Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
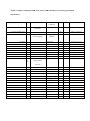
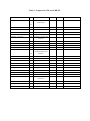
Reproducibility and Clinical Validation of Tissue tracking methodology CMR-based strain methodologies in clinical validation of tissue tracking: CMR based techniques were first allowing the assessment of regional myocardial deformation noninvasively starting with myocardial tagging (1) which creates non-invasive markers in the myocardium. Tag lines obscure some of the endocardial borders, reduce temporal resolution and increase scan time. These reasons, in addition with the time consuming post-processing have prohibited tagging from becoming a mainstream clinical application. Most postprocessing issues have been overcome by the Harmonic Phase (HARP) algorithm, using the first harmonic peaks of the image’s k-space which has been validated intensively (2). Tagging has been mostly used to assess circumferential strains and cardiac rotation and twist. Alternative techniques to tagging such as DENSE (3) and SENC (4), both of which, however, have only been used by a limited number of centers. Speckle-Tracking Echocardiography: Both, 2D-STE and 3D-STE have been validated against sonomicrometry and CMR tagging (Table 2) (5–8). Overall, GLS compares best to CMR tagging, with a small bias and reasonably small limits of agreement. CMR Feature Tracking: GLS as well as basal, mid and apical GCS showed the best intraobserver reproducibility, with a coefficient of variation (CV) ranging from 3% to 17%. GLS performed better in the LV (CV ranging from 12% to 18%) than in the RV (CV 29% to 43%), but clearly worse than for GCS, although they have similar absolute values. Radial strain showed CVs ranging from 23% to 31%, with slightly better reproducibility, when measured from short axis slices. Similar trends are observed for the inter observer variability of global strain values (9, 10). Morton et al. reported inter study variability (11) in 3 repeated exams in one day performed in the morning (9:00 am) immediately after the first scan and in the afternoon (2:00 pm). Similar findings were obtained with GCS performing best (CV: 20%) and RV GLS worst (CV: 30%). Segmental strain values may show large variability, which may be clinically unacceptable (CVs up to 63%). Magnetic field strength, however, does not influence reproducibility (10). CMR-FT has been validated against the traditional CMR strain techniques (Table 4). Overall GCS compare best to CMR tagging with HARP post-processing, e.g. (12), with high correlation and low limits of agreement. CMR-FT has been compared to SENC for global longitudinal function (13), with small bias and fair limits of agreement for both RV and LV. Direct Comparison of 2D-STE and CMR-FT: Comparisons of STE with CMR-FT have shown promising results in correlation and inter-modality variation across multiple studies looking at strain measurements (Table 3). Global longitudinal and circumferential strain showed the best agreement between STE and CMR-FT, except in the cases where geometry is altered, as in hypertrophic cardiomyopathy, where circumferential strain was less comparable. This could be attributed to different endocardial border definition in echocardiography and CMR. Radial strain between techniques is not comparable. These inter-modality comparisons follow the separate variability of the different components, and variability is unacceptably large for radial strain. References 1. Zerhouni EA, Parish DM, Rogers WJ, Yang A, Shapiro EP. Human heart: tagging with MR imaging--a method for noninvasive assessment of myocardial motion. Radiology 1988;169:59–63. 