Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
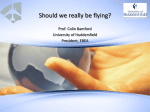
Comorbid Personality Disorders and Substance Use Disorders of Mentally 111 Homicide Offenders: A Structured Clinical Study on Dual and Triple Diagnoses by Anu Putkonen, Irma Kotilainen, Christian C. Joyed, and Jari Tiihonen Several studies have demonstrated that persons suffering from MMD are at increased risk for community violence, other violent offenses, and homicide, particularly if they have coexisting alcoholism or SUD (Swanson et al. 1990; Eronen et al. 1996i>; Hodgins et al. 1996a; Tiihonen et al. 1996; RSsfinen et al. 1998; Brennan et al. 2000). Moran et al. (2003) were die first to demonstrate the independent association between premorbid ICD-10 PD and number of physical assaults during a 2-year followup among community-dwelling patients with psychotic disorders (UK700 study data, n = 670). However, the authors could not examine whether comorbid PD increased the risk of serious assaults in psychosis, because neither the seriousness nor the frequency of assaults was recorded. The literature provides no direct evidence of an association between comorbid personality disorders and severe violence among psychotic individuals. Data from high- and low-risk subgroups are important, as SUDs are common among persons with MMD (47% lifetime prevalence in the United States), compared to the general population (13.2%, Regier et al. 1990), while only a few of the dually diagnosed (MMD + SUD) persons commit homicide (Eronen et al. 1996fc). Among nonpsychotic persons, antisocial personality disorder (APD) has a strong association with homicide (Eronen et al. 1996a). Comorbidity of APD with other psychiatric disorders is common; in the Epidemiological Catchment Area (ECA) study, as much as 84 percent of U.S. individuals with APD also had alcohol use disorder, and a powerful association between active APD and schizophrenia and mania was reported (Regier et al. 1990). The lifetime prevalence of APD in the U.S. general population was estimated to be 4.5 percent among males and 0.8 percent among females. Because nonpsychotic individuals with APD are characterized by poor compliance with medical treatments, including medication Abstract Comorbid substance use disorders (SUDs) increase the risk of homicide by persons with major mental disorders (MMDs). However, there are no published data from clinical interviews or lifetime objective documents on the prevalence of lifetime personality disorder (PD) or SUD among a comprehensive sample of mentally ill homicide offenders. Therefore, a nationally representative sample of men with MMD (n = 90) who had committed or attempted homicide was assessed using the research version of the Structured Clinical Interview for DSM-IV Axis I and Axis II Disorders. Lifetime documents, records, and questionnaires from persons who knew the subjects since childhood were used. Seventy-eight percent of the mentally ill homicide offenders were diagnosed with schizophrenia, 17 percent with schizoaffective disorder, and 5 percent with other psychosis. A lifetime SUD was detected in 74 percent and alcohol use disorder in 72 percent PD accounted for 51 percent, in 47 percent as antisocial personality disorder (APD). All subjects diagnosed with PD had SUD. Only 25 percent of the subjects had neither SUD nor PD. Among persons with dual diagnoses (MMD and SUD), about two-thirds had PD or APD. These results indicated that there were two-thirds major diagnostic categories of psychotic homicide offenders: about one-half had triple diagnosis (APD + SUD + MMD), one-quarter had "pure" dual diagnosis (SUD + MMD), and one-quarter had "pure" MMD. The fourth possible category, "APD + MMD but no SUD," was not found. The prevention of severe violence by persons with MMD necessitates effective treatments for those with dual diagnosis who also have a history of APD. Keywords: Major mental disorders, schizophrenia, antisocial personality disorder, substance abuse, homicide, violence. Schizophrenia Bulletin, 30(l):59-72,2004. Send reprint requests to Dr. A. Putkonen, Department of Forensic Psychiatry, University of Kuopio, Niuvanniemi Hospital, FIN-70240 Kuopio, Finland; e-mail: [email protected]. 59 Schizophrenia Bulletin, Vol. 30, No. 1, 2004 A. Putkonen et al. (Black et al. 1988), psychotherapy (Woody et al. 1985), and integrated substance abuse and psychiatric treatment programs for dually diagnosed patients (Robins et al. 1991), the same may apply to persons with MMD and a history of APD. Thus, the role of APD could also be of great interest when early prevention of violent crimes and treatment of violent psychotic patients are considered. SUD Among Mentally 111 Homicide Offenders The studies on comprehensive samples of mentally ill homicide offenders (table 1; Lindqvist 1986; Gottlieb et al. 1987; Gabrielsen et al. 1992; Eronen 1995; Eronen et al. 1996fc; Erb et al. 2001) reported lower prevalence of alcoholism or SUD among homicide offenders with psychotic disorders (8-44%) than among nonpsychotic homicide offenders (61%, Gottlieb et al. 1987). The low prevalence of APD (8-14%) and SUD (8-44%) among nationally representative samples of male homicide offenders with MMD in the existing literature is not in accordance with the replicated findings that SUD is more common among persons with schizophrenia (47% lifetime prevalence in the United States), compared to the general population (13.2%; Regier et al. 1990), and that SUD is associated with increased risk for homicidal behavior among individuals with schizophrenia. However, these reports were made on the basis of file documents and without patient interviews. Such studies are likely to underrecord comorbid SUD and APD, because SUD is substantially underdiagnosed in psychiatric care settings (Drake and Mueser 2000; Hansen et al. 2000) and prisons (Abram and Teplin 1991) and PD is traditionally not determined or documented in patients who meet the criteria of MMD (Surtees and Kendell 1979). Later, the multiaxial system of DSM classification (APA 1994) made it more likely that clinicians would diagnose both lifetime MMD and PD within the same person. It is difficult to study clinically the association of APD, MMD, and homicide. The optimal study design, a prospective cohort study, should be very large to achieve sufficient statistical power because of the rarity of both homicides and MMD in the general population. Persons