Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
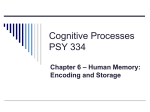
604 Subthreshold Stimulation of Purkinje Fibers Interrupts Ventricular Tachycardia in Intact Hearts Experimental Study With Voltage-Sensitive Dyes and Imaging Techniques Guy Salama, Anthony Kanai, Igor R. Efimov Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Abstract The effects of subthreshold stimulation (STS) delivered during right atrial pacing and ventricular tachycardia (VT) were investigated in Langendorff-perfused guinea pig hearts. The hearts were stained with a voltage-sensitive dye (RH 421) to map the propagation of optical action potentials. Sustained VT was reliably induced by 5-second trains (cycle length [CL], 25 to 50 milliseconds; duration, 0.5 to 10 milliseconds; and voltage, 2x threshold voltage) of impulses (n=12 hearts) or a single premature beat (n=6). The location of extrastimuli was not critical to the induction of VT, but the diameter of the heart had to be .14.5 mm. During VT, heart rate increased from 200 to 600 beats per minute; action potential durations decreased from 112 to 175 milliseconds to 60 to 105 milliseconds, with no diastolic interval. Activation on the epicardium spread anisotropically, but VT decreased the "apparent" maximum conduction velocity (Om.) by 68% and altered the orientation of the major axis from beat to beat. Activation patterns and Omax measured during VT were similar to patterns recorded during direct pacing of the ventricle and indicated that Purkinje fibers no longer propelled ventricular excitation. STS (CL, 25 to 50 milliseconds; duration, 0.5 to 25 milliseconds; and voltage, 0.5 x to 0.8 x threshold; trains of 2.0 to 2.5 seconds) interrupted VT when applied to Purkinje fibers lining the endocardium (n=6) but failed to interrupt VT when applied to the epicardium (n=8). In atrial pacing, STS delivered to the endocardium increased Omax from 2.44+0.32 (mean±SEM) to 3.63±0.21 m/s in a local region surrounding the first activation sites (n=4). Alternatively, VT could be terminated by reducing Omax (=55%) with procainamide (10 gmol/L) (n=6). STS terminates VT by synchronizing ventricular excitation most likely by increasing local conduction and/or improving the coupling between Purkinje and ventricular cells. (Circ Res. 1994;74:604-619.) Key Words * subthreshold stimulation * ventricular tachycardia * action potentials * cycle length * apparent maximum conduction velocity * anisotropic propagation . reentry * voltage-sensitive dyes n the clinical setting, human ventricular tachycardia (VT) can be terminated by subthreshold stimula- vation by mapping with multiple surface electrodes, STS (10 to 100 Hz) terminated VTs most effectively when applied at the "early" activation site of the tachycardia on the endocardium.'0 Several mechanisms have been proposed to explain the termination of VT and/or VF by STS. The proposed mechanisms did not clearly distinguish between VT and VF and were based on the interruption of reentry pathways by reducing the size of the excitable gap. For instance, STS may interrupt reentry by (1) prolonging repolarization (ie, action potential [AP] duration) and causing a local increase in the refractory period,'1 (2) initiating an early partial depolarization, resulting in supernormal conduction velocity at the stimulation site,12 and/or (3) inducing a local release of catecholamine, which would enhance local conduction velocity.10 Difficulties in understanding the mechanism(s) whereby STS interrupts VT are compounded by the lack of a common definition of VT, the different physiological states of the hearts in various studies, and the different methods used to initiate VTs. Thus, the interruption of VT by STS may well depend on the nature of the VT. In turn, the most common cause of VT is reentry, and at least three mechanisms have been proposed to account for reentry. (1) An activation wave front could propagate repeatedly around a cut (anatomic block) made in the center of the atrial muscle.'3 Two tion (STS) applied with catheter electrodes inserted in the left ventricle through the aorta. These findings are potentially important in the development of effective low-energy defibrillation techniques. However, the mechanism(s) whereby STS terminates VT and the precise location of the electrodes applying STS have yet to be elucidated. Stimulation with low-level noncapturing impulses was shown to block normal heart beats, first in amphibian' and then in canine2 and human3 ventricular muscles. STSs of different frequencies were subsequently tested in attempts to interrupt arrhythmias. High-frequency (333 Hz) STS blocked excitation waves elicited by premature extrastimuli in canine ventricles.4 Low-frequency (13.3 to 20 Hz) STS was equally effective at interrupting VT in the clinical setting,5 atrial tachycardia,6 and triggered activity7'8 and in blocking the induction of ventricular fibrillation (VF).9 In studies of actiFrom the University of Pittsburgh School of Medicine, Department of Physiology, Pittsburgh, Pa. Previously published as a preliminary report in abstract form (Circulation. 