubes still have superior performance specifications and are better matched for NaI(Tl). But considerable progress has been made with the photodiode approach and special-purpose devices that use this technology are beginning to appear. Figure 27.11 shows a schematic for a miniature camera module that uses avalanche photodiodes. The scintillator used in this application is CsI(Tl). The scintillation light emitted for CsI(Tl) is better matched to the properties of the photodiode. Because of the compactness offered by such designs, scintillation cameras can be designed in novel ways for specific applications. One potential application is breast cancer imaging, where several of these devices could be arranged around the breast to collect SPECT data more efficiently than bulky conventional scintillation cameras. Solid-state detectors directly convert the absorbed gamma ray energy into collection of electric charge and do not need photomultiplier tubes. Since the PMT is a bulky and expensive component, this represents a significant breakthrough. Cadmium zinc telluride is an attractive solid-state detector13 (Fig. 27.12). It can be manufactured in a pixelated array and has comparable gamma ray detection FIGURE 27.11 PMT replacements. PMTs are an expensive and bulky component of the scintillation camera. Future designs may incorporate avalanche photodiodes. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.14 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION FIGURE 27.12 Solid state imagers. Although NaI(Tl)-based scintillation cameras will be the choice for the near future, improvements in solid-state detectors such as CdZnTe may lead to competitive imaging systems. efficiency to NaI(Tl) at 140 keV. Another advantage is that the energy resolution with CdZnTe is nearly a factor of 2 better than that of NaI(Tl). However, several production problems need to be solved before CdZnTe becomes a viable replacement for NaI(Tl). 27.3 SPECT SYSTEMS Single-photon-emission computed tomography (SPECT) produces tomographic images of the internal distribution of radiopharmaceuticals. 14,15 It is most commonly used in the diagnosis of coronary artery disease and in tumor detection. Projection images collected by one or more scintillation cameras are mathematically reconstructed to obtain the tomographic slices. Most clinical SPECT studies are qualitative with simplistic corrections for attenuation and scattered radiation. Quantitative SPECT requires corrections for attenuation, scatter, and spatial resolution, although these have not been routinely implemented in the past because of their computational load. SPECT instrumentation has evolved to include coincidence imaging of positron-emitting radiopharmaceuticals, specifically 18 F fluorodeoxyglucose. A SPECT system consists of one or more scintillation cameras mounted to a gantry that can revolve about a fixed horizontal axis (the axis of rotation) 16ñ19 (Fig. 27.13). SPECT studies are usually acquired over a full 360∞ arc, although myocardial perfusion studies typically use only data from the 180∞ arc that minimizes tissue attenuation. SPECT acquisitions are performed with the scintillation camera located at preselected angular locations (step-and-shoot mode), or in a continuous rotation mode. In the step-and-shoot mode, the detector rotates to each angular position and collects data in a preselected frame duration while the detector is motionless. In the continuousrotation mode, the study duration is selected and the rotation speed is adjusted to complete the orbit during this time. Projections are collected as the detector rotates and are binned into 60 to 120 frames over 360∞. It is crucial to maintain close proximity to the body as the detector rotates about the patient to achieve the best possible spatial resolution. Although a number of different approaches have been used to accomplish this, the most common method moves the detectors radially in and out as a function of rotation angle. Myocardial perfusion studies are the most commonly performed SPECT procedures. Because the heart is located in the left anterior portion of the thorax, gamma rays originating in the heart are highly attenuated for views collected from the right lateral and right posterior portions of the arc. For this reason, SPECT studies of the heart are usually collected using the 180∞ arc that extends from the left posterior oblique to the right anterior oblique view.20 This results in reconstructed images with the best contrast, although distortions are often somewhat more pronounced than when 360∞ data are used.21 Because of the widespread use of myocardial perfusion imaging, many SPECT systems have been optimized for 180∞ acquisition by using two detectors Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.15 FIGURE 27.13 