with APD tend to gather together, or to be selected, in populations or facilities with a very high prevalence of APD and SUD (Abram and Teplin 1991). Therefore, not even comparative data of lifetime APD among all persons with MMD in communities are available. In most Western countries, it is also impossible to obtain objective historical documents for individuals from large populations. Without such documents, childhood conduct disorder symptoms, which are needed for the DSM-IV diagnosis of APD, are underdiagnosed and the resulting prevalence remains low. In many Western countries, prison populations include homicide offenders with MMD (Taylor and Gunn 1984; C6t6 and Hodgins 1990). Therefore, the studies of representative high-security hospital populations or prison populations in such countries are not nationally representative samples of psychotic homicide offenders in these countries. Possibly the best available way would be a structured clinical study of a nationally representative APD Among Mentally 111 Homicide Offenders Results from the only study concerning the prevalence of comorbid APD among a nationally representative sample of mentally ill homicide offenders by Erb et al. (2001) indicated that only 8 percent of all male homicide offenders with schizophrenia in West Germany from 1955 to 1964 (n = 284), and 14 percent of male homicide offenders with schizophrenia in Hessen from 1992 to 1996 (n = 29), met the criteria of DSM-III for APD on the basis of hospital documents and crime registers (table 1). A smaller Canadian study compared homicide offenders and nonhomicide offenders who were incarcerated in Quebec penitentiaries (C6t6 and Hodgins 1992). Among 11 homicide offenders with schizophrenia in that study, 64 percent had APD and 73 percent had alcohol use disorder. Among 36 persons with affective disorders (2 with bipolar disorder, 5 with atypical bipolar disorder, and 29 with major depression), the prevalence of APD was 65 to 100 percent and of SUD 60 to 100 percent in each diagnostic group. However, the sample set did not include mentally ill homicide offenders who had been "not guilty of homicide by reason of insanity," and the number of offenders in each group was small (n - 2-29). PD Among Mentally 111 Homicide Offenders Two studies have reported the prevalence of mentally ill homicide offenders with any existing comorbid PD diagnosis in their examination reports for juridical court (Lindqvist 1986; Putkonen et al. 2001) and one study the prevalence of PD among a U.K. security hospital population (Taylor et al. 1998; table 1). Lindqvist found that 9 percent of mentally ill homicide offenders of both sexes (n = 34) in Northern Sweden from 1970 to 1981, and Putkonen et al. found that 32 percent of female homicide offenders with MMD in Finland (n = 34) were diagnosed with PD. Taylor et al. (1998) studied the records of the patients in three U.K. security hospitals and diagnosed 231 homicide offenders with ICD-10 psychosis and 78 having "psychosis with independent PD" (25%). 60 Schizophrenia homicide offenders and attempters in Hessen (1992-1996) 124 female homicide offenders examined for court in Finland 1980-1992 DSM-III-R diagnoses were made on the basis of forensic psychiatric examination reports, hospital records, crime registers, and yearly assessments for court. 29 (25 males + 4 females) with schizophrenia All schizophrenia homicide offenders and attempters in Federal Republic of Germany 1955-1964 Erbetal. (2001) Eronen(1995) DSM-III-R diagnoses were made on the basis of forensic psychiatric examination reports, hospital records, crime registers, and yearly assessments for court. 284 (232 males + 52 females) with schizophrenia All 1,740 patients resident in the 3 special hospitals in the United Kingdom during the first half of 1993 Taylor etal. (1998) 18 female schizophrenia patients 309 with psychosis gender distribution not specified 93 (86 males + 7 females) with schizophrenia 1,428 homicide offenders examined for court in Finland during 12 yrs (75% of all) Eronenet al. (1996ft) Diagnoses of forensic psychiatric examination reports were collected. ICD-10 diagnoses were made on the basis of hospital records. Criminal records were available on two-thirds of the sample. DShA-lll-R diagnoses were made on the basis of forensic psychiatric examination reports. Diagnoses of psychiatric examination reports were collected. Substance abuse2 of (A) psychotic and (B) nonpsychotic offenders. 58 with psychosis (42 males + 16 females), 16 of whom had schizophrenia 251 of 263 homicide offenders investigated for court in Copenhagen during 1959-1983 Diagnoses of forensic psychiatric examination reports were collected. Gottlieb etal. (1987) Gabrielsen et al. (1992) 34 with "mental disease, mainly males" Method All 64 homicide offenders (60 males + 4 females) in Northern Sweden during 1970-1981 Subjects of the study Undqvist(1986) Authors (yr) Number, gender, and diagnostic distribution of mentally III homicide offenders APD — — 25% — — 14% 8% — — — — 9% (6% + SUD) PD SUD 33% 1 38%,1 31 % 3 — Males 44%, 1 females 43% 1 males 40% females 12% A: 33%, 32% Prevalence of Table 1. The prevalence of PD, APD, and SUD In previous studies of mentally III persons with homicidal behavior, calculated on the basis of published data o © I I I a a Schizophrenia Bulletin, Vol. 30, No. 1, 2004 A. Putkonen et al. s sample of psychotic homicide offenders in a country where the clearing rate of homicides is high, all homicide offenders having psychiatric symptoms are examined, and objective lifetime documents are available. To date, there have been no such studies concerning the prevalence of comorbid APD and SUD among representative samples of homicide offenders with MMD. Because file-based studies may underestimate possible dual and triple diagnoses, die aim of the present study was to determine whether the prevalence of APD and SUD in a clinical interview study, verified with detailed documents, differs from that in document studies. I £ I I s a S o 1 CO "3 I 2 E o .5 O 05 a In Finland, MMD has, in practice, been considered such a severe disorder as to diminish the ability of an individual to control his or her violent behavior. Therefore, violent offenders are investigated by senior psychiatrists if any psychiatric symptoms have been detected in criminal investigations, hearings, documents, or examinations in prison by medical staff, or if the homicide offender or his or