Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Clinical Science (1992) 83, 149-155 (Printed in Great Britain)
I49
Disparities in circulatory adjustment to standing between
young and elderly subjects explained by pulse contour
analysis
W. WIELING, D.
P. VEERMAN, J. H. A. DAMBRINK and B. P. M. IMHOLZ
Department of Internal Medicine, University of Amsterdam, Academic Medical Centre.
Amsterdam, The Netherlands
(Received 28 October 1991/3 February 1992; accepted 10 March 1992)
1. The circulatory adjustment to standing was investigated in two age groups. Young subjects consisted of
20 healthy 10-14-year-old girls and boys. Elderly
subjects consisted of 40 70-86-year-old healthy and
active females and males. Continuous responses of
blood pressure and heart rate were recorded by
Finapres. A pulse contour algorithm applied to the
finger arterial pressure waveform was used to assess
stroke volume responses.
2. During the first 30s (initial phase), an almost
identical drop in mean blood pressure was found in
both age groups (young, 16+10mmHg; old,
17f lOmmHg), but the initial heart rate increase
was attenuated in the elderly subjects (young,
29 f 7 beats/min; old, 17 7 beats/min).
3. During the period from 30 s to 10min of standing,
mean blood pressure increased from 96 f 12 to
106f 12mmHg in the elderly subjects compared with
almost no change in the young subjects (from 8 2 f 8
to 84 f 7mmHg). In the elderly subjects a progressive
increase in total peripheral resistance (from
114f 14% to 146f29%) was found, compared with
an initial rapid increase in total peripheral resistance
(126+18% after 30s) with no further change during
prolonged standing (124f17% after 10min) in the
young subjects. In this age group the decrease in
stroke volume and the increase in heart rate after
10min of standing were large (young, -37+11%
and 27 f 11beats/min; old, - 31f 9% and 7 f 6 beats/
min, respectively).
4. In conclusion, young subjects adjust to orthostatic
stress mainly by a marked increase in heart rate. In
healthy elderly subjects an attenuation of the heart
rate response during orthostatic stress is compensated
by a pronounced increase in total peripheral resistance resulting in an increase in blood pressure.
+
INTRODUCTION
In earlier studies we reported the magnitude and
time course of blood pressure (BP) and heart rate
(HR) responses induced by standing in healthy 10-
14-year-old children [11 and healthy 70-86-year-old
subjects [2], using continuous monitoring of finger
arterial BP [3, 41.
In the present study we extended these observations by analysing the differences in circulatory
adjustment to standing between young and elderly
subjects in detail. We compared not only BP and
HR responses, but also changes in stroke volume
(SV), cardiac output (CO) and total peripheral
resistance (TPR) by applying a pulse contour algorithm to the finger arterial BP waveform [5, 61.
Three specific questions raised in our previous
studies [l, 21 were addressed:
(1) Why do young and elderly subjects have a
comparable initial BP drop upon standing notwithstanding the attenuation of the initial HR response
in old age [l, 2]?
(2) Is the progressive rise in BP in the elderly
during prolonged standing accompanied by a progressive increase in TPR [2]?
(3) Is the large HR increase present in young
subjects during prolonged standing accompanied by
an equally large fall in SV [l]?
METHODS
Subjects
The responses of 10 girls and 10 boys aged 10-14
years and of 20 healthy females and 20 healthy
males aged 70-86 years were investigated. A detailed
description of the setting of the study, the selection
procedure and the anthropometric data of the subjects has been given previously [l, 21.
Measurements
Continuous non-invasive finger arterial BP was
recorded by means of a TNO Finapres model 5 [3].
It has been demonstrated previously that, in steadystate conditions, finger mean arterial BP is 510mmHg below brachial arterial BP owing to the
pressure gradient between the brachial and the
Key words: ageing, cardiac output, heart rate, non-invasive continuous blood pressure, orthostatic hypotension, postural changes, stroke volume, total peripheral resistance.
Abbreviations: BP, blood pressure; CO, cardiac output; HR, heart rate; SV, stroke volume; TPR, total peripheral resistance.
Correspondence: Dr W. Wieling, Department of Internal Medicine, F4-222, Academic Medical Centre, Meibergdreef 9, I105 AZ Amsterdam, The Netherlands.