1990;82[suppl III]:III-98). Correspondence to Dr Guy Salama, Department of Cell Biology and Physiology, University of Pittsburgh, W1442 Biomedical Science Tower, Pittsburgh, PA 15261. Salama et al Subthreshold Stimulation Interrupts VT Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 factors were necessary for repeated reentry or circus movement around the loop: block and slowed conduction. The anatomic barrier provided a track around which a propagating wave could loop. Slowed conduction made it possible for the tissue to repolarize and recover from refractoriness before the return of the next activation wave front. The time interval between the repolarization and the arrival of the next activation wave front was called the excitable gap. Factors that increase conduction velocity or the refractory period of the muscle decrease the excitable gap and thus increase the likelihood of extinguishing the wave front. The anatomic block could be caused by myocardial infarction or ischemia, whereas slow conduction may result from a rise in resting membrane potential. In circus movement, activation wave fronts propagate repeatedly around an anatomic barrier from beat to beat, resulting in monomorphic electrogram signals. (2) Anisotropic reentry is based on the heterogeneous propagation of APs, with fast and slow conduction velocities along directions parallel and transverse to the longitudinal axis of ventricular cells. This form of reentry was demonstrated in hearts with infarcted left ventricles caused by a coronary occlusion. After a healing period, the infarction resulted in a two-dimensional thin layer of surviving tissue that sustained reentry loops through pathways of fast and slow conduction that aligned with the longitudinal and transverse axes of the underlying fibers.14,15 As for circus movement, anisotropic reentry requires a pathological injury and results in monomorphic electrogram signals. (3) In the absence of hypoxia or ischemia (ie, in "healthy" heart muscle), leading circle tachycardia was first demonstrated in rabbit atrial muscle.'6 The difference between leading circle and circus movement is the lack of an excitable gap; ie, the instant a region of tissue is repolarized, the next wave arrives to depolarize it. In leading-circle reentry, the refractory period set the wavelength of the circuit, and slight changes in refractoriness result in beat-to-beat alterations of activation patterns. As a result, electrogram signals appear polymorphic. The present report describes a nonhypoxic nonischemic model of VT in intact mammalian hearts and confirms that STS terminates VT under controlled experimental conditions. More important, activation patterns were mapped at high spatial and temporal resolution by use of voltage-sensitive dyes and imaging techniques to examine the mechanism(s) whereby STS terminates VT. On the basis of optical maps of normal and arrhythmic activation patterns, it appears that Purkinje fibers, which normally drive the excitation of the myocardium, become uncoupled and fail to synchronously drive the activation of the myocardium during VT. When STS is delivered to the endocardium, it appears that the coupling between the Purkinje network and the ventricular mass is reestablished, which interrupts such arrhythmias. Materials and Methods Preparation Guinea pigs (450 to 550 g, either sex) were anesthetized with an intraperitoneal injection of Nembutal (30 mg/kg), and their hearts were rapidly excised, cannulated at the aorta, and retrogradely perfused in a modified Langendorif apparatus. Input of perfusate at the aorta was controlled with a peristaltic 605 pump (Miniplus 2, Gilson, Middleton, Wis) and was connected to a graduated manometer to obtain a physiological mean aortic pressure of 80 mm Hg. The flow rate of the pump determined the flow of perfusate delivered to the coronary vessels and was adjusted for each heart to take into account differences in muscle mass. For each heart, the coronary flow rate was set at the beginning of each experiment to obtain 80 mm Hg for aortic pressure and was thereafter kept constant. A perfusion system with constant coronary flow rate ensured that oxygen delivery to the myocardium remained constant at all times, irrespective of the contractile state of the heart, coronary vascular tone, and arrhythmic conditions. Flow rates were in the range of 12 to 18 mL/min for the various hearts used in the present study. From the pressure-flow relation, changes in aortic pressure were used to detect possible changes in coronary resistance that might occur as a consequence of hypoxia, ischemia, or edema. Once the desired flow rate was determined, hearts selected for the present study had stable aortic pressures; if the pressure rose above 90 mm Hg, the data were discarded. The perfusate contained (mmol/L) NaCl 130, NaHCO3 12.5, MgSO4 1.2, KCl 4.75, glucose 50, and CaCl2 1.0, at 35-+±1°C. Solutions were continuously gassed with 95% 02/5% CO2 with the pH adjusted to 7.4 with NaHCO3. The present study describes data from a total of 30 animals (n=30). Activation patterns were measured during right atrial pacing and then during VT induced by a train of extrastimuli (n=12) or by a single precisely timed stimulus (n=6), for a subtotal of n= 18. The termination of VT by STS delivered at various locations on the heart was measured in the same 18 hearts. The interruption of VT by procainamide was repeated in another 6 hearts, and the effects of STS during right atrial pacing were assessed in another 6 hearts. In most hearts, the induction and termination of VT were repeated several times, typically five times. However, n refers to the number of hearts tested, not the incidence of VT induction and termination. The numbers of successful inductions and terminations of VT were considerably larger since the process was typically repeated four or five times with each heart. Guinea pigs weighing >450 g were used because their hearts were sufficiently large (circumference, >45 mm) to induce sustained VT. With smaller hearts, self-sustained VT could not be induced by single premature beats or trains of extraimpulses. The critical requirement that hearts have a minimum size to induce VT strongly suggested that reentry was the predominant mechanism and that this criterion defined the minimum length of the reentry pathways. Staining Procedure Hearts were stained with voltage-sensitive dye (RH 421, Molecular Probes, Eugene, Ore) by injecting 50 ,L of a 1 mmol/L stock solution of dye (dissolved in ethanol) into a 5-mL bubble trap placed above the aortic cannula. The dye was administered in a series of four bolus injections (12.5 ,L each) made over a 5- to 10-minute period, which maintained the