her lawyer asked for investigation. About 70 percent of all homicide offenders undergo a detailed forensic psychiatric examination that includes physical examinations, brain CT or fMRI study, EEG, laboratory tests, structured psychological tests, and usually structured diagnostic interviews (Eronen et al. 1996a) during a period of 4 to 8 weeks, usually in a psychiatric or forensic psychiatric hospital. Mentally ill homicide offenders and mose who attempted homicide are not convicted in juridical court. However, the forensic Psychiatric Board (of the Ministry of Social and Health Affairs) commits such individuals to one of two state psychiatric hospitals, on the basis of the examination report and collateral documents. This same board eventually permits their discharge. Only in very exceptional cases are homicide offenders with a pretrial MMD diagnosis incarcerated in prisons (Putkonen et al. 2001). The examination reports include data that are obtained by court order from physicians and hospitals, schools, social welfare offices, the military, prisons, and crime registers, in addition to questionnaires completed by parents, siblings, teachers, and employees. On 1 March 1998 there were 99 persons in the Niuvanniemi (psychiatric state) Hospital who were diagnosed as suffering from MMD during their homicidal act. Two of them were female. Ninety-three persons were willing to be interviewed between March and May of 1998. Three persons were excluded: one female and two males who did not obtain an MMD diagnosis. For the final analysis, 90 males were evaluated by the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I). The information was insufficient in two cases concerning the assessment of SUD. Five persons could Q W 8. £ IJO. •o Q S" Sc r- Methods •D ^C 1 m '«" £ 1a> 8 o I? C ® o ^ © is 1 sic psy rts a c o o linati | Ia 1 CO CO CD n? b b to •o •o I E o 2 % in I (0 •c a. ^ ® .E CD a £ "o a> ^ ^ ,_ = (0 £ ]o o c .n •o a. < l X fi O CD -g ^ S f - C CM (D E CD 1 (D £ I O ® Q) t CD $ CT> o ^ Ew 1 $ CD CD CO CD o o Q.-O O TJ . £ il CD E | CD J2 T3 E JS .a a. P o 62 Mentally 111 Homicide Offenders Schizophrenia Bulletin, Vol. 30, No. 1, 2004 not be assessed with the Structured Clinical Interview for DSM-IV Axis H Disorders (SCID-II) because of a lack of confirmed information on their behavior before the age of 15. One of them had already been excluded from the SUD assessment. All but two (both Asian males) were Caucasians. Of all the participants, 65 (72%) had committed one or more homicides and 25 (28%) had attempted to kill someone. The mean age of the participants was 43.6 years (range 21-73 years, standard deviation [SD] 11.5). The participants were committed to the hospital between 1948 and 1997 (mean 1989, SD 9.60), 35 of them (39%) during the last 3 years. The mean duration of treatment was 8.7 years (range 1-50 years, SD 9.60). DSM-IV Axis I and Axis II diagnoses were assessed with the SCID Research Version (First et al. 1996a, 1996£>) by two forensic psychiatrists. According to the SCID protocol, all available information was used. Information given by a participant during the interview was subsequently verified through other sources. Both medical and psychiatric data, and forensic psychiatric examination reports, were studied. Because of the limited ability of most patients to use the self-report personality questionnaire, we assessed all items as needed. The interviews lasted between 2 and 8 hours. To test the interrater reliability, 15 percent of the participants were studied by both of the interviewers. The concordance rates between the raters were 1.00 concerning MMD and PD, and 0.86 concerning SUD. Offenders with PD could have been discharged from the hospital at either a later or an earlier stage of treatment, when compared to those with pure psychotic disorders. Therefore, the PD data were also compared by the X2 test with those of the patients having a longer duration of treatment. The prevalence of PD and SUD between homicide offenders and homicide attempters was compared as well. The prevalence and comorbidity of PD, SUD, and MMD diagnoses were calculated for the entire sample and for the main MMD groups. The co-occurrence of PD and SUD for each MMD group was compared with that of other patients with the x 2 test- A p value lower than 0.05 was considered statistically significant. SPSS 8.0 for Windows was used for statistical analyses. and comorbidity of PD and SUD subtypes in the main MMD groups are shown in table 2. Seventy-eight percent of the male homicide offenders were diagnosed with schizophrenia, 17 percent with schizoaffective psychosis, and 5 percent with other psychoses. Fifty-one percent of the patients additionally received one or more lifetime PD diagnoses, including 47 percent with APD. Many patients fulfilled the criteria for several PDs (figure 2). An SUD diagnosis was obtained for 74 percent of the 88 offenders for whom SUD was assessed (figure 3). Seventy-two percent (n = 63) had alcohol abuse, and 64 percent (n - 56) had alcohol dependence. Other substance than alcohol abuse was diagnosed in 36 percent {n - 32) of the cases, and other substance dependence in 33 percent (n = 29). Thus, 89 percent of the alcohol abusers and 91 percent of the other substance abusers were also dependent on those substances. Seventy-five percent of the offenders obtained more than one psychiatric diagnosis (figure 4). All participants with PD also had SUD, but only half of those with no PD had SUD. The prevalence of PD and APD among offenders with dual disorders was 66 percent and 61 percent, respectively. The prevalence of PDs (table 2) was significantly higher among die group with schizophrenia (n = 65, x 2 = 4.44, df= \,p = 0.035) than among the remaining subjects (n = 20). The group with schizoaffective disorder (n = 15) had a significantly higher prevalence of SUD than the remaining subjects {n = 73, x 2 = 14.86, df=l,p = 0.0001). There was no substantial difference between tie persons who were admitted to the hospital during the last 3 years and those who had been in the hospital for more than 3 years, concerning the prevalence of PD (x 2 = 0.10, df= 1, p = 0.7573, n = 85) or SUD (X2 = 1.13, df= I, p = 0.287, n = 88). Nor was there a difference between those who committed a homicide and those who attempted to commit a homicide, concerning the prevalence of PD (x 2 = 1.26, df= l,p = 0.263, n = 85) or SUD (x 2 = 1.86, df = \,p = 0.173, n = 