I50
W. Wieling et al.
finger artery [4, 71. Changes in arterial BP during
laboratory tests, including orthostatic manoeuvres,
are followed reliably by Finapres [3, 4, 7, 81.
Subjects were instructed to keep the measuring
finger cuff at heart level to avoid interference of
hydrostatic pressure differences. For direct inspection during the measurement from each subject, a
single-lead ECG was recorded and was input to a
cardiotachometer to obtain instantaneous HR responses. Together with BP, HR and an event
marker, this was recorded on a strip chart (7402-A,
Hewlett-Packard, Los Angeles, CA, U.S.A.). For offline analysis, the ECG, the BP signal and the event
marker were recorded on tape using a cassette data
recorder (TEAC R-61; TEAC Corp, Tokyo, Japan).
The standing-up manoeuvre was performed after
5 min of supine rest and subjects remained standing
for 10min. The duration of the time from the onset
of the manoeuvre to stable stand was marked. In
some elderly subjects, an assisting hand was needed
to ensure a quick change of posture.
Data analysis
Upon playback, a 30s control period before and
10min after the onset of standing were selected for
further analysis. First, the Finapres BP and the
event-marker signals were analog-to-digital converted at a sampling rate of 200Hz and were input
into a PDP-11/44 computer system [l, 21.
By means of the signal analysis program BEATFAST [9], the beat-to-beat integrated mean BP and
the instantaneous HR values were determined. In
addition, this program calculates the beat-to-beat
values of left ventricular SV, CO and TPR using the
pulse contour algorithm of Wesseling et al. [5]. In
short, SV is calculated as the integral of the pressure
pulse over the arterial systolic period divided by the
aortic characteristic impedance [ 5 , 61.
Smith et al. [lo], using radial and brachial artery
waveforms, found pulse contour CO in good agreement with dye-dilution measurements, while varying
BP, HR and CO over a wide range by pharmacological intervention. Wesseling et al. [l 11, on estimating the transfer function between aortic and
brachial waveforms, found a constant (15%) overestimation of SV from the brachial pulse contour
data. We have shown previously that when intrabrachial measurements upon standing are repeated
within a short time period, almost identical
responses are obtained both for the arterial BP
measurements and for the pulse contour computations [12].
To obtain absolute SV values, calibration with a
standard method such as thermodilution is needed
[5, 12, 131, but without such calibration one can use
the relative changes in SV [ 5 , 61.
The reliability of the use of the pulse contour
algorithm in BEATFAST on indirect finger arterial
BP waveforms has not yet been evaluated. We,
therefore, compared pulse contour data from simul-
taneously measured intrabrachial and finger BP
tracings recorded during standing up in a previous
study [4]. The results of this evaluation are given
separately in the Results section.
Calculations
After the calculation of beat-to-beat values, corrections were made for occasional ectopic beats by
means of linear interpolation. In three of the 40
elderly subjects, the extent of ectopic beats during
one of the stages of prolonged standing was too
large and made the interpolation unreliable. Individual responses of the remaining 37 elderly and the
20 young subjects were averaged to obtain group
responses.
The onset of standing up was taken as t=O.
Average BP and HR values of a 30s period before
standing were taken as controls. The circulatory
adjustment to standing was divided into three
phases as described previously [l, 23: an initial
phase (first 30 s) with characteristic changes in BP
and HR, an early steady-state phase (1-2 min standing) and a phase of prolonged standing (5-10min
upright). The circulatory responses in the three time
periods were quantified as follows.
(1) Initial response (first 30s). The changes in BP
and HR from control and the percentage changes in
SV, CO and TPR were determined each 0.5s. In
contrast to earlier studies [l, 2, 61, we did not
sample at characteristic peaks and troughs, since
these points could not always be identified clearly
for all variables in the elderly subjects.
(2) Early steady-state response (1-2 min of standing). The changes in BP and HR from control and
the percentage changes in SV, CO and TPR during
a 10s period centred at 1 and 2min of standing
were calculated [l, 21.
(3) Prolonged standing (5-10min of standing). The
changes in BP and HR from control and the
percentage changes in SV, CO and TPR during a
10 s period centred at 5 and 10min of standing were
calculated [l, 21.