dye concentration in the coronary vessels at :10 ,umol/L. Ethanol from one injection was washed out before the next injection such that the peak ethanol concentration in the coronary perfusate was <0.25%. Control injections of 250 ,L ethanol in the bubble trap produced a transient increase in ethanol concentration of up to 5% in the coronary perfusate. Such a bolus addition of ethanol had no adverse effects on left ventricular pressure or surface bipolar electrogram signals. Dye delivered through the coronary perfusate produced a deep and homogeneous staining of the myocardium, which made it possible to record optical action potentials for 2 to 4 hours without restaining the heart. For longer experiments, the hearts were effectively restained by following the same procedure. Stained hearts exhibited voltage-dependent fractional changes in fluorescence of -9.2±3% with signal-tonoise ratios of -250: 1. 606 Circulation Research Vol 74, No 4 April 1994 Placement of Stimulating Electrodes Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Bipolar stimulating electrodes were constructed by use of 250-,um-diameter Teflon-coated silver wires with a 50-gm interelectrode distance and exposed tips 0.5 mm in length. Three sets of bipolar Ag+/AgCl stimulating electrodes were positioned on the heart: (1) For atrial pacing, an electrode was glued to the right atrium with cyanoacrylate adhesive. (2) For endocardial pacing, a bipolar (250-,um-diameter Tefloncoated wires with a 50-gm interelectrode distance) electrode with a 2-mm hook was inserted transmurally across the free wall and then pulled back to remain implanted on the endocardium. The tips of the bipolar electrode were pushed against the endocardium without penetrating the wall to avoid direct current injection and excitation of deeper cells of the subendocardium. When the bipolar electrode was pulled ever so slightly into the wall, cells of the subendocardium and the midwall were directly excited; this excitation was readily distinguished because activation patterns that emerged on the epicardium were dramatically altered. Endocardial pacing most likely excited both Purkinje and adjacent myocardial cells. However, local excitation of nearby endocardial cells had little effect on activation sequences because of the dominant role of Purkinje fiber-driven excitation. (3) For epicardial pacing, an electrode was positioned at the center of the epicardium (ie, the center of the field of view of the photodiode array). The epicardial stimulating electrode could be readily repositioned to other locations within or outside the field of view of the array. After placing the stimulating electrode, hearts were mounted in a fluid-filled Plexiglas chamber designed to measure optical maps of AP propagation and to abate the curvature of the left ventricle and gross movements of vigorously contracting hearts. Details of the chamber, spatial homogeneity of temperature on the preparation, and control conditions regarding effects of the chamber on AP characteristics were previously reported.17 Pacing Protocols Hearts were paced at a basic drive cycle length (CL) of 300 milliseconds (=200 beats per minute) (S1), with a square-wave pulse of 5-millisecond duration, at twice the diastolic threshold (ie, 2x capture voltage). The rate was within the physiological range for guinea pigs (200 to 300 beats per minute at 41°C). Stable sinus (sinoatrial nodal) rhythm was mimicked by pacing the right atrium at 200 beats per minute, which overcame the intrinsic rate, at 35°C. During endocardial or epicardial pacing, a second electrode was placed on the endocardium or epicardium and was paced in synchrony with right atrial stimuli to prevent out-of-phase sinoatrial nodal beats from capturing the ventricles and interfering with activation patterns elicited by pacing the endocardium or epicardium. Refractory periods were measured using conventional premature beat techniques. Heart rate was controlled by synchronous pacing (S,) of the right atrium and the ventricle. The premature stimulus (S2) was delivered to the ventricle at the test site once for every 10 S, pulses. Starting with long S1-S2 intervals, S1-S2 was systematically decreased in 1-millisecond steps. S2 elicited an extra beat that propagated across the myocardium until S2 failed to elicit a propagated response. The refractory period was defined as the shortest S1-S2 interval at which a propagated response to S2 occurred. Both S, and S2 stimuli were 5-millisecond square pulses at 2 x diastolic threshold voltage. VT was induced by either a brief train of extrastimuli or a single premature beat. The most reliable procedure to induce an arrhythmia consisted of pacing the right atrium at a basal rate of S, (CL, 300 milliseconds; duration, 5 milliseconds; voltage, 2x threshold) and then turning on a burst of extrastimuli (S2) consisting of 5-second trains (CL, 25 to 50 milliseconds; duration, 0.5 to 10 milliseconds; and voltage, 2x threshold). S2 applied as a train of impulses was equally effective at eliciting an arrhythmia when delivered either on the endocardium or epicardium. To induce an arrhythmia with a single stimulus (S2), S, was synchronously applied on the right atrium and the left ventricle (either on the endocardium or epicardium), and the cycle length was set at 300 milliseconds. An extrastimulus (S2) was then applied after every eighth S, at progressively shorter (S1-S2) coupling intervals in 10-millisecond decrements until the induction of VT or the tissue became refractory to S2 stimuli. In most cases, VT was elicited when SI-S2 was 5'65% of the CL (ie, '-195 or z162.5 milliseconds for S, cycle lengths of 300 and 250 milliseconds, respectively). If the tissue was refractory to S2, the S1-S2 coupling interval was increased by 10 milliseconds longer than the refractory period and then decreased in 1-millisecond decrements to induce VT. When the extrastimulus was