88). Discussion These results demonstrated that there are three distinct diagnostic categories of psychotic persons who kill or try to kill others (figure 4). A triple diagnosis (MMD + APD + SUD), die largest category, included about half (47%) of the mentally ill homicide offenders. A "pure" dual diagnosis (MMD + SUD) was found among a quarter (24%), and only a quarter (25%) had "pure" MMD. The fourth possible category, "APD and MMD but no SUD," was not found among this nationally representative sample of men with MMD who had killed or tried to kill someone. Results The distribution and comorbidity of different MMDs, PDs, and SUDs are shown in figures 1, 2, and 3, respectively. Figure 4 illustrates the comorbidity of substance use and personality disorders and three diagnostic categories. For comparison, previous studies on mentally ill homicidal offenders are listed in table 1. The prevalence 63 A. Putkonen et al. Schizophrenia Bulletin, Vol. 30, No. 1, 2004 Figure 1. Psychotic disorders among mentally III persons with homicidal behavior (n = 90) Other psychosis 5% Schizoaffective disorder 17% Schizophrenia 78% of the codisorders and provide important new data from severe violence of psychotic persons. SUDs, particularly alcohol use disorders, are known to increase the risk of homicide (Eronen et al. 1996a) among persons with MMD. However, the relationship between APD and severe violence of persons with MMD has been unclear. Structured interview studies have demonstrated that lifetime APD is common in prison populations, both among nonpsychotic criminal offenders (49%-61%) and among randomly selected males with MMD convicted of various crimes in Quebec penitentiaries (63%, n - 38) and in Chicago Cook County Jail (81%, n = 65) (C6t£ and Hodgins 1990; Abram and Teplin 1991). However, prison populations are biased and exclude offenders found not guilty by reason of insanity. Hodgins et al. (19966) hypothesized that it is the syndrome of stable antisocial behavior rather than substance abuse that is related to offending among persons with schizophrenia. The present study demonstrated that in severe violence of individuals with MMD, lifetime SUD is diagnosed in 74 percent, and APD in 47 percent. However, neither APD nor SUD alone but the combina- To our knowledge, our study was the first that reported a high prevalence of APD (47%, figure 2), SUD (74%), and alcohol use disorders (72%, figure 3) among a nationally representative sample of psychotic homicide offenders. The prevalence of SUD (alcoholism) was about 1.6-fold among mentally ill homicide offenders, compared to the rate among persons with schizophrenia in the ECA study (Regier et al. 1990). Previously, it seemed that only 8 to 14 percent of homicide offenders with schizophrenia had a history of APD (Erb et al. 2001) and that the prevalence of alcoholism was lower among psychotic homicide offenders (8%-44%, table 1) than among persons with MMD in the general population. However, the previous studies on nationally representative samples of homicide offenders were made from examination reports for court and hospital documents. A substantial underdiagnosing of SUD by psychiatrists has been demonstrated (Hansen et al. 2000). Also, according to diagnostic hierarchy, lifetime PD has traditionally not been diagnosed in the presence of MMD (Surtees and Kendell 1979). Thus, a structured study with clinical interviews and objective lifetime documentation could result in higher prevalence 64 Schizophrenia Bulletin, Vol. 30, No. 1, 2004 Mentally 111 Homicide Offenders Figure 2. Comorbldlty of PDs among mentally III persons with homicidal behavior (n = 85)1 ^APDonly34% No PD 49% APD = 47% BPD= 11% OPD = APD + BPD 3% avoidant PD (5.8%) obsessive-compulsive PD (3.5%) passive-aggressive (3.5%) depressive (2.3%) narcissistic (2.3%) histrionic (1.2%) schizoid (1.2%) APD + BPD + OPD 6% BPDonly 1% APD + OPD 5% OPD only 2% Note.—APD = antisocial personality disorder; AUD - alcohol use disorder; BPD = borderline personality disorder; OPD = other personality disorder; PD = personality disorder. 1 Five patients could not be assessed. SUD (alcoholism)" may be rare but in any case is not associated with homicidal behavior. tion of both lifetime APD and SUD (alcohol use disorder) was the most "dangerous" category among persons with MMD. The prevalence of this triple diagnosis (APD + SUD + MMD) was nearly two times greater than the prevalence of pure dual diagnosis (SUD + MMD) or pure MMD. Also, among all persons with dual diagnoses (MMD + SUD), those with an additional history of APD had a particularly high risk for severe violence and accounted for nearly two-thirds (61%) of the homicidal acts of this group. However, APD was not found among 53 percent of homicide offenders. Our result that APD without SUD was not found among mentally ill homicide offenders could suggest that all subjects having MMD and APD in communities would also have alcoholism. However, a structured interview study by Hodgins et al. (19966) demonstrated that among 74 male schizophrenia patients consecutively discharged from a security hospital and two psychiatric hospitals in Canada, 27 percent (n = 20) had APD. The prevalence of alcohol use disorder was only 45 percent and of other SUD 70 percent. Thus, 55 percent did not have alcohol use disorder. (The prevalence of alcohol use disorder among non-APD schizophrenia patients was 20%.) We suggest that the combination "MMD and APD but no APD Among Persons With MMD in Community and Treatment Settings. We have not found any community study that demonstrates the prevalence of APD among a nationally representative sample of persons with MMD. Such data would be needed to compare the prevalence of APD in homicidal and nonhomicidal men suffering from MMD. The prevalence of DSM-III APD in structured interview studies among persons with MMD in different treatment settings varied between 1 percent and 81 percent and was highest in prisons (Abram and Teplin 1991). In a recent report from U.K. 700 study data (Moran et al. 2003), the prevalence of ICD-10 dissocial PD was 6 percent among the 670 outpatients with MMD in London. Persons with a primary diagnosis of alcoholism had not been included. The prevalence of DSM-IV APD in the present study was 8-fold compared to this rate. Methodological Considerations. Research of violent behavior is complicated by many practical issues. Most violent offenses are mild and not registered in police records, and in most countries a large proportion of 65 Schizophrenia Bulletin, Vol. 30, No. 1, 2004 A. Putkonen et al. Figure 3. Comorbldlty of AUDs and SUDs among mentally III persons with homicidal behavior (n = 88)1 NoSUD 26% AUD only 38% Other SUD only 2% Other SUD+AUD 34% Note.