2. Osman NF, McVeigh ER, Prince JL. Imaging heart motion using harmonic phase MRI. IEEE Trans. Med. Imaging 2000;19:186–202. 3. Aletras AH, Ding S, Balaban RS, Wen H. DENSE: displacement encoding with stimulated echoes in cardiac functional MRI. J. Magn. Reson. 1999;137:247–252. 4. Osman NF, Sampath S, Atalar E, Prince JL. Imaging longitudinal cardiac strain on shortaxis images using strain-encoded MRI. Magn. Reson. Med. 2001;46:324–334. 5. Amundsen BH, Helle-Valle T, Edvardsen T, et al. Noninvasive myocardial strain measurement by speckle tracking echocardiography: Validation against sonomicrometry and tagged magnetic resonance imaging. J. Am. Coll. Cardiol. 2006;47:789–793. 6. Bansal M, Cho GY, Chan J, Leano R, Haluska BA, Marwick TH. Feasibility and Accuracy of Different Techniques of Two-Dimensional Speckle Based Strain and Validation With Harmonic Phase Magnetic Resonance Imaging. J. Am. Soc. Echocardiogr. 2008;21:1318– 1325. 7. Seo Y, Ishizu T, Enomoto Y, et al. Validation of 3-dimensional speckle tracking imaging to quantify Regional Myocardial Deformation. Circ. Cardiovasc. Imaging 2009;2:451–459. 8. Kaku K, Takeuchi M, Tsang W, et al. Age-related normal range of left ventricular strain and torsion using three-dimensional speckle-tracking echocardiography. J. Am. Soc. Echocardiogr. 2014;27:55–64. 9. Augustine D, Lewandowski a J, Lazdam M, et al. Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: comparison with tagging and relevance of gender. J Cardiovasc Magn Reson 2013;15:8. 10. Schuster A, Morton G, Hussain ST, et al. The intra-observer reproducibility of cardiovascular magnetic resonance myocardial feature tracking strain assessment is independent of field strength. Eur. J. Radiol. 2013;82:296–301. 11. Morton G, Schuster A, Jogiya R, Kutty S, Beerbaum P, Nagel E. Inter-study reproducibility of cardiovascular magnetic resonance myocardial feature tracking. J. Cardiovasc. Magn. Reson. 2012;14:43. 12. Hor KN, Gottliebson WM, Carson C, et al. Comparison of Magnetic Resonance Feature Tracking for Strain Calculation With Harmonic Phase Imaging Analysis. JACC Cardiovasc. Imaging 2010;3:144–151. 13. Ohyama Y, Ambale-Venkatesh B, Chamera E, et al. Comparison of strain measurement from multimodality tissue tracking with strain-encoding MRI and harmonic phase MRI in pulmonary hypertension. Int. J. Cardiol. 2015;182:342–348. 14. Altiok E, Neizel M, Tiemann S, et al. Quantitative analysis of endocardial and epicardial left ventricular myocardial deformation-comparison of strain-encoded cardiac magnetic resonance imaging with two-dimensional speckle-tracking echocardiography. J. Am. Soc. Echocardiogr. 2012;25:1179–1188. 15. Kleijn SA, Brouwer WP, Aly MFA, et al. Comparison between three-dimensional speckle-tracking echocardiography and cardiac magnetic resonance imaging for quantification of left ventricular volumes and function. Eur. Heart J. Cardiovasc. Imaging 2012;13:834–839. 16. Helle-Valle T, Remme EW, Lyseggen E, et al. Clinical assessment of left ventricular rotation and strain: a novel approach for quantification of function in infarcted myocardium and its border zones. Am. J. Physiol. Heart Circ. Physiol. 2009;297:H257–67. 