Influence of the level of supine BP on circulatory
responses upon standing up
In our previous study in elderly subjects [2] it
was found that the level of supine BP affected the
changes in BP during prolonged standing. We
therefore analysed the circulatory responses after 2,
5 and 10min standing of ten elderly subjects with
the lowest supine mean BP values (lower BP quartile) and the ten elderly subjects with the highest
supine mean BP values (upper BP quartile).
Statistics
Two-way analysis of variance was used to compare the data of the two age groups and the
Orthostatic circulatory adjustment: young compared with elderly
151
different instants of measurements. Student’s t-test
for unpaired observations was used to perform
comparisons between the two age groups. A P value
of <0.05 was considered significant. Results are
expressed as means SD.
+
RESULTS
SOJ
Comparison of the pulse contour analysis applied to
simultaneously recorded intrabrachial and finger arterial
waveforms
:
lsol
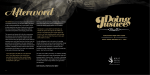
This comparison was based on BP tracings
recorded in 11 healthy subjects aged 18-40 years
during standing up [4]. Group average brachial and
finger mean arterial BP and HR responses during
orthostatic stress are given in the upper two panels
of Fig. 1. The lower three panels show the group
average percentage changes in SV, CO and TPR
calculated from both signals. The mean Finapres
arterial BP upon standing was somewhat lower
than the intrabrachial arterial BP. The changes in
SV, CO and TPR in a period up to 2min standing
of Finapres and intrabrachial arterial BP are almost
identical.
50’
I
50-]
Control period
Supine BP was substantially higher in the elderly
subjects; supine HR did not differ (Table 1).
Initial response (first 30s)
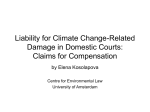
In the young subjects (Fig. 2) the standing up
manoeuvre was performed in 3 f1s. It was accompanied by an 8+8mmHg rise in mean arterial BP
at 2.5s and an instantaneous large increase in HR.
This immediate BP increase was followed by a
pronounced drop in pressure to a minimum of
16f10mmHg below the control level at 9 s after the
start of standing up. The increase in HR reached
a maximum of 29+7beats/min after 12s. Upon
standing, SV remained unchanged for 7s. The combination of an increase in HR and a stable SV in
this phase resulted in a rise in CO, with a maximum
of 143& 23% after 6 s. A drop in BP despite a rise in
CO can only be explained by a reduction in TPR a
minimum of 60f8% was reached at 9 s after the
start of the manoeuvre. After 9s, at the moment
when CO was still elevated, TPR started to increase.
BP recovered and even showed a slight overshoot.
HR showed a subsequent rapid decrease around
21s. At the end of the initial phase SV had decreased to 68+ 12% and CO to 86f 14%. Meanwhile, TPR had increased to a value of 126+18%
and BP had increased by 4+7mmHg.
In the elderly subjects (Fig. 2), the standing up
manoeuvre took significantly longer (6 f 1 s,
P<O.OOl compared with young subjects) and the
immediate increase in BP upon standing was significantly more pronounced (17 f 10mmHg, P <0.001
sE
I-
1
0
~
. . . .......................................
100
501
-I5
5
\
0
I
I
30
I
I
I
60
Time (s)
90
,
1
I20
Fig. I. Average mean intrabrachial and finger BP (MAP) and HR
responses during a period up to Zmin of standing in II adult
subjects [4]. Average relative SV, CO and TPR responses calculated from
the direct brachial artery BP waveform are indicated by the solid line, and
data from the simultaneously recorded indirect finger BP waveform as a
broken line.
compared with young subjects). This increase was
accompanied by a large drop in SV to a minimum
of 58 19% at 2 s after the onset of standing, a drop
in CO to 63+20% and a concomitant increase in
TPR of 170+47%. At 9.5s, the immediate increase
in BP was followed by a fall of 17 10mmHg from
the control value, similar to that in the young
subjects. The maximal increase in HR, occurring at
14 s, was smaller in the elderly subjects (17 7 beats/
min, P<O.Ol compared with young subjects). The
+
+
+
I52
W. Wieling et al.
Table I. Orthostatic responses in young and elderly subjects. Values
are means SD. Statistical significance: *P <0.05, **P <0.01, ***P <0.00 I
+
compared with young subjects. Abbreviation: MAP, finger mean arterial BP.