—AUD = alcohol use disorder; SUD - substance use disorder. 1 Two patients could not be assessed. crimes remain unsolved (International Criminal Police Organization 1998). Moreover, in many countries only a small proportion of all homicide offenders undergo forensic psychiatric examination. Such shortcomings could be circumvented by studying exclusively serious violent crimes, such as homicide, in countries where the elucidation rate is high and most violent offenders are thoroughly investigated. We believe that our sample was representative of insane Finnish males with homicidal behavior because of the high clearing rate of homicides during the years of the sample (95%-98%), the comprehensive pretrial practice of diagnosing MMD among violent offenders, and the practice of sending all homicide offenders with pretrial MMD diagnoses to state psychiatric hospitals. Selective discharge was excluded by comparing the patients who had been in the hospital less than 3 years with those who came over 3 years ago. In general, many individuals tend to understate their behavioral problems and their substance use, even when interviewed. Crime registers do not provide information on most of the items that are included in the diagnostic criteria of DSM-IV APD, such as symptoms of childhood conduct disorder. This emphasizes the importance of obtaining other objective data dating back to childhood. The prevalence of SUD and PD in the present study represents the rate of DSM-IV diagnoses made on the basis of interviews, data on several years of hospital observation, lifetime registers, records, and questionnaires from parents, teachers, and others who knew the patient. However, it is possible that the prevalence of PD and SUD could be even higher. Nolan et al. (1999) reported that comorbid psychopathy as assessed by Hare's criteria was more common (19%) among violent than among nonviolent hospitalized patients with schizophrenia (n = 51), but they did not study clinical diagnoses. Hare's criteria for psychopathy are a way to predict future violence. Because the aim of the present study was to obtain data on the epidemiology of severe violence among persons with MMD and persons with dual diagnoses, we did not study psychopathy but assessed DSM-IV diagnoses with the latest research version of the SCID. Although many persons with high psychopathy scores have APD, all persons with APD do not have psychopathy. Diagnostic instruments derived from the DSM-IV Axis II usually have good test-retest and interrater relia- 66 Mentally 111 Homicide Offenders Schizophrenia Bulletin, Vol. 30, No. 1, 2004 Figure 4. Comorbidity of PDs and SUDs among mentally ill persons with homicidal behavior, three diagnostic categories (n = 84)1 Triple diagnosis (MMD+SUD+PD) 51% "Pure" dual diagnosis (MMD+SUD) 24% Note.—MMD « major mental disorder; PD = personality disorder; SUD = substance use disorder. 1 Six patients could not be assessed. bility, although their validity in assessing the constructs has been questioned (Westen 1997). Studies that compared different rating instruments (Perry 1992) at the beginning of the 1990s showed good agreement for people with any PD. However, the average capacity of different instruments to similarly categorize patients by Axis II diagnosis was low, partly because of a lack of construct validity of DSM-IV personality disorders. Discriminative validity was, however, highest for APD and borderline PD (Hyler et al. 1992; Westen 1997), which have been successfully studied with these instruments. Studies on different diagnostic instruments showed that a PD diagnosis could not be made simply on the basis of direct questions. Clinical observation and information on interpersonal interactions over time were always also needed. This emphasizes the importance of clinical examination and may partly explain the different results from file-based and interview studies. In the ECA study, APD was the only DSM-III—R Axis II disorder investigated, independently of Axis I disorders, because it fulfills the criteria of a clinical syndrome (e.g., the symptoms are highly intercorrelated, APD has a genetic component [Lyons et al. 1995], and it is found in every society). Because APD was the main target of interest in our study, we considered the SCID to be the best research instrument available for it. Criminal history does not necessarily mean that a person has both conditions of APD diagnosis (i.e., at least two symptoms of childhood conduct disorder and at least three symptoms of adult antisocial behavior). In selected populations, such as prison populations, the SCID—II may not provide high discrimination power. However, in populations where APD is less common and the information on childhood conduct disorder and adult antisocial behavior is available, the SCID for DSM-IV Axis II disorders is useful and gives valuable information about the etiology of violent behavior. A person who has behaved violently since childhood may fulfill the above-mentioned DSM-IV criteria of APD. However, all persons with APD are not violent, and one instance of violent behavior like homicide does not indicate a diagnosis of APD. Only one of the seven other symptoms of APD, "the pervasive pattern of disregard for and violation of the rights of others," is irritability or aggressivity, although three symptoms are needed for the diagnosis. Likewise, only 47 percent of psychotic homicide offenders in the present study were diagnosed with APD. 67 Schizophrenia Bulletin, Vol. 30, No. 1, 2004 A. Putkonen et al. Table 2. The prevalence of PD and SUD in the main groups of major mental disorders among homicidal patients Schizophrenia (n = 70) Schizoaffective Disorder (n = 15]I Other Psychoses (n == 5) Total n % n % n % n % PD PD NoPD PD could not be assessed APD BPD OPD APD + BPD APD + OPD BPD + OPD 37 28 5 35 8 9 7 7 4 56.9 43.1 7.1 52.2 12.1 13.6 10.8 10.6 6.2 5 10 0 4 1 4 1 2 1 33.3 66.7 0 26.7 6.7 26.7 6.7 14.3 6.7 1 4 0 1 0 0 0 0 0 20.0 80.0 0 20.0 0 0 0 0 0 43 42 5 40 9 13 8 9 5 50.6 49.4 5.6 47.0 10.6 15.3 9.4 10.5 5.9 SUD SUD No SUD SUD could not be assessed AUD OSUD AUD, no OSUD OSUD, no AUD AUD + OSUD 50 18 2 49 29 20 1 28 73.5 26.5 2.9 72.1 42.6 29.4 1.5 41.2 12 3 0 11 3 9 1 2 80.0 20.0 0 73.3 20.0 60.0 6.7 13.3 3 2 0 3 0 3 0 0 60.0 40.0 0 60.0 0 60.0 0 0 65 23 2 63 32 32 2 30 73.9 26.1 2.3 71.6 36.4 36.4 2.3 34.1 PD and SUD PD, no SUD SUD, no PD No SUD, no PD PD or SUD not assessed 37 0 12 16 5 56.9 0 18.5 22.9 7.1 5 0 7 3 0 33.3 0 46.7 20.0 0 1 0 2 2 0 20.0 0 40.0 40.0 0 43 0 21 21 5 50.6 0 24.7 24.7 5.6 Note.