17. Goffinet C, Chenot F, Robert A, et al. Assessment of subendocardial vs. subepicardial left ventricular rotation and twist using two-dimensional speckle tracking echocardiography: comparison with tagged cardiac magnetic resonance. Eur. Heart J. 2009;30:608–617. Table 1: Studies comparing STE to CMR techniques for assessing left ventricular deformation. First author, year (refrence) Correlation coefficient Bias (LOA) Endocardial segmental LS 0.53 0.8% (17.9 to -16.4) Endocardial segmental CS 0.64 7.3% (24.7 to -10.0) Epicardial segmental LS 0.61 -1.8% (9.7 to -13.0) Epicardial segmental CS 0.36 0.2% (14.4 to -14.0) 0.8 10% (13.2 to 6.7) regional rotation 0.71 0.6% (3.6 to -2.4) regional strain 0.87 1.5% (5.7 to -2.7) GLS 0.5 - GRS 0.59 - GCS 0.63 - Endocardial twist - 0.09°(−3.1 to 3.3) mid-ventricular twist - 0.78° (−3.2 to 4.8) Epicardial twist - 0.42°(−4.7 to 5.5) Peak twist velocity - −7.9 °/s (−36.0 to 20.0) Altiok 2012(14) Kleijn 2012 (15) n Patient characteristics Methods compared 44 Patients referred for ischemia assessment 2D-STE vs. CMR-tagging 45 Healthy subjects 3D-STE vs. CMR-tagging GCS Helle-Valle 2009 (16) 38 Bansal 2008 (6) 30 Goffinet 2009 (17) 53 15 healthy and 23 re-perfused MI patients Ischemic heart disease 43 heart failure and 10 controls 2D-STE vs. CMR-tagging 2D-STE vs. CMR-tagging 2D-STE vs. CMR-tagging Table 2: Studies comparing CMR-FT to other CMR techniques for assessing myocardial deformation. First author, year (reference) Hor 2010 (3) n Patient characteristics Methods Compared 233 Duchenne Muscular Dystrophy Tagging/HARP LV-GCS (medial slice) Moody 2014 (104) 10 Dilated Cardiomyopathy LV-GLS Ohyama 2015 (23) 30 + 15 Bias (LOA) .89 -0.4% (-3.6 to 2.9) .77 .73 .75 .80 .70 .76 .73 .61 1.5% (-4.3 to 7.3) 2.1% (-4.1 to 8.3) 1.4% (-4.6 to 7.4) .9% (-4.5 to 6.3) 2.5% (-4.5 to 9.5) 3.3% (-3.9 to 10.5) 2.4% (-4.6 to 9.4) 1.6% (-6.0 to 9.2) .60 .57 .72 -2.8% (-9.6 to 4.0) 2.7 (-1.8 to 7.3) 0.4% (-5.9 to 606) Pulmonary Hypertension + Controls LV-GCS LV-GLS RV-GLS Singh, 2014 (105) COV Tagging/ CIMTag whole wall Sub epi Mid Sub endo Whole wall Sub epi Mid Sub endo LV-GCS R Tagging-HARP SENC SENC 18 LV-GCS LV-GLS Augustine, 2013 (21) 8 10 20 Tagging (1.5T) 26 LV-GCS LV-GRS 3.9% (-3.92 to 11.8) 3.6% (-2.99 to 10.22) - - .7% (-6.0 to 4.0) -1% (-16 to 3) 11% (-1 to 23) .35 no - -3.7% (-9.6 to 2.2) -30.5% (-84.4 to 23.4) Tagging (3T) Normal subjects Tagging/HARP LV-GCS LV-GLS LV-GRS Lu, 2013 (106) 21 17 Anthracycline Tagging/HARP Table 3: Comparison STE and CMR-FT. First author, year (reference) n Patient characteristics R COV Bias (LOA) Kempny, 2012 (88) 28 + 25 Tetralogy of Fallot and Controls LV-GLS - 15.8% -2% (-9 to 5) LV-GCS - 17.0% 1% (-10 to 12) LV-GRS - 69.0% 15% (-29 to 58) RV-GLS - 16.6% -1.5% (-9 to 6.5) - - -1.38% (-10.37 to 7.62) 0.77% (-4.34 to 5.88) -10.88% (-54.47 to 32.71) 0.04% (-8.47 to 8.57) - 14.4% 19.4% -0.82% (-8 to 6.5) 3.1% (-9.8 to 16.1) 0.81 0.87 - 1.9% (9.9 to -6.0) 1.5% (9.7 to -6.7) 0.87 0.61 0.79 - -6.0% (0.2 to -12.2) -10.1% (22.5 to -42.8) -0.7% (7.9 to -9.3) 0.68 - 0.7% (7.7 to -6.3) 0.93 - -0.3 ms (83.3 to -83.8) Padiyath, 2013 (103) 20 Tetralogy of Fallot and Controls LV-GLS LV-GCS LV-GRS RV-GLS Orwat 2014 (107) 20 + 20 Hypertrophic Cardiomyopathy and Controls LV-GLS LV-GCS Onishi, 2015 (108) 71 Heart failure LV-GLS LV-GCR Kaku, 2014 (16) 19 Normal subjects LV-GLS LV-GRS LV-GCS Makoto, 2014 (109) Constriction and restriction LV-GLS Onishi, 2013 (110) Radial dyssynchrony 72 Dyssynchrony