delivered on the endocardium, S2 rarely failed to initiate VT (<5% failure rate). When delivered on the epicardium, S2 failed to induce an arrhythmia in 15% to 20% of the hearts. During sustained VT, hearts were paced on the right atrium at Sl, and S2 was turned off. Electrode leads similar to those used to induce VT were used to deliver STSs at various sites on the endocardium or epicardium. To deliver STS, the settings on the stimulator were changed to deliver a 2- to 5-second train of impulses with a CL of 25 to 50 milliseconds, a duration of 0.5 to 25 milliseconds, and a voltage of 0.5 x to 0.8 x threshold. For hearts in our modified Langendorff apparatus, coronary flow rate remained constant before and after VT, and transient changes in vascular resistance were monitored through changes in perfusion pressure. The onset of VT occasionally caused a transient decrease in coronary resistance as monitored by a 10 to 20 mm Hg drop in perfusion pressure from a control of 80 mm Hg. The decrease in coronary resistance could be due to a metabolic vasodilation1819 or ventricular relaxation at the start of VT. Note that the term STS has become established in the literature and is used here for the sake of consistency. Subthreshold stimulation can be more precisely defined as the injection of current stimuli too low to elicit a regenerative response or AP propagation in normal resting ventricular muscle. An alternative nomenclature might be "subcapture" stimulation, because local current responses are elicited but fail to elicit the spread of APs.20 Two other terms are used in the STS literature: "low"- and "high"-frequency STS are used to refer to stimulation rates of .100 and >100 Hz, respectively, in line with the terminology used in previous reports. Optics Light from a 45-W tungsten-halogen lamp (PTI, Princeton, NJ) was collimated with a parabolic reflector and cooled with a heat filter. The excitation beam was controlled with an electronic shutter (Melles Griot, Irvine, Calif) to illuminate the heart only during optical recordings. The beam was passed through an interference filter (520+20 nm, Omega Optical, Brattleboro, Vt), reflected by a 45°C dichroic mirror (600-nm cutoff, Corion, Holliston, Mass), and focused on the stained heart with an epi-illumination lens (50 mm, 1:1.8 E series, Nikon, Garden City, NJ). Epifluorescence was collected, passed through a 645-nm cutoff filter (Schott Glass RG 645), and focused onto a 12x12-element photodiode array (Centronic, Newbury Park, Calif). Five diodes in each corner of the array were ignored such that optical signals were recorded from 124 of 144 diodes. The magnification of the image focused on the array was kept at x 1.5 such that each diode received light from a 1 x 1-mm area of tissue. The depth of field of the collecting lens restricted the fluorescence measurements to a layer of cells 144 ,um from the surface.21 The image focused on the array was reflected by a mirror onto a custommade graticule with the exact dimensions of the array (Graticules Ltd, Tonbridge, UK) located on a plane parafocal with the plane of the array. Precise focusing and aligning of the heart with respect to the array were accomplished by focusing Salama et al Subthreshold Stimulation Interrupts VT and aligning the image of the heart on the graticule. Details regarding the optical setup were previously reported.'7'21 Data Acquisition Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Photocurrents from each of 124 photodiodes were passed to current-to-voltage converters, AC-coupled with a 3-second time constant, and amplified x100; transient signal changes were digitized with eight-bit precision and stored via direct memory access in a DEC PDP 11-73 computer (Digital Equipment Corp, Woburn, Mass). Signals from each diode were sampled every 0.768 millisecond such that electrical activity from the heart was scanned at a rate of 1302 frames per second. A frame for the array consisted of sequential sampling of 128 analog signals, 124 optical signals, and 4 instrument channels. The instrument channels were used to simultaneously monitor the basal pacing impulse, atrial and ventricular bipolar electrograms, and extrastimuli. The instrument channels were sampled and digitized in synchrony with the 124 optical recordings. The sampling rate of the analogto-digital (A/D) converters was three times faster than the highest frequency component of APs (ie, more than twice the Nyquist frequency). As a result, the digitized data reproduced the analog signals without loss of information.22 The highfrequency cutoff of the analog circuits was 1 kHz, but the effective frequency cutoff was limited to the sampling rate of the A/D multiplexer, set at 1.3 kHz per channel for the present experiments. Fast analysis and display programs made it possible to view optical APs and activation patterns within 10 seconds after data acquisition. Selected data were transferred from RAM memory to RL02 hard disk and then to magnetic tape for archival storage. Data acquired under the RT-11 operating system (DEC) were transferred to a computer operating under UNIX MVME 147 CPU (Motorola, Phoenix, Ariz) to analyze the data in greater detail and generate Postscript files for hard-copy laser-printer displays. Signal Analysis Scans were taken at various times during the course of an experiment, and the maximum duration of a scan was 34 seconds at a rate of 1302 frames per second (limited by the RAM memory available on the DEC computer). To analyze an activation pattern for a particular cardiac beat, six optical APs (from the apex, middle, and base of the heart) were displayed on a monitor, and a cursor was used to select a window of data representing one heart beat. An algorithm calculated the first derivative of all 124 APs for the chosen beat. Maximum dF/dt (Vm..) was taken as the time point when most of the cells viewed by a given photodiode depolarized. The