Young
subjects
(IC-I5 years)
(n =20)
Supine
MAP(mmHg)
HR (beatslrnin)
sv (%)
co (%I
TPR (%)
Upright
I min
MAP(mmHg)
HR (beatslmin)
sv (%I
co (%I
TPR (%)
2min
MAP(mmHg)
HR (beatslmin)
sv (%)
co (%I
TPR (%)
5min
MAP(mmHg)
HR (beatslmin)
sv 6)
co (%I
TPR (%)
IOmin
MAP(mmHg)
HR (beatslmin)
sv (%I
co (%I
TPR (%)
Elderly
subjects
(>70 years)
(n = 37)
76+6
63+9
100
I00
100
96 f lo***
59+8
I00
I00
I00
7+6
20+ 10
-34+9
- 12+ 10
25+ 10
I +9**
9 7***
-24+ lo***
-13+12
17+24
7+6
22+11
-36+ I I
- 12+ 10
28, I 6
6+8
7 6***
-28+11*
- l8+ I3
34 & 27
9+5
23+ 10
-36+ I I
- I 2 + I I*
28+ I6
7-1: 10
6 6***
-29+11*
-19+11*
38 29
7+7
27+11
-37+ I I
- l o + I3
14+ 17
10+9
7 f6***
-31 +9*
-21 f 14**
46 29**
+
+
+
+
+
fall in BP at 9.5s was again accompanied by a
transient rise in CO, but the magnitude of this rise
was smaller than in the young subjects (127 +20%,
P ~ 0 . 0 5 ) The
.
magnitude of the drop in TPR with a
minimum of 69 _+ 13% near 11 s after the onset of
standing up was also less in the elderly subjects
( P <0.01 compared with young subjects). After 9.5 s,
BP increased, but an overshoot was not observed.
After 30s of standing, orthostatic falls in SV to
77+12% and in CO to 87f13% were observed
(P<O.Ol and P>0.05 compared with young subjects, respectively) with no change in BP. TPR had
increased to 114 14% ( P >0.05 compared with
young subjects).
+
Early steady state (I-2min of standing) and prolonged
standing (5-l0min of standing)
After lmin of standing, mean BP had increased
in the young subjects, but not in the elderly subjects. After 2min, a comparable increase in BP was
present in both groups. The increase in HR and the
decrease in SV remained greater in the young
subjects in this phase (Table 1).
During the period from 1 to 10min after the
onset of standing, BP increased from 96+12 to
106f 12mmHg in the elderly subjects, ( P <0.01),
whereas HR hardly changed. In the young subjects
there were almost no further changes in BP; HR
increased, but not significantly (Fig. 2, Table 1).
At 5 and 10min of standing the increase in HR
and the decrease in SV were still greater in the
young subjects. At the end of the 10min standing
period CO had decreased and TPR had increased
by significantly more in the elderly subjects, but the
BP responses did not differ.
Influence of the level of supine BP on circulatory
responses upon standing up
Upon standing, mean arterial BP increased more
in the lower BP quartile than in the upper BP
quartile (Table 2). In the lower BP quartile the
decrease in CO was 5-10% less than in the upper
BP quartile, but this difference was not significant.
DISCUSS10N
Since the subjects were instructed to keep their
hand at heart level (i.e. just a few centimetres above
the hydrostatic indifference point) when moving
from recumbency to the upright posture, alterations
in finger haemodynamics are consequences of circulatory adjustment to standing [14]. Variations at
the hydrostatic indifference point should not be
extrapolated to other vascular beds. Arterial and
venous pressures taken in the lower part of the
body should be corrected by subtracting the pressure equivalent of the vertical distance of the hydrostatic column of blood below the heart, and pressures in the upper part by adding the distance
above the heart [14].
In the adult validation group, excellent agreement
of the pulse contour data for the simultaneously
measured intrabrachial and finger BP recordings in
a period up to 2min of standing was found (Fig. 1).
Thus, we feel confident that the use of this pulse
contour method on distal peripheral pressure waves
such as those obtained with a Finapres device is
appropriate for the comparison of percentage
changes in SV, CO and TPR in this study.
Initial circulatory response
In the young subjects the initial cardiovascular
responses follow the same time course as reported
for adult subjects [6]. The magnitude of the responses appears to be even more pronounced (Figs.
1 and 2).
The explanation of the characteristic initial response on standing has been described recently [6].
Orthostatic circulatory adjustment: young compared with elderly
IS01
I53
I
;++
50
8
..........................................