—APD - antisocial personality disorder; AUD - alcohol use disorder; BPD = borderline personality disorder; OPD - other personality disorder; OSUD = other substance use disorder; PD = personality disorder; SUD - substance use disorder. In the McArthur Study (Steadman et al. 1998) no significant difference was found between the prevalence of violence by discharged patients (n = 51) and persons living in the same neighborhoods, a result that seems to contradict several previous and subsequent studies among persons with schizophrenia. However, less than a fifth of the patients followed in that study were diagnosed with schizophrenia (17.2%). And, as Steadman et al. (1998) reported, followed-up patients were less likely to have a documented history of violence than patients lost to followup. Furthermore, 44 percent of the patients with schizophrenia refused to participate in the study, which is a high proportion that is likely to include most antisocial personalities with schizophrenia. tries. The population in Finland, with over 5 million inhabitants, is considered to be socially and racially homogeneous. Organized crime, illegal drug abuse, and gang violence have been less common in Finland than in most other Western countries. The homicide rate, however, has been higher in Finland than in most European countries (2.14-3.03 per 100,000 population), but it is still only one-third of the rate found in the United States (7.9-9.8 per 100,000 population) (Eronen et al. 1997). About 77 percent of all homicide offenders in Finland were heavily intoxicated by alcohol during the homicide (Virkkunen 1974). There are, unfortunately, no large epidemiological studies on the prevalence of APD and SUD in the general population, or among persons with schizophrenia in Finland. In a large birth-cohort study (n = 11,017), males with coexisting schizophrenia and alcoholism (n = 11) were 25.2 times more likely to commit violent crimes than mentally healthy men, and 36 percent had already committed violent crimes (Rasanen et al. 1998), but no one had committed homicide. However, National Considerations. There are no priori reasons to believe that substantial national differences exist in the prevalence of APD and SUD in Western countries. However, the possibility may not be totally ruled out until structured clinical studies are performed in other coun- 68 Mentally Dl Homicide Offenders Schizophrenia Bulletin, Vol. 30, No. 1, 2004 even non-SUD males with schizophrenia had a 3.6 times higher risk for violent crimes than males without mental disorders. None of the women with schizophrenia (n = 25) had committed any crimes. Low socioeconomic status (SES) did not increase the risk of violence among males with schizophrenia, as boys with schizophrenia from high-SES homes had a higher risk for violent crimes than boys with schizophrenia from low-SES homes (Tiihonen et al. 1997). Seven percent of all male violent offenders of the cohort were diagnosed as psychotic by the age of 26. this underdiagnosed subgroup of mentally ill persons with a history of APD and SUD, and the subsequent lack of effective treatments, is likely to be associated with their poor outcome and increased risk for severe violence. For instance, the insufficient response of violent offenders to traditional psychiatric treatments, which are usually targeted to psychotic symptoms and only sometimes to dual disorders, may be a consequence of the high prevalence of APD among violent offenders. In the treatment of violent offenders with MMD, distinguishing the three categories (persons with triple diagnoses, persons with pure dual diagnoses, and persons with pure MMD) is of clinical importance because the risk factors for violence and the treatment needs of each group are likely to be different Antisocial peers, disadvantaged neighborhoods (Silver et al. 1999), and easy access to alcohol and some other psychoactive drugs may be particularly detrimental for patients with a triple diagnosis (APD + SUD + MMD). Early detection of psychotic symptoms and administration of novel antipsychotic medication in the early phase of the MMD may decrease substance abuse (Drake and Mueser 2000), symptoms of APD (Benedetti et al. 1998), and violent behavior. The effects of integrated treatments for dually diagnosed persons might be improved if the persons with pure dual disorders and those with a history of APD were treated in separate settings. Further research is needed to demonstrate whether the prognosis of different groups of violent offenders with MMD can be improved by specific integrated, multidisciplinary, long-term treatment programs, according to the needs of persons with dual and triple diagnoses. The prevention of severe violence by mentally ill persons necessitates that effective treatments be created for those with dual diagnoses who also have a history of APD. Treatment A dual diagnosis (i.e., the combination of MMD and SUD) is associated with poor treatment outcome (Drake and Mueser 2000), increased psychotic symptoms (Negrete et al. 1986; Drake et al. 1989), medication noncompliance (Drake et al. 1989), hostile and threatening behavior (Drake et al. 1989), depression, suicidal behavior (Bartels et al. 1992), and psychosocial problems such as homelessness (Drake et al. 1991). Persons with dual diagnoses have an increased vulnerability toward negative outcomes, which include violence, legal problems, and incarceration, and they are less capable of being helped by traditional psychiatric or substance abuse treatments. Alcohol and most other psychoactive drugs increase the risk for violent behavior by pharmacologically disinhibiting aggressive impulses (Virkkunen 1974), which can increase conflict and volatility in social relations, thus exacerbating symptoms of perceived threat and hostility (particularly in persons with active psychoses), substituting for or interfering with prescribed psychotropic medications that might otherwise control high-risk symptoms, increasing economic stress and survival demands, and, finally, exposing the user