earliest activation event among the 124 APs in the same beat was assigned an activation time point of t=0.00. Activation at different diodes was measured relative to the first site to fire an AP; ie, each diode was assigned a relative activation time point with respect to the first site(s) to fire an AP. The activation time point of each AP was labeled with a "tick" mark that could be verified and corrected by the operator using an interactive program. Occasionally, a brief noise spike on an AP caused the algorithm to miscalculate and misplace the tick mark identifying the relative activation time point. An interactive program made it possible to correct the error by canceling the mark and recalculating the depolarization time point. The algorithm was highly reliable and rarely required correction by the investigator (.1% of activation events). The upstroke of optical APs was not distorted by movement artifacts from vigorously contracting hearts, because they preceded the onset of muscle shortening by 60 to 100 milliseconds. As a result, motion artifacts did not pose a problem for the detection of activation times and activation patterns. The repolarization time point of each AP was defined as (d2F/ dt2)m,x of the AP downstroke, and the duration was the time interval between activation and repolarization time points.23 607 Patterns of AP propagation were displayed as isochronal maps based on the relative activation times of the 124 APs. The first to last isochrones depicted the earliest to the latest regions of tissue to activate, and the time delay between isochrones was in units of milliseconds. Each diode was depicted as a box in a symbolic map of the array that was filled with the appropriate AP tracing detected by that diode and its relative activation time. The rise times of optical AP upstrokes were taken as the time difference between points at 10% and 90% of the AP amplitude. Detailed maps of fiber orientation were previously measured as a function of depth in guinea pig right and left ventricles.21 Our measurements of fiber orientations at different depths of guinea pig free ventricular walls were in excellent agreement with detailed histological studies in dog hearts.24 Histological analyses of fiber orientations were also superimposed on optical maps of activation and repolarization from the same tissue. Each heart was paced at different sites to compare activation patterns and time delays produced by the different stimulation protocols. Conduction velocities were measured from the activation time delays along the epicardium, and the mean±SEM conduction velocity was calculated for perfused hearts paced under the same stimulation protocol. Mean±SEM conduction velocities were determined and compared from the same hearts paced at different sites. Conduction Velocities A completely automated analysis of propagation velocity was developed that did not require us to identify directions of fast and slow propagation and to select diode pairs to calculate propagation velocities. A computer algorithm calculated the average activation (or repolarization) velocities from the vectorial average of 124 local velocity vectors oriented between 0 and Ir radians. Average velocities along different directions were calculated from the projection of the average vector onto a set of 36 orientations from 00 to 1800, using an averaging algorithm with a bin width of 5°. The maximum and minimum scalar amplitudes of vectors oriented from 00 to 1800 represented the fastest and slowest conduction velocities, respectively, in the tissue. Computer-automated calculations of maximum and minimum conduction velocities (0.. and Oi, respectively) (based on the 124 local velocity vectors) were compared with manual conventional measurements of conduction velocity (based on the selection of 20 diode pairs along directions of fast and slow propagation). The values of Omax. and Omin reported in these studies were obtained with the automated algorithm, since it represented a more thorough analysis of all the AP recordings. In the case of multiple activation sites, the automated analysis underestimated conduction velocities because the averaging routines canceled vectors of similar magnitudes but opposite directions. Multiple breakthrough sites occurred rarely during atrial pacing and more often during VT. Modifications of the algorithm avoided subtraction of vectors oriented in opposite directions, as occurs during colliding wave fronts, and made it possible to calculate average propagation velocities even in the presence of multiple activation (or repolarization) breakthrough sites. The following algorithm was used to determine distribution of the local conduction velocity vectors. First, a gradient vector for activation (GA) was calculated for each diode. The horizontal component of the gradient vector (i) was calculated from the activation time delays between a diode and its two adjacent neighbors (for boundary diodes, only one neighbor was taken into account) in the same row of diodes divided by the distance 2d. The vertical component (j) was calculated from the time delays between the diode and its adjacent neighbors on the same column divided by 2d. The distance d represented the distance (center to center) between tissue patches viewed by the diodes (see Fig 1; interdiode distance d equals 1.5 mm divided by the optical magnification). In the 608 Circulation Research Vol 74, No 4 April 1994 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 FIG 1. The relative activation and repolarization times were determined for each diode as described in "Materials and Methods." For a diode located at position i,j, a local gradient vector of activation (GA) was determined from the averaged activation time delay (t) between that diode and its nearest neighbors divided by the distance (d) between the two recording sites: GA=Gx+Gy, where Gx=1/2[(ti+1,i-ti,)/dd+(ti, -ti-,,i)/ and d]i= (t+1,j-ti ,1j)I2di, GY= 1/2[(t,j+1 -t,j1)/d+ (t,j-t,j 1)/d]j =(ti,j+1-ti,j 1)2dj, where i and j are the horizontal and vertical components of the gradient vector, respectively. The local velocity vector U was defined as a vector with the same orientation in space and magnitude that is the reciprocal of IGAI: IU-=1/IGAI=1/(GX2+Gy2)1/2. The direction of GA is represented by a unitary vector n-=iGx/(Gx2+Gy2) 2+jG /(Gx2+G12)1/2 For each diode, the local conduction velocity yector (UA) was calculated as follows: UA= UJC1 =iGx/(GX2+Gy2) +jGy/(GX2+GY2) present experiments, distance d=1 mm for optical magnification of 1.5. The local gradient vector was the resultant of the vertical and horizontal components: GA=GX+GY. These 124 gradient vectors point in the direction of greatest change in activation and have units of time per unit distance of myocardium; ie, they are normal to the local propagating wave front. Local velocity vectors (units of meters per second) were defined as vectors with orientations and magnitudes equal to the reciprocal absolute values of the gradient vectors (see Fig 1). Results Patterns of Activation Under Various Stimulation Protocols Fig 2 illustrates a map of 124 simultaneously recorded APs during a single cardiac beat. The optical response from each diode is drawn in its appropriate location in a symbolic map of the array. Each diode is identified by a number on the upper left corner of the box that defines its location. In the present experiments, the array viewed 12 x 12-mm regions of left epicardium such that the base, apex, and anterior and posterior regions were respectively aligned with the top, bottom, left, and right edges of the array. The optical tracings were analyzed to determine the first site(s) to fire an AP(s) and were assigned an activation time point (t=0.0). All other sites fired at later time points, and for each diode, the relative activation time delays were recorded above the AP tracing (in milliseconds). From the relative activation time delays, isochronal maps were plotted to better visualize activation patterns. During right atrial pacing, activation began on the anterior and spread rapidly to the posterior region of the epicardium (Fig 3A). In physiological sinus rhythm and in atrial pacing, the specialized conduction system of the heart elicited the synchronous excitation of the ventricular free walls. As a result, the first sites to activate represented "breakthrough" sites emerging from the endocardium to epicardium. The pattern propagated rapidly across the surface and was highly reproducible whenever Purkinje fibers drove the excitation of the tissue. For instance, when Purkinje fibers were directly paced with an electrode paced on the endocardium, activation patterns were identical (in orientation and activation time) to patterns observed during sinus rhythm or right atrial pacing (Fig 3B). Whenever Purkinje fibers triggered ventricular excitation, activation patterns that emerged on the epicardium represented the breakthrough of excitation from the endocardium to the epicardium. In atrial and subendocardial pacing (Fig 3A and 3B), the "apparent" Omax was 2.64+0.24 m/s (n= 18), which was attributed to the rapid conduction velocity of Purkinje fibers.21 In contrast, direct stimulation of the epicardium produced elliptical patterns with Omax (0.84±0.15 m/s) and 0m.i (0.44±0.06 m/s) (n=6) oriented parallel to the longitudinal and transverse axes of epicardial fibers (Fig 3C). Conduction velocities during epicardial pacing represented velocities intrinsic to the myocardial tissue, in the absence of Purkinje fiber-driven activation. To verify this interpretation, the endocardial pacing electrode that produced rapid Purkinje fiber-dependent activation (Fig 3B) was displaced to the subendocardium to avoid direct stimulation of the Purkinje fibers. In subendocardial pacing, activation on the epicardium propagated with slow velocities compared with atrial pacing, and the major isochronal axis of the ellipse was rotated by 900 (Fig 3C). Activation driven by the specialized conduction system was dramatically different from activation obtained by direct electrical stimulation of the myocardium in both orientation and velocity, and these patterns were highly reproducible from heart to heart (n = 18). Unless stimulated directly on the epicardium, conduction velocities measured from activation time delays on the epicardium represented apparent conduction velocities, because activation waves could propagate transmurally, ie, in a direction perpendicular to the epicardial surface. Depolarization times for left ventricles under atrial pacing or sinus rhythm were 8±4 milliseconds (mean±SD, n= 18). The activation sequence always started from the anterior and spread to the posterior edge of the ventricles. During pacing at the center of epicardia, activation spread anisotropically from the stimulus site, resulting in isochronal lines that formed ellipses with major axes oriented at 135+±3. The orientation of the major axis was parallel to the longitudinal axis of epicardial fibers.21 During epicardial pacing at the center of left ventricles, activation times across the ventricles were 20±5 milliseconds (mean±SD, n=18), which was considerably slower compared with activation times (8±4 milliseconds) measured during sinus rhythm. These differences in activation time delays were compiled from 18 guinea pig hearts. For each heart, there was a consistent and significant increase (3.0±+ 0.4 times [mean±+SD], n=18) in activation time delay during epicardial pacing compared with Purkinje fiber-driven excitation of the ventricles. Induction and Termination of Sustained VT by Burst Stimulation Fig 4 illustrates the induction and termination of VT using a train of extrastimuli followed by a train of STS. The top panel shows five tracings of continuous (34- -ws- Salama et al Subthreshold Stimulation Interrupts VT . .1 c A . -, .9 _8* m0 A - zD 25 MbiI' K kS .. O 1 a . ,- -1 9 =: lt C4 a4 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 10 ._ ,Q_ ( .t Mi 11 *n,RI, * M A Wb A s .