+l-
50
50i
200 1
-
-ll-
* i l - -8- ++ .8
I
I
:
-
i ++-I++
.Iti l - .e
i= 100
50
-15
0
15
30
'
60
I20 300 600
Time (I)
-IS
0
15 30
60
I20
300 600
Time (s)
Fig. 2 Group mean finger arterial BP (MAP) and HR responses and relative changes in SV, CO and TPR during the
initial response upon standing. Average responses of 20 young subjects (left panel) and 37 elderly subjects (right panel) are shown.
Briefly, the muscular effort of standing up compresses vessels in the legs and abdomen, causing an
immediate translocation of blood towards the heart
and increasing right atrial pressure. Left ventricular
SV remains stable for the first 5s, most probably
owing to the combination of the blood translocated
towards the heart by the muscular effort of standing
up and the buffering effect of the pulmonary blood
volume [14, 151. The combination of an instantaneous HR increase and a stable SV results in a
pronounced increase in CO, with a maximum
around 7 s after the onset of standing. Simultaneously, a drop in mean arterial BP of about
20mmHg (Figs. 1 and 2) is found. The two phenomena taken together reflect a pronounced drop in
TPR. It is our view that the immediate increase in
right atrial pressure upon standing activates lowpressure receptors, resulting in a reflex release of
vasoconstrictor tone [6]. In contrast, with a passive
head-up tilt, an immediate fall in right atrial pressure has been reported [16] and the transient dip in
arterial pressure is usually not observed [l, 2, 4, 61.
Vasodilatation in the working leg and abdominal
muscles is possibly an additional factor in the drop
in systemic vasoconstrictor tone upon standing, but
the relative contribution of reflex vasodilatation due
to an increase in right atrial pressure and local
vasodilatation in working muscles is unknown [l5].
In the elderly subjects (Fig. 2) standing up evoked
a different cardiovascular response: the immediate
temporary increase in BP during the act of standing
(6s duration) was larger than in the young subjects.
Meanwhile, an abrupt decrease in SV and an
increase in TPR were now observed. These immediate changes resemble the response induced by the
Valsalva manoeuvre [17] and are most probably
due to the straining that accompanied the considerable physical activity needed for this age group to
stand up quickly. From about 7 s after the onset of
standing up the cardiovascular responses in the
elderly subjects appeared similar to those in the
young subjects.
The magnitude of the initial drop in BP did not
differ between the two age groups (Fig. 2). Pulse
contour analysis showed that the almost identical
values of the initial drop in BP could be traced
back to a smaller transient rise in CO combined
with a less pronounced drop in TPR in the elderly
subjects. The reduction in the transient increase in
CO in the elderly subjects is caused by an attenuation of the initial HR response, since SV in both
groups was comparable around 7 s after the onset of
154
W . Wieling et al.
Table 2. Orthostatic responses in elderly subjects subdivided into
upper and lower BP quartiles during prolonged standing. Values are
means SD. Statistical significance: *P <0.05, **P <O.W I compared with
+
u m r BP auartile. Abbreviation: MAP, finner mean arterial BP.
Supine
MAP(mmHg)
HR (beatslmin)
sv 6)
co (%I
TPR (%)
Upright
2min
MAP(mmHg)
HR (beatslmin)
sv (%I
co ("6)
TPR (%)
Upper
BP quartile
Lower
BP quartile
(n=IO)
(n=IO)
108+9
60+7
I00
84 f4**
54+9
I00
I00
I00
100
I00
42+40
12+8*
6+5
-22* 10
--13+8
32+ I9
3+6
7+6
-32+13
-23+ 14
38 33
14+ 12*
s,6
-25+12
-17+9
43 + 32
5+4
7+6
-29+ 12
13+9*
8+5
-29+ I I
- l9+ 10
46 29
3+7
7+5
-32+12
-23+ 15
5 min
MAP (mmHg)
HR (beatslmin)
sv (%I
co (%I
TPR (%)
IOmin
MAP(mmHg)
HR (beatslmin)
sv (%I
co !%)
TPR (%)
+
-25+ll
44+32
standing up (Fig. 2). Attenuation of the initial HR
response on standing in the elderly is a sign of
diminished vagal HR responsiveness; it is attributed
to age-related functional changes in the parasympathetic limb of the arterial baroreflex arc, yet the site
is still debated [18-211.