to criminal affiliations and surroundings. The violent acts of persons with APD and SUD may result from certain psychotic symptoms (Link et al. 1992), although the violence is more likely to reflect interactions between several different factors (e.g., personality traits, history of violent behavior, substance abuse [Taylor et al. 1998]) and/or originate from childhood antisocial behavior (Arsenault et al. 2000; Tengstrom et al. 2001). There are promising data of integrated treatments for dually diagnosed persons (Ridgely et al. 1990; Drake et al. 1998; Drake and Mueser 2000), but there is not much evidence on specific treatments of persons with triple diagnoses. APD is associated with poor compliance, not only for traditional treatments but also for integrated treatments for dually disordered persons (Robins et al. 1991). However, we have not found any controlled studies of specific treatments for persons with triple diagnoses (MMD + SUD + APD), and, therefore, we do not know if they cannot be treated with the methods currently available. The lack of data on the specific treatment needs of Conclusions Several conclusions can be drawn from this study. First, there are three different diagnostic categories of persons with MMD who kill or try to kill others. About one-half had a triple diagnosis (MMD + APD + SUD), one-quarter had a pure dual diagnosis (MMD + SUD), and one-quarter had pure MMD. The fourth possible category, "APD and MMD but no SUD," was not found. Second, APD (DSM-FV) is an important predictor of severe violence of psychotic persons, but only when comorbid with SUD. Third, among persons with dual diagnoses (MMD + SUD), those with a history of APD are a particular risk group for severe violence. People with triple diagnosis accounted for nearly two-thirds (61%) of the homicidal acts of this group. 69 Schizophrenia Bulletin, Vol. 30, No. 1, 2004 A. Putkonen ct al. Fourth, lifetime SUD, and particularly alcoholism, is an even more important risk factor for severe violence among psychotic males than the previous literature has demonstrated. Among mentally ill homicide offenders, 74 percent had SUD and 72 percent had an alcohol use disorder. Fifth, the prevention of severe violence of persons with MMD necessitates that effective treatments be created for persons with triple diagnoses (MMD + SUD + APD). Drake, R.E.; Osher, F.C.; and Wallach, M.A. Alcohol use and abuse in schizophrenia: A prospective community study. Journal of Nervous and Mental Disease, 177:408-414, 1989. Drake, R.E.; Osher, F.C.; and Wallach, M.A. Homelessness and dual diagnosis. American Psychologist, 46:1149-1158, 1991. Erb, M.; Hodgins, S.; Freese, R.; Miiller-Isbemer, R.; and Jbckel, D. Homicide and schizophrenia: Maybe treatment does have a preventive effect. Criminal Behaviour and Mental Health, 11:6-26, 2001. References Eronen, M. Mental disorders and homicidal behavior in female subjects. American Journal of Psychiatry, Abram, K.M., and Teplin, L.A. Co-occurring disorders among mentally ill jail detainees. Implications for public policy. American Psychologist, 46:1036-1045, 1991. 152:1216-1218, 1995. Eronen, M.; Hakola, P.; and Tiihonen, J. Mental disorders and homicidal behavior in Finland. Archives of General Psychiatry, 53:497-501, 1996a. Eronen, M.; Tiihonen, J.; and Hakola, P. Schizophrenia American Psychiatric Association. DSM-IV: Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: APA, 1994. and homicidal behavior. Schizophrenia Arsenault, L.; Moffitt, T.E.; Caspi, A.; Taylor, P.J.; and Silva, P.A. Mental disorders and violence in a total birth cohort. Results from the Dunedin study. Archives of General Psychiatry, 57:979-986, 2000. Bartels, S.J.; Drake, R.E.; and McHugo, G.J. Alcohol abuse, depression, and suicidal behavior in schizophrenia. American Journal of Psychiatry, 149:394-395, 1992. J.B.W. User's Guide for the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I). Benedetti, F.; Sforzini, L.; Colombo, C ; Maffei, C ; and Smeraldi, E. Low-dose clozapine in acute and continuation treatment of severe borderline personality disorder. Journal of Clinical Psychiatry, 59:103-107, 1998. Research Version. New York, NY: Biometrics Research Department, 1996a. First, M.B.; Gibbon, M.; Spitzer, R.L.; Williams, J.B.W.; and Benjamin, L. User's Guide for the Structured Clinical Interview for DSM-IV Axis II Disorders (SCID-II). Research Version. New York, NY: Biometrics Research Department, 1996Z?. Black, D.W.; Bell, S.; Hulbert, J.; and Nasrallah, A. The importance of Axis II in patients with major depression: A controlled study. Journal of Affective Bulletin, 22(l):83-89, 1996fc. Eronen, M.; Tiihonen, J.; and Hakola, P. Psychiatric disorders and violent behavior. International Journal of Psychiatry in Clinical Practice, 1:179-188, 1997. First, M.B.; Gibbon, M.; Spitzer, R.L.; and Williams, Disorders, 14:115-122, 1988. Gabrielsen, G.; Gottlieb, P.; and Kramp, P. Criminal homicide trends in Copenhagen. Studies on Crime and Crime Prevention, 1:106-114, 1992. Brennan, P.A.; Mednick, S.A.; and Hodgins, S. Major mental disorders and criminal violence in a Danish birth cohort Archives of General Psychiatry, 57:494-500, 2000. Gottlieb, P.; Gabrielsen, G.; and Kramp, P. Psychotic homicides in Copenhagen from 1959 to 1983. Acta Psychiatrica Scandinavica, 76:285-292, 1987. Hansen, S.S.; Munk-Jorgensen, P.; Guldbaek, B.; Solgard, T; Lauszus, K.S.; Albrechtsen, N.; Borg, L.; Egander, A.; Faurholdt, K.; Gilberg, A.; Gosden, N.P.; Lorenzen, J.; Richelsen, B.; Weischer, K.; and Bertelsen, A. Psychoactive substance use diagnoses among psychiatric C6te", G., and Hodgins, S. Co-occurring mental disorders among criminal offenders. Bulletin of the American Academy of Psychiatry and the Law, 18:271-281,1990. C6te\ G., and Hodgins, S. The prevalence of major mental disorders among homicide offenders. International Journal of Law and Psychiatry, 15:89-99, 1992. Drake, R.E.; Mercer-McFadden, C ; Mueser, K.T.; McHugo, GJ.; and Bond, G.R. Review of integrated mental health and substance abuse treatment for patients with dual disorders. Schizophrenia Bulletin, 24(4):589-608, 1998. in-patients. Acta Psychiatrica Scandinavica, 102:432-438, 2000. Hodgins, S.; Mednick, S.A.; Brennan, P.A.; Schulsinger, F.; and Engberg, M. Mental disorder and crime: Evidence from a Danish birth cohort. Archives of General Psychiatry, 53:489-496, 1996a. Drake, R.E., and Mueser, K.T. Psychosocial approaches to dual diagnosis. Schizophrenia Bulletin, 26(1): 105-118, 2000. 