* ...-I-1 ... a 9 1 -. a mx-.1 XZ ;t.i '] ..i1 O2 * -I C4 00 ,n:. m 0o9 t5 OR ... 1 .... . W 5 5 '"'!n .1 -1 bli lf, n .1 XN g8 -I1 0 .. 'i 1 -I ~ 0 Pa LCL 'S in F- W 0 a A -13 ~ oo .n O q" og 0 'I C) ..1 1 . a . --- . - W 0 E 0 c: 'c 609 610 Circulation Research Vol 74, No 4 April 1994 BASE N N I ', cc cc 9m cc W 1 _ < (`, 1 1 Alm C. Epicardium pacing A. Right Atrial Stimulation i 0 f t XF i1 ;..m 1 2e 4:0 71 4l A 1 7 L.1 1Ill- Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 1 B. Endocardium pacing \,i ( / D. Subendocardium pacing FIG 3. Activation patterns recorded under different stimulation protocols. A, The heart was paced (cycle length [CL], 300 milliseconds) with an electrode on the right atrium to control heart rate and mimic activation patterns during physiological sinus rhythm. B, The left endocardium was paced (CL, 300 milliseconds) in synchrony with the right atrium. Impulses from the right atrium encountered refractory tissue because of atrioventricular nodal delay such that the activation pattern was initiated by the stimulation of the endocardium. In panels A and B, activation emerged at the center and anterior region of the epicardium (solid dot) and propagated with similar orientation and apparent conduction velocity. C, The epicardium was paced (CL, 300 milliseconds) in synchrony with the right atrium, and the activation pattern was initiated by the stimulus site (solid dot) on the epicardium. Activation spreads according to the intrinsic propagation velocity and orientation (1350) of the longitudinal axis of epicardial fibers.21 D, The endocardial electrode in panel B was displaced in the ventricular wall to avoid contact with Purkinje fibers lining the endocardium. Activation was initiated from a stimulus site on the endocardium, and the first site to emerge on the epicardium (solid dot) was shifted slightly compared with panel B. A subendocardial site received the initial excitation and propagated on the same layer of ventricle and transmurally according to the fiber orientations as a function of depth. The pattern that emerged on the epicardium (panel D) was rotated by 700 to 900 compared with panel C because of the transmural clockwise rotation of ventricular fibers from endocardium to epicardium. Activation began at solid dot and spread according to isochronal line (shown 1 millisecond apart). second) recordings of cardiac electrical activity. The top three tracings (Nos. 15, 49, and 94) monitored optical signals from three diodes on the array corresponding to 3 (of 124) separate sites on the heart. These diodes were arbitrarily selected to represent APs from the base (No. 15), middle (No. 49), and apex (No. 94) of the left epicardium. These numbers referred to our diodenumbering scheme that identified the location of the diode on the array (as shown in Fig 2) and thus the area of tissue monitored. The tracings labeled IC1 and 1C3 (indicating instrument channel 1 and instrument channel 3, respectively) monitored bipolar electrograms located on the left ventricle and atrium, respectively. The heart was paced on the right atrium at a constant CL of 300 milliseconds, which mimicked stable physiological sinus rhythm activation of the heart. Fig 4 shows VT induced by extrastimuli (left "time bar" between IC1 and 1C3) consisting of a 5-second burst of stimuli (CL, 50 milliseconds; duration, 10 milliseconds; and voltage, 2x threshold) delivered on the endocardium. To visualize APs before and during the induction of VT, a 3-second interval of the five tracings was displayed at a faster sweep speed (Fig 4, lower left tracings). The first two APs in tracings 15, 49, and 94 exhibited the expected upstroke plateau and repolarization phases of guinea pig ventricular APs. The last set of APs that fired under right atrial stimulation (solid arrow, ASt) received an extrastimulus that produced a transitional premature beat (solid arrow, TRANS) immediately after the repolarization phase of the previous APs. The subsequent six cycles of depolarization (solid arrows, 1 to 6) depicted the onset of VT. Each cycle of VT was analyzed to map the spread of depolarization in greater detail in Fig 5. VT was monitored for 25 seconds and then was terminated by a 2.5-second train of STS (CL, 50 milliseconds; duration, 10 milliseconds; and voltage, 0.8 x threshold; right "time bar") delivered on the endocardium. To visualize the electrical events during sustained VT and its termination during STS, the tracings were displayed at a faster sweep speed (Fig 4, lower right tracings). The solid arrows (below channel 94, right tracings) labeled the cycles of depolarization from 6 to 1, which occurred just before the interruption of VT and recovery back to atrial rhythm. Activation patterns in cycles 6 to 1 were analyzed and displayed as isochronal maps in Fig 6. During VT, AP upstroke velocities and amplitudes decreased, and AP durations decreased from 112 to 175 milliseconds to 60 to 105 milliseconds (n=6). Electrical activity recorded at all 124 sites appeared as waves of depolarization, and the moment a region of tissue repolarized, the next wave arrived to depolarize it with no diastolic interval (n=6). Each activation sequence at a particular site was associated with a set of depolarizing waves recorded at the other 123 sites, such that the spread of activation could be identified and mapped for each cycle of VT. For instance, the 110th (Fig 4, solid arrow labeled 110 under tracing 94) of 265 cycles of VT was analyzed and displayed in Fig 6, to illustrate the spread of activation during VT. Fig 5 illustrates activation patterns during the induction of VT. Control activation patterns were measured during right atrial pacing (Fig SA), the first transitional beat at the onset of a train of extrastimulation (Fig SB), and the first to the sixth beat of VT (Fig SC through 5H). These isochronal maps record the sequence of consecutive cardiac cycles labeled in Fig 4 by solid arrows (bottom left). The last normal atrial beat (Fig SA) before VT exhibited the standard activation pattern measured when the specialized conduction system (ie, Purkinje fibers) drives the excitation of the ventricles, as in Fig 3A and 3B. The transitional beat propagated more slowly and at a different orientation compared with the last atrial pacing beat (Fig SB). After the induction of VT, heart rate increased from 200 to ;600 beats per minute, and the apparent Omax decreased by two thirds compared with normal sinus rhythm. The decrease in apparent conduction velocity presumably _,. Salama et al Subthreshold Stimulation Interrupts VT -. . '..