The less pronounced drop in TPR upon standing
in the elderly subjects might be related to an agerelated reduction in vasodilator capacity. Changes
in end-organ responsiveness or in the capacity
involved in reflex release of vasoconstrictor tone
should be taken into consideration [22-271. It must
be realized, however, that the stimulus inducing
cardiovascular reflex responses must have been
different for the two age groups: in the elderly
standing up was accompanied by a pronounced and
prolonged increase in BP (Fig. 2).
Early steady state and prolonged standing
In the elderly subjects mean BP increased gradually by 10mmHg in the period from 30s to
10min of standing, whereas in the young subjects
BP was more elevated initially, but hardly changed
after 30s of standing. The increase in BP in the
elderly subjects is accompanied by a progressive
increase in TPR during prolonged standing; TPR
increased from 114% to 146% in the period from
30s to 10min of standing (Fig. 2, Table 1).
Although there is no unanimity on the vasoconstrictor response to circulatory stresses in old age, a
tendency towards an augmented response during
prolonged stresses has been reported in some [26,
271 but not all [28] studies. The timing of the
measurement [l, 2, 151 and the use of invasive
versus non-invasive measurements [7, 291 are
important considerations when explaining the discrepancies between studies. In the young subjects an
initial rapid increase in TPR to 125% was found,
with no further change after 30s of standing. Thus
the major difference between the young and old
subjects investigated is the progressive increase in
TPR in the elderly subjects, resulting in a larger
increase in TPR after 2min of standing in the latter
(Fig. 2, Tables 1 and 2).
A large difference in the increase in TPR in
response to orthostasis has been reported in the
literature when adult normotensive subjects and
hypertensive patients were compared: in the hypertensive patients the increase in TPR was greater
[27]. In the present study, in the (mainly normotensive) elderly subjects the level of BP was not an
influence on the TPR responses. The larger increase
in mean BP during prolonged standing in the
elderly subjects with the lower supine BP can be
explained by a less pronounced decrease in CO
upon standing in this group (Table 2).
The increase in HR after 10min of standing in the
young subjects is almost four times as large as in
the elderly subjects (27 versus 7 beats/min). This
large postural increase in HR could be considered
as compensation for the more pronounced decrease
in SV that we found in these subjects (Fig. 2, Table
1). We attribute this to a more pronounced gravitational pooling of blood [30-321 and the consequent reduction in heart size on standing [33, 341.
Smith and co-workers [26, 351 have, indeed, shown
that during lower body negative pressure and the
Valsalva manoeuvre, caudal displacement of blood
is more pronounced in young adult subjects. However, during head-up tilt in adult and elderly male
subjects, there were no significant differences in
thoracic blood volume responses [28].
The postulated increase in peripheral pooling of
blood in the young subjects during orthostatic stress
could be related to the function and/or structure of
the lower limb veins and the surrounding skeletal
muscle [14]. Initial increases in venous volume due
to a shift of blood to the lower part of the body
during orthostasis should be considered, enhanced
by venous stress-relaxation and additional transcapillary fluid movement to the interstitial spaces
[14]. The effect of age on these responses is largely
unknown; evidence of disordered venous innervation
has been reported in adult patients with postural
tachycardia and venous distensibility has been
reported to decrease with ageing [30, 36, 371.
Orthostatic circulatory adjustment: young compared with elderly
CONCLUSIONS
Non-invasive continuous finger BP recording and
pulse contour analysis of the finger arterial waveform enabled us to disclose different haemodynamic
mechanisms underlying cardiovascular adjustment
to orthostatic stress in healthy young and elderly
subjects; it showed that in these age groups postural
stress appears to evoke differential cardiovascular
responses.
In the active elderly subjects orthostatic BP
control appears adequate, despite a blunted HR
response on standing. Our data suggest that in
healthy elderly subjects orthostatic stress evokes a
reduced vasodilatation in the initial phase of standing. On the contrary, during prolonged standing,
pronounced large increases in vascular tone appear
to be the characteristic mechanisms for orthostatic
BP control.
In the young subjects marked increases in HR
during prolonged standing are observed, most likely
as a response to increased gravitational pooling of
blood below the level of the diaphragm.