70 Schizophrenia Bulletin, Vol. 30, No. 1, 2004 Mentally 111 Homicide Offenders an unselected birth cohort. Schizophrenia Bulletin, 24(3):437^t41, 1998. Regier, D.A.; Farmer, M.E.; Rae, D.S.; Locke, B.Z.; Keith, S.J.; Judd, L.L.; and Goodwin, F.K. Comorbidity of mental disorders with alcohol and other drug abuse: Results from the Epidemiological Catchment Area (ECA) study. Journal of the American Medical Association, 264:2511-2518, 1990. Hodgins, S.; Toupin, J.; and C6te\ G. Schizophrenia and antisocial personality disorder: A criminal combination. In: Schlesinger, L.B., ed. Explorations in Criminal Psychopathology. Clinical Syndromes With Forensic Implications. Springfield, IL: Charles C. Thomas, 1996fc. pp. 217-237. Hyler, S.E.; Skodol, A.E.; Oldham, J.M.; Kellman, H.D; and Doidge, N. Validity of the Personality Diagnostic Questionnaire-Revised: A replication in an outpatient sample. Comprehensive Psychiatry, 33:73-77, 1992. Crimes Statistics, 1996-1997. Lyon, France: The Ridgely, M.S.; Goldman, H.H.; and Willenbring, M. Barriers to the care of persons with dual diagnoses: Organizational and financing issues. Schizophrenia Bulletin, 16(1): 123-132, 1990. Organization, 1998. Lindqvist, P. Criminal homicide in Northern Sweden 1970-1981: Alcohol intoxication, alcohol abuse and mental disease. International Journal of Law and Psychiatry, 8:19-37, 1986. Robins, L.N.; Tipp, J.; and Przybeck, T. Antisocial personality. In: Robins, L.N., and Regier, D., eds. Psychiatric Disorders in America: The Epidemiologic Catchment Area Study. New York, NY: Macmillan/Free Press, 1991. pp. 258-290. Link, B.G.; Callen, F.T.; and Andrews, H. The violent and illegal behavior of mental patients reconsidered. American Sociological Review, 57:275—292, 1992. Silver, E.; Mulvey, E.P.; and Monahan, J. Assessing violence risk among discharged psychiatric patients: Toward an ecological approach. Law and Human Behavior, 23:237-255, 1999. International Criminal Police Organization. International Lyons, M.J.; True, W.R.; Eisen, S.A.; Goldberg, J.; Meyer, J.M.; Faraone, S.V.; Eaves, L.J.; and Tsuang, M.T. Differential heritability of adult and juvenile antisocial traits. Archives of General Psychiatry, 52:906-915, 1995. Steadman, H.J.; Mulvey, E.P.; Monahan, J.; Robbins, P C ; Appelbaum, P.S.; Grisso, T ; Roth, L.H.; and Silver, E. Violence by people discharged from acute psychiatric inpatient facilities and by others in the same neighborhoods. Archives of General Psychiatry, 55:393-401, 1998. Moran, P.; Walsh, E.; Tyrer, P.; Burns, T; Creed, F.; and Fahy, T. Impact of comorbid personality disorder on violence in psychosis: Report from the UK700 trial. British Journal of Psychiatry, 182:129-134,2003. Surtees, P.G., and Kendell, R.E. The hierarchy model of psychiatric symptomatology: An investigation based on Present State Examination ratings. British Journal of Psychiatry, 135:438-443, 1979. Negrete, J.C.; Knapp, W.P.; Douglas, D.; and Smith, W.P. Cannabis affects the severity of schizophrenic symptoms: Results of a clinical survey. Psychological Medicine, 16:515-520, 1986. Swanson, J.W.; Holzer, C.E., HI; Ganju, V.K.; and Jono, R.T. Violence and psychiatric disorder in the community: Evidence from the Epidemiologic Catchment Area surveys. Hospital and Community Psychiatry, 41:761-770, 1990. Nolan, K.A.; Volavka, J.; Mohr, P.; and Czobor, P. Psychopathy and violent behavior among patients with schizophrenia or schizoaffective disorder. Psychiatric Services, 50:787-792, 1999. Taylor, P.J., and Gunn, J. II. Effect of psychiatric diagnosis on conviction and sentencing of offenders. British Medical Journal, 289:9-12, 1984. Perry, J.C. Problems and considerations in the valid assessment of personality disorders. American Journal of Psychiatry, 149:1645-1653, 1992. Taylor, P.J.; Leese, M.; Williams, D.; Butwell, M.; Daly, R.; and Larkin, E. Mental disorder and violence. A special (high security) hospital study. British Journal of Psychiatry, 172:218-226, 1998. Putkonen, H.; Collander, J.; Honkasalo, M-L.; and LOnnqvist, J. Finnish female homicide offenders 1982-92. Journal of Forensic Psychiatry, 9:672-684, 1998. TengstrSm, A.; Hodgins, S.; and Kullgren, G. Men with schizophrenia who behave violently: The usefulness of an early- versus late-start offender typology. Schizophrenia Bulletin, 27(2):205-218, 2001. Putkonen, H.; Collander, J.; Honkasalo, M-L.; and LOnnqvist, J. Personality disorders and psychoses form two distinct subgroups of homicide among female offenders. Journal of Forensic Psychiatry, 12:300-312, 2001. Tiihonen, J.; Hakola, P.; Eronen, M.; Vartiainen, H.; and RyynSnen, O-P. Risk of homicidal behavior among discharged forensic psychiatric patients. Forensic Science International, 79:123-129, 1996. RSsSnen, P.; Tiihonen, J.; Isohanni, M.; Rantakallio, P.; Lehtonen, J.; and Moring, J. Schizophrenia, alcohol abuse, and violent behavior A 26-year followup study of 71 Schizophrenia Bulletin, Vol. 30, No. 1, 2004 A. Putkonen et al. Tiihonen, J.; Isohanni, M.; RSsa'nen, P.; Koiranen, M.; and Moring, J. Specific major mental disorders and criminality. A 26-year prospective study of the 1966 northern Finland birth cohort. American Journal of Psychiatry, 154:840-845, 1997. Virkkunen, M. Alcohol as a factor precipitating aggression and conflict behaviour leading to homicide. British Journal of Addiction, 69:149-154, 1974. Westen, D. Divergences between clinical and research methods for assessing personality disorders: Implications for research and the evolution of axis II. American Journal of Psychiatry, 154:895-903, 1997. Woody, G.E.; McLellan, T.; Luborsky, L.; and O'Brien, C.P. Sociopathy and psychotherapy outcome. Archives of General Psychiatry, 42:1081-1086, 1985. 72 Acknowledgments The authors thank Ms. Aija Ra"sSnen and Mrs. Tarja Mehtonen for secretarial assistance. The Authors Anu Putkonen, M.D., is Forensic Psychiatrist; Irma Kotilainen, M.D., is Forensic Psychiatrist; and Christian C. Joyal, Ph.D., is Visiting Researcher, Department of Forensic Psychiatry, University of Kuopio and Niuvanniemi Hospital, Kuopio, Finland. Jari Tiihonen, M.D., Ph.D., is Professor and Chairman, Department of Forensic Psychiatry, University of Kuopio and Niuvanniemi Hospital; Senior Lecturer, Department of Psychiatry, University of Helsinki, Helsinki, Finland; and Consultant, Department of Clinical Physiology, Kuopio University Hospital, Kuopio, Finland.