SPECT acquisition. One or more scintillation cameras collect images at typically 60 to 120 angles around a 360∞ orbit. The scintillation camera acquires projection images from a large volume simultaneously. arranged at ~90∞ (Fig. 27.14). This reduces the acquisition time by a factor of 2 over single detectors and is approximately 30 percent more efficient than triple detector SPECT systems. Positioning the detectors at 90∞ poses some challenges for maintaining close proximity. Most systems rely on the motion of both the detectors and the SPECT table to accomplish this. The heart is continually moving during the SPECT acquisition, and this further compromises spatial resolution. Because the heart beats many times per minute, it is impossible to directly acquire FIGURE 27.14 SPECT system configurations. Although a single scintillation camera can be used to acquire SPECT data, multiple detectors improve the overall sensitivity. Two detectors arranged at either 180 or 90∞ are the most common configuration. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.16 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION a stop-action SPECT study. However, since the heart motion is periodic, it is possible to obtain this information by gating the SPECT acquisition. 22 In a gated SPECT acquisition, the cardiac cycle is subdivided and a set of eight images spanning the ECG R-R interval is acquired for each angular view. These images are acquired into predetermined time bins based on the patientís heart rate, which is monitored by the ECG R wave interfaced to the SPECT system. As added benefits of gating, the motion of the heart walls can be observed and ventricular volumes and ejection fractions can be determined. 22,23 Although most SPECT imaging samples more or less static distribution of radionuclides, some SPECT systems can perform rapid sequential studies to monitor tracer clearance. An example of this is determination of regional cerebral blood from the clearance of 133 Xe.24 Multiple 1-minute SPECT studies are acquired over a 10-minute interval. When one acquisition sample is completed, the next begins automatically. In order to minimize time, SPECT systems that perform these studies can alternately reverse the acquisition direction, although at least one SPECT system utilizes slipring technology so that the detectors can rotate continuously in the same direction. In order to produce accurate tomographic images, projection data representing the line integrals of activity in the internal distribution have to be acquired. This information is not directly available because of tissue attenuation. Simple attenuation correction methods can be used in regions of the body such as the abdomen or head where the tissue density is more or less uniform. However, compensation for attenuation in the thorax requires an accurate attenuation map for each tomographic plane. This is especially important for myocardial perfusion studies, since the artifacts resulting from tissue attenuation mimic the patterns caused by coronary artery disease. In recent years, all the SPECT manufacturers have offered systems that can perform transmission measurements along with the emission studies. These systems use the scintillation camera to detect the transmission of gamma rays from an external source.17,25,26 Several different configurations are available. Most use a line source that is translated across the camera field of view at each angular stop in much the same way as a first-generation CT scanner (Fig. 27.15). Typically a source such as Gd-153 or Ba-133 is FIGURE 27.15 Attenuation correction. To obtain accurate SPECT results, corrections must be made for tissue attenuation. In regions where there are large variations in tissue density such as the thorax, this requires an independent transmission study. This shows one possible configuration where line sources of Gd-153 are translated across the field of view to collect the transmission data. This information is reconstructed to obtain a crude CT image of the thorax to correct myocardial perfusion studies. (Courtesy of GE Medical Systems.) Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.17 used that has a different gamma ray energy than those used in the emission study so that the studies can be acquired simultaneously (with appropriate correction for cross talk). Other approaches use multiple stationary line sources to collect this information. At least one vendor has an x-ray tube and separate detectors to obtain a moderate-quality CT scan.27 In each configuration, the transmission data are collected and reconstructed to yield the attenuation maps. This information can be incorporated into an iterative algorithm to effect the correction. In spite of the energy discrimination available on all SPECT systems, Compton scattered radiation still accounts for about 30 to 40 percent of the acquired counts in SPECT imaging. Scattered radiation decreases contrast and can impact other corrections. For example, when attenuation correction is applied without also correcting for scattered radiation, the count density in the heart walls near the liver may be overenhanced. SPECT systems in the future may resort to other detectors that have substantially better energy resolution than that of NaI(Tl), but for now, scatter compensation routines must be employed. Scatter correction has been performed in several different ways.15,28ñ33 The easiest to implement is the subtraction method, where information is simultaneously acquired into a second energy window centered below the photopeak in the Compton scatter region of the energy spectrum. After establishing an appropriate normalization factor, the counts from the scatter window are subtracted from the photopeak window. The corrected projections are then used in the reconstruction algorithm. The disadvantage of this approach is that it increases noise and it is difficult to establish an accurate normalization factor. To accommodate this type of correction (and also to image differentenergy gamma rays), SPECT systems allow the simultaneous acquisition from multiple energy windows. The number of energy windows available varies for each manufacturer, although every system is capable of imaging from at least four energy windows. 27.3.1 SPECT Image Reconstruction The details of SPECT image reconstruction are beyond the scope of this article. However, the demands of image reconstruction do impact the features required by the computer. The CPU must be fast enough and have enough memory to accommodate the entire SPECT data set. This is well within the capability of home PCs. A typical SPECT study is less than 5 Mbyte and the current processor speeds approaching 1 GHz are fast enough to render reconstructions using either filter backprojection or optimized iterative algorithms in an acceptable time (less than 10 minutes). 27.3.2 SPECT System Performance Typical performance specifications for SPECT imaging systems are summarized in Table 27.3. As with conventional planar imaging, the scintillation cameras, and the associated collimation are the primary factors affecting the performance. SPECT spatial resolution is nearly isotropic with an FWHM of 8 to 10 mm for brain imaging where the detectors can get close to the radioactive source. TABLE 27.3 SPECT System Performance Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.18 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION The spatial resolution degrades to 12 to 18 mm for body imaging because the detectors can not be positioned as close. The components of SPECT spatial resolution and their relative importance can be identified from the equation shown below: As before, R int and R col represent the intrinsic and collimator resolution components. R filter is the FWHM of the smoothing kernel required to yield an acceptable reconstruction. The intrinsic spatial resolution is the least important factor in this calculation, since it is usually a factor of 2 or more smaller than the other components. The trade-off between spatial resolution and count sensitivity is explicit in this equation. Decreasing R col to improve spatial resolution will often require R filter to become larger to compensate for increased noise. 27.3.3 SPECT/PET Hybrid Systems The primary reason for the success of nuclear medicine imaging is the availability of radiopharmaceuticals that provide crucial diagnostic information. For cancer diagnosis and followup, 18 F flourodeoxyglucose ( 18F FDG) is an exquisite imaging agent for a wide variety of malignancies including lung, colon, breast, melanoma, and lymphoma. Because 18F is a positron emitter that yields very high energy x-rays (511 keV) when the positron combines with a free electron, it can not be imaged well on conventional SPECT systems. The thin NaI(Tl) crystals have a low efficiency for detection at this energy (less than 10 percent). Also, the collimators designed for the 511-keV photons have low count sensitivity and poor spatial resolution. The collimation can be eliminated if coincidence detection is used. Annihilation photons from positrons are always colinear. This feature can be exploited to count only events that are simultaneously detected by opposed detectors. Two opposed scintillation cameras with their collimators removed and the addition of coincidence electronics will turn a SPECT system into a PET tomograph (Fig. 27.16).34,35 The efficiency for coincidence detection equals the product of the individual efficiencies, so that the coincidence efficiency is about 1 percent for conventional scintillation cameras. This is actually much higher than the efficiency with collimators. Coincidence efficiency can be improved by using thicker NaI(Tl) crystals, and all the vendors have done this. However, thicker crystals degrade the intrinsic spatial resolution when the scintillation FIGURE 27.16 Two or more opposed scintillation cameras can be used as coincidence detection systems for PET imaging. Valid events are established when the two detectors record events within the 10- to 15-ns timing window. Graded filters and lead septa are placed in front of the detectors to limit scattered radiation. (Courtesy of GE Medical Systems.) Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.19 cameras are used for conventional (i.e., collimated) studies. A solution to this problem, called StarBrite, has been recently introduced. Thick NaI(Tl) crystals (25 mm) have slots machined in the PMT side of the detector to prevent the scintillation light from scattering throughout the crystal to maintain good spatial resolution. There are other concerns, primarily the count rate capability. With most SPECT imaging studies, there are essentially no count rate losses resulting from the time it takes to process each event. The amount of radioactivity that can be safely administered and the low sensitivity of the collimation keep the count rate in the range that the electronics can easily handle. However, when the collimators are removed for coincidence imaging, the NaI(Tl) crystals are exposed to count rates above the capacity of the conventional electronics. Much effort over the past decade has been devoted to increasing the count rate capability of the scintillation cameras. In the early 1990s, the maximum observed counting rate for a scintillation camera was in the 200,000 to 400,000 count/second range. This rate has been extended to over 1,000,000 counts/second by shortening the integration time on the pulses and implementing active baseline restoration. Because the light is proportional to the energy deposited in the crystal, one can shorten the pulse integration time without extreme degradation. Even with this substantial improvement in count rate, the maximum activity the system can handle is about 3 mCi. Typical performance values for a coincidence scintillation camera system are given in Table 27.4. TABLE 27.4 SPECT/PET Hybrid System Performance In addition to specialized electronics, other measures have been taken to help reduce the count rate burden. One example of these is a graded absorber placed in front of each detector to help reduce the scattered radiation component. 36 Because scattered radiation has lower energy than the unscattered photons, low-energy scatter will be preferentially absorbed by lead, since the photoelectric cross section is inversely proportional to the cube of the gamma ray energy. If only lead is used, the lead characteristic x-ray resulting from the absorption will be detected. Additional layers of tin, copper, and aluminum will absorb the respective characteristic x-rays. This graded filter causes a significant reduction in the low-energy scattered radiation and, since the scintillation cameras process every event, also reduces the overall count rate burden. Even though the thin NaI(Tl) crystals have low intrinsic efficiency, the uncollimated detectors present a large solid angle to the annihilation photons. Maximum sensitivity is achieved when all coincidences, even those at large angles, are accepted. This makes the camera sensitivity extremely sensitive to the source location. Sources located near the central axis of the detectors have a large solid angle, while those at the periphery can interact only with a very small portion of the detectors. In addition, the scatter component increases to well over 50 percent when large coincidence acceptance angles are used. This problem has been addressed by using lead slits aligned perpendicular to the axial direction of the system to restrict the angular extent of the coincidences. While this reduces the sensitivity of the imaging system, it also reduces the scatter component to less than 30 percent and limits the solid angle variability. The intrinsic spatial resolution of the hybrid systems is comparable to that of the dedicated PET systems with a FWHM of 4 to 5 mm. However, the count sensitivity is at least an order of magnitude lower. This, along with the maximum count rate constraint, guarantees that the coincidence camera data will be very count poor and therefore require substantial low-pass filtering when reconstructed. As a result the quality of the reconstructed images is perceptibly worse than the dedicated PET images. In head-to-head comparisons, it has been found that the hybrid systems perform well on Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.20 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION tumors greater than 2 cm in diameter located in the lung.37ñ39 Tumors smaller than these and those located in high-background areas are detected with a much lower sensitivity. These results are important since they provide a guide where the application of the coincidence camera will be useful. In a conventional scintillation camera, Anger logic is used to determine the location of an interaction. The tacit assumption in this approach is that only one event is occurring at a time. At the high count rate encountered in coincidence imaging, multiple interactions are likely, and when this occurs, the events are improperly located somewhere between the two true locations. Improved algorithms have been developed that can identify multiple hits and that use a maximum likelihood calculation to correctly determine event locations. The projection data collected by the coincidence cameras require correction for random coincidences, scatter, and attenuation if accurate tomographic images are to be obtained. Random or accidental coincidences occur when two unrelated photons are detected. These random coincidences increase rapidly with the count rate and give rise to a nondescript background that has to be subtracted from the projections. Typically randoms are either monitored in a separate time window or are calculated from the singles count rate and are subtracted. Scatter correction is sometimes ignored in coincidence PET, or maybe monitored by a separate energy window and subtracted as discussed for SPECT imaging. Accurate reconstruction of PET data requires correction for attenuation since the degree of attenuation for coincidence imaging is very high, approaching values of 100 or more. Attenuation correction requires information about the transmission of the annihilation radiation through the body at the coincidence lines of response. When attenuation correction is ignored, severe artifacts are seen in the reconstructed images. As with SPECT imaging, a separate transmission study with an external source, typically Cs-137, must be acquired to provide the attenuation map used in the correction. 27.4 SUMMARY SPECT imaging is expected to play a continuing important role in medical imaging. Future improvements in SPECT instrumentation are likely to include new detectors and collimation schemes. The coincidence scintillation cameras will also continue their evolution with the addition of more cameras and multidetector levels optimized for SPECT and coincidence imaging. Reconstruction algorithms will evolve as new techniques are developed and as the performance of the computer expands. In spite of the importance of instrumentation, the primary motivating factor in SPECT imaging will continue to be the creation and implementation of new radiopharmaceuticals. While SPECT will continue to be highly utilized for myocardial perfusion imaging, SPECT use in tumor imaging will probably experience the largest growth. Applications will include treatment planning for internal radiation therapy as well as diagnostic studies. REFERENCES 1. Hubbell J. H., ìReview of photon interaction cross section data in the medical and biological context,î Phys. Med. Biol., 1999; 44:R1ñR22. 2. Graham L. S., et al., ìNuclear medicine from Becquerel to the present,î Radiographics, 1989; 9:1189ñ1202. 3. Anger H. O., et al., ìRecent applications of the scintillation camera,î Strahlentherapie [Sonderb] 1967; 65:70ñ93. 4. White W., ìResolution, sensitivity, and contrast in gamma-camera design: A critical review,î Radiology, 1979; 132:179ñ187. 5. Genna S., S. C. Pang, and A. Smith, ìDigital scintigraphy: Principles, design, and performance,î J. Nucl. Med., 1981; 22:365ñ371. 6. Gunter D., Collimator Characteristics and Design, 1st ed., Nuclear Medicine, R. Henkin, et al., (eds.), vol. 1., 1996, Mosby, St. Louis, pp. 96ñ124. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.21 7. Moore S. C., K. Kouris, and I. Cullum, ìCollimator design for single photon emission tomography,î European Journal of Nuclear Medicine, 1992; 19:138ñ150. 8. Muehllehner G., J. G. Colsher, and E. W. Stoub, ìCorrection for field nonuniformity in scintillation cameras through removal of spastial distortion,î J. Nucl. Med., 1980; 21:771ñ776. 9. Graham L. S., R. L. LaFontaine, and M. A. Stein, ìEffects of asymmetric photopeak windows on flood field uniformity and spatial resolution of scintillation cameras,î J. Nucl. Med., 1986; 27:706ñ713. 10. Bieszk J. A., ìPerformance changes of an Anger camera in magnetic fields up to 10 G,î J. Nucl. Med., 1986; 27:1902ñ1907. 11. Strand S. E., and I. Larsson, ìImage artifacts at high photon fluence rates in single-crystal NaI(Tl) scintillation cameras,î J. Nucl. Med., 1978; 19:407ñ413. 12. Kuikka J. T., et al., ìFuture developments in nuclear medicine instrumentation: A review,î Nucl. Med. Commun., 1998; 19:3ñ 12. 