REFERENCES
I. Dambrink, J.H.A., Imholz, B.P.M., Karemaker, J.M. & Wieling, W. Circulatory
adaptation t o orthostatic stress in healthy IC-14year-old children investigated
in a general practice. Clin. Sci. 1991; 81, 51-8.
2. Imholz, B.P.M., Dambrink, J.H.A., Karemaker, J.M. & Wieling, W. Orthostatic
circulatory control in the elderly evaluated by non-invasive continuous blood
pressure measurement. Clin. Sci. 1990; 79; 72-9.
3. Wesseling, K.H. Finapres, continuous noninvasive finger arterial pressure
based on the method of Peak. In: Meyer-Sabellek, W., Anlauf, M., Gotzen, R.
& Steinfeld, L. eds. Blood pressure measurement. Darmstadt: Steinkopff
Verlag, 1990 161-72.
4. Imholz, B.P.M., Settels, 1.1. van den Meiracker, A.H., Wesseling, K.H. &
Wieling, W. Noninvasive beat-trjbeat finger blood pressure measurement
during orthostatic stress compared t o intra arterial pressure. Cardiovasc. Res.
1990; 24, 214221.
5. Wesseling, K.H., de Wit, B., Weber, J.A.P. & Smith, N.T. A simple device for
the continuous measurement of cardiac output. Adv. Cardiovasc. Phys. 1983;
5, 16-52.
6. Sprangers, R.L.H., Wesseling, K.H., Imholz, A.L.T., Imholz, B.P.M. & Wieling,
W. Initial blood pressure fall on stand up and exercise explained by changes
in total peripheral resistance. J.Appl. Physiol. 1991; 70, 523-30.
7. Imholz. B.P.M., Wieling. W., Langewouters, G.J. & van Montfrans, G.A.
Continuous finger arterial pressure: utility in the cardiovascular laboratory.
Clin. Autonom. Res. 1991; I, 43-53.
8. Friedman. D.B., Jensen, F.B.. Matzen, S. & Secher. N.H. Non-invasive blood
pressure monitoring during head-up tilt using the Penaz principle. Acta
Anaesthesiol. Scand. 1930; 34, 519-22.
9. Wesseling, K.H. FAST system user manual. Amsterdam: TNO-Biomedical
Instrumentation, 1991.
10. Smith, N.T., Wesseling, K.H., Weber, J.A.P. & de Wit, B. Preliminary
evaluation of a pulse contour cardiac output computer in man. Feasibility of
brachial or radial arterial pressures. Proc. San Diego Biomed. Symp. 1974; 13,
107-13.
II. Wesseling. K.H., Lasance, H.A.J., Ascoop, A. & Beneken, J.E.W. Transfer
functions and pulse contour stroke volume monitoring from central and
peripheral arterial pressure pulses in man. Excerpta Med. Int. Congr. Ser.
1976; 5, 36.
I55
12. Wesseling, K.H., Sprangers, R.L.H. & Wieling, W. Peripheral resistance
changes upon stand-up compared t o those t o tilt-up and onset t o cycling.
Implication of the cardiopulmonary reflex. In: Schmidt, T.H., Engel, B.T. &
Bliimchen, G., eds. In: Temporal variations of the cardiovascular system.
Berlin: Springer-Verlag, 1992 (In press).
13. Jansen, J.R.C., Wesseling, K.H., Settels, 1.1. & Schreuder, 1.1. Continuous
cardiac output monitoring by pulse contour during cardiac surgery. Eur.
Heart J.1990; II (Suppl. I),26-32.
14. Rowell, L.B. Human circulation regulation during physical stress. Oxford:
Oxford University Press, 1986.
15. Wieling, W. & Van Lieshout, 1.1. Maintenance of postural normotension in
humans. In: Low, P.A., ed. Evaluation and management of clinical autonomic
failure. Boston: Little Brown and Company, 1992: 69-77.
16. Brigden, W., Howarth, S. & Sharpey-Schafer, E.P. Postural changes in the
peripheral blood-flow of normal subjects with observations on vasovagal
fainting reactions as a result of tilting, the lordotic posture, pregnancy and
spinal anaesthesia. Clin. Sci. 1950 9, 79-91.
17. Eckberg, D.L. & Sleight, P. The human baroreflex. Oxford: Oxford University
Press, 1992: 61-77.