13. Yaffe, M. J., and J. A. Rowlands, ìX-ray detectors for digital radiography,î Phys. Med. Biol., 1997; 42: 1ñ39. 14. Madsen M. T., ìThe AAPM/RSNA physics tutorial for residents. Introduction to emission CT,î Radiographics, 1995; 15:975ñ991. 15. Tsui B. M., et al., ìQuantitative single-photon emission computed tomography: Basics and clinical considerations,î Semin. Nucl. Med., 1994; 24:38ñ65. 16. Jaszczak R. J., and R. E. Coleman, ìSingle photon emission computed tomography (SPECT). Principles and instrumentation,î Invest. Radiol., 1985; 20:897ñ910. 17. Fahey F. H., ìState of the art in emission tomography equipment,î Radiographics, 1996; 16:409ñ420. 18. Links J. M., ìAdvances in nuclear medicine instrumentation: Considerations in the design and selection of an imaging system,î Eur. J. Nucl. Med., 1998; 25:1453ñ1466. 19. Rogers W. L., and R. J. Ackermann, ìSPECT instrumentation,î Am. J. Physiol. Imaging, 1992; 7:105ñ120. 20. Tsui B. M., et al., ìQuantitative myocardial perfusion SPECT,î J. Nucl. Cardiol, 1998; 5:507ñ522. 21. LaCroix K. J., B. M. Tsui, and B. H. Hasegawa, ìA comparison of 180 degrees and 360 degrees acquisition for attenuationcompensated thallium-201 SPECT images,î J. Nucl. Med., 1998; 39:562ñ574. 22. White M. P., A. Mann, and M. A. Saari, ìGated SPECT imaging 101,î J. Nucl. Card., 1998; 5:523ñ526. 23. Berman D. S., and G. Germano, ìEvaluation of ventricular ejection fraction, wall motion, wall thickening, and other parameters with gated myocardial perfusion single-photon emission computed tomography,î J. Nucl. Card., 1997; 4:S169ñS171. 24. Bruyant P., et al., ìRegional cerebral blood flow determination using 133Xe and a standard rotating gamma-camera,î Comput. Biol. Med., 1998; 28:27ñ45. 25. King M. A., B. M. Tsui, and T. S. Pan, ìAttenuation compensation for cardiac single-photon emission computed tomographic imaging: Part 1. Impact of attenuation and methods of estimating attenuation maps,î J. Nucl. Cardiol., 1995; 2:513ñ524. 26. Celler A., et al., ìMultiple line source array for SPECT transmission scans: Simulation, phantom and patient studies,î J. Nucl. Med., 1998; 39:2183ñ2189. 27. Patton J. A., ìInstrumentation for coincidence imaging with multihead scintillation cameras,î Semin. Nucl. Med., October 2000, 30:239ñ254. 28. Buvat I., et al., ìComparative assessment of nine scatter correction methods based on spectral analysis using Monte Carlo simulations,î J. Nucl. Med., 1995; 36:1476ñ1488. 29. Beekman F. J., C. Kamphuis, and E. C. Frey, ìScatter compensation methods in 3D iterative SPECT reconstruction: A simulation study,î Phys. Med. Biol., 1997; 42:1619ñ1632. 30. Beekman F. J., H. W. de Jong, and E. T. Slijpen, ìEfficient SPECT scatter calculation in non-uniform media using correlated Monte Carlo simulation,î Phys. Med. Biol., 1999; 44:N183ñN192. 31. Riauka T. A., and Z. W. Gortel, ìPhoton propagation and detection in single-photon emission computed tomography ó A n analytical approach,î Medical Physics, 1994; 21:1311ñ1321. 32. Haynor D. R., et al., ìMultiwindow scatter correction techniques in single-photon imaging,î Medical Physics, 1995; 22:2015ñ2024. 33. Rosenthal M. S., et al., ìQuantitative SPECT imaging: A review and recommendations by the Focus Committee of the Society of Nuclear Medicine Computer and Instrumentation Council,î J. Nucl. Med., 1995; 36:1489ñ1513. 34. Jarritt P. H., and P. D. Acton, ìPET imaging using gamma camera systems: A review,î Nucl. Med. Commun., 1996; 17:758ñ766. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website. NUCLEAR MEDICINE IMAGING INSTRUMENTATION 27.22 DESIGN OF MEDICAL DEVICES AND DIAGNOSTIC INSTRUMENTATION 35. Lewellen T. K., R. S. Miyaoka, and W. L. Swan, ìPET imaging using dual-headed gamma cameras: an update,î Nucl. Med. Commun., 1999; 20:5ñ12. 36. Muehllehner G., R. J. Jaszczak, and R. N. Beck, ìThe reduction of coincidence loss in radionuclide imaging cameras through the use of composite filters,î Phys. Med. Biol., 1974; 19:504ñ510. 37. Shreve P. D., et al., ìOncologic diagnosis with 2-[fluorine-18]fluoro-2-deoxy-D-glucose imaging: Dual-head coincidence gamma camera versus positron emission tomographic scanner,î Radiology, 1998; 207:431ñ437. 38. Shreve P. D., R. S. Steventon, and M. D. Gross, ìDiagnosis of spine metastases by FDG imaging using a gamma camera in the coincidence mode,î Clin. Nucl. Med., 1998; 23:799ñ802. 39. Coleman R. E., C. M. Laymon, and T. G. Turkington, ìFDG imaging of lung nodules: A phantom study comparing SPECT, camera-based PET, and dedicated PET,î Radiology, 1999; 210:823ñ828. Downloaded from Digital Engineering Library @ McGraw-Hill (www.digitalengineeringlibrary.com) Copyright © 2004 The McGraw-Hill Companies. All rights reserved. Any use is subject to the Terms of Use as given at the website.