18. Smith, 1.1. & Porth, C.J.M. Age and the response t o orthostatic stress. In:
Smith, J.J.,ed. Circulatory response t o the upright posture. Boca Raton, F L
CRC Press, 1991: 121-39.
19. Karemaker, J.M., Wieling. W. & Dunning, A.J. Aging and the baroreflex.
Handb. Hypertens. 1988; 12, 2438.
20. Bennett, T. & Gardiner, S.M. Physiological aspects of the aging cardiovascular
system. 1. Cardiovasc. Pharmacol. 1988; I2 (Suppl. 8), SI-7.
21. Hajduczok, G., Chapleau, M.W., Johnson, S.L. & Abboud, F.M. Increase in
sympathetic activity with age. I. Role of impairment of arterial baroreflexes.
Am. J. Physiol. 1991; 260 (Heart Circ. Physiol., 29), HI 113-20.
22. Vanhoutte, P.M. Aging and vascular responsiveness. I. Cardiovasc. Pharmacol.
1988; I2 (Suppl. 8), SI 1-8.
23. Hajduczok, G., Chapleau, M.W. & Abboud, F.M. Increase in sympathetic
activity with age. II. Role of impairment of cardiopulmonary baroreflexes.
Am. J. Physiol. 1991; 260 (Heart Circ. Physiol. 29), H1121-7.
24. Cleroux, J,, Giannattasio, C., Bolla, G. et al. Decreased cardiopulmonary
reflexes with aging in normotensive humans. Am. 1. Physiol. 1989; 257 (Heart
Circ. Physiol. ZS), H961-B.
25. Van Brummelen, P., Biihler, F.R., Kiowski, W. & Amann, F.W. Age-related
decrease in cardiac and peripheral vascular responsiveness t o isoprenaline:
studies in normal subjects. Clin. Sci. 1981; 60,571-7.
26. Ebert, T.J., Hughes, C.V.. Tristani, F.E., Barney, ].A. & Smith, 1.1. Effect of age
and coronary heart disease on the circulatory responses t o graded lower body
negative pressure. Cardiovasc. Res. 1982; 16, 663-9.
27. London, G.M., Weirs, LA., Pannier, B.P., Laurent, S.L. & Safar, M.E. Tilt test
in essential hypertension. Differential responses in heart rate and vascular
resistance. Hypertension 1987; 10, 29-34.
28. Smith, J.J., Hughes, C.V., Ptacin, M.J., Barney, J.A., Tristani, F.E. & Ebert, T.J.
The effects of age on hemodynamic response to graded postural stress in
normal men. J. Gerontol. 1987; 42, 406.
29. Hainsworth, R. Non-invasive investigations of cardiovascular reflexes in
humans. Clin. Sci. 1990; 78, 43743.
30. Streeten, D.H.P. Pathogenesis of hyperadrenergic orthostatic hypotension.
Evidence of disordered venous innervation exclusively in the lower limbs.
1. Clin. Invest. 1990; 86, 1582-8.
31. Asmussen, E., Christensen, E.H. & Nielsen, M. The regulation of circulation in
different postures. Surgery 1940; 8, 604-16.
32. De Marker, H. Zur orthostatischen Sofortregulation. In: Denolin, H. &
Demanet, J.C., eds. Neural control of the cardiovascular system and
orthostatic regulation. Cardiology 1976; 61 (Suppl. I), 78-90.
33. Laurell, H. Die orthostatische arterielle Anamie, ein gewohnliches, aber oft
fehlgedeutes Krankheitsbild. Fortschr. Geb. Roentgenstr. 1936; 53, 501-19.
34. Abe, T. The small heart syndrome. Asiat. Med. J. 1990; 33, 295-302.
35. Smith, J.J., Barney, J.A., Porth, C.J., Groban, L., Stadnicka, A. & Ebert, T.J.
Transient hemodynamic responses to circulatory stress in normal male
subjects of different ages. Physiologist 1984; 27, 210.
36. Gascho, J.A., Fanelli, C. & Zelis, R. Aging reduces venous distensibility and
the venodilatory response t o nitroglycerin in normal subjects. Am. J. Cardiol.
1989; 63, 267-70.
37. Garnier. B. Blutdruckregulation, nervensystem und alter. Acta. Gerontol.
1972; 2, 387-96.