-(., 2Z..ao ii s.- .. ... . .4(O Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 - t ) A 17 I .5 I J *..V .1' ...I1. *.. '..', * *jj%. . 9, F5.. *1 . 1. 'It (7 L) G , _; ._ .- *, A.. * ,.} .,' r _o } 1. _- a .. _. .5,. . . g1 ,_ ,>,, 'K _ :a" _,_, I *_,. 4/ .s _. .4.. I _.-.t I _t _^_ K _, ,_a; 6'4-C- C _vo:8_ _*-L ,,_ 0% .7 * -K, _ 4<.. . _ @ 4, *^:4, _ .+, _S.; iL; 4' II; --***:;1 , _;,4.. : _-.K :L _S.t i ,>@- J C.) 00 611 612 Circulation Research Vol 74, No 4 April 1994 .ll cl: 0 cc UJ A 0 ,..v ', --N ', ;z.- -bN > ',11) 11 -Z 0) _: _ _ 0 ZI^ at .0~ oo- _ 01 01 _ ;=-om _ Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 A. Atrial Stimulation C. VT beat #1 E. VT beat #3 G. VT beat #5 B. Transitional beat D. VT beat #2 F. VT beat #4 H. VT beat #6 FIG 5. Activation patterns during the induction of ventricular tachycardia (VT). lsochronal maps were derived from the consecutive of depolarization that occurred during right atrial rhythm, just before VT, during a transitional cycle of depolarization, and for six cycles of depolarization after the induction of VT (arrows labeled 1 through 6, bottom left in Fig 4). A, Activation pattern of the last normal beat was typical for atrial pacing. Consistent with Fig 3A and 3B, activation emerged on the anterior segment of left epicardium (solid dot) and propagated toward the posterior region. B, Activation pattern of the transitional beat is shown. Activation emerged on the anterior region (solid dot), as in panel A, and propagated at slower apparent velocity and at an orientation similar to subendocardium pacing shown in Fig 3D. C through H, During VT, apparent conduction velocities decreased by -60% (from -2.6 to -0.8 m/s), rate increased from 200 to 600 beats per minute, and wave fronts aligned with the longitudinal axis of fibers of the subendocardium (B and F), midwall (G), or epicardium (C, D, E, and H).21 Activation began at the solid dot and spread according to isochronal line (shown 1 millisecond apart). waves decreased the synchrony of activation since during VT the same region of ventricle depolarized at 30 milliseconds (Figs 5G and 6C) compared with 4 to 5 milliseconds during atrial pacing (Figs 3A and 5A). Activation patterns (Fig 5C through 5H) had similar apparent propagation velocities and orientations compared with those measured during direct electrical pacing of the ventricle, with Omax of 0.84±0.06 m/s. The major isochronal axis of the transitional (Fig 5B) and the fourth beat (Fig 5F) were oriented at a 225°/45° angle, which suggested that activation was initiated deep in the subendocardium, as in Fig 3D. The major isochronal axis of beats 1 (Fig 5C), 2 (Fig SD), 3 (Fig 5E), and 6 (Fig SH) were oriented at 135°/3150, which indicated that the epicardial fiber orientation2' guided the propagation of these wave fronts, as in Fig 3C. The bipolar electrograms indicated that extrastimuli induced a polymorphic VT (Fig 4, tracing ICI) while retaining a stable atrial rhythm (Fig 4, tracing 1C3). The termination of VT was reliably achieved by STS delivered to the Purkinje fibers on the surface of the endocardium (Fig 4, right tracings). Fig 6 described the isochronal maps for beat 110 in the middle of VT, six beats preceding the termination of VT, and the recovery to atrial pacing. The 110th beat depicted a pattern with two activation wave fronts that propagated and collided at the center of the ventricle (Fig 6A). The third beat before atrial rhythm revealed another example of two activation breakthrough sites. The spread of activation during the interruption of VT was consistently slower than during atrial rhythm (Fig 6B through 6C), and the first normal beat exhibited the rapid activation and orientation of activation pattern observed during Purkinje fiber-driven excitation of the ventricles (Fig 6H). Sustained VT could be induced by 5-second trains of burst stimulation (CL, 25 to 50 milliseconds; duration, 0.5 to 10 milliseconds; and voltage, 2x threshold) applied to the endocardium or epicardium or by a single properly timed premature beat (duration, 5 milliseconds; voltage 2x threshold) as illustrated in Fig 10. However, sustained VT could only be induced in hearts isolated from guinea pigs weighing 2450 g, most likely because the larger physical dimensions of their hearts were required to maintain reentrant pathways (n=36). The hearts of 450-g guinea pigs weighed, on average, 2.5 +0.15 g wet weight (n= 12), with a circumference of 44.5+2.8 mm during diastole. VT could not be induced by extrastimulus protocols in hearts with smaller dimensions (n= 12). VT could be terminated by STS (CL, 25 to 50 milliseconds; duration, 0.5 to 25 milliseconds; and voltage, 0.5 x to 0.8 x threshold) applied at various sites on the endocardium, but not on the epicardium. To illustrate the latter result, VT was induced by a train of extraimpulses applied on the endocardium as in Fig 4 (not shown) and was monitored for 45 seconds; then STS was delivered to the epicardium. As shown in Fig 7, Salama et al Subthreshold Stimulation Interrupts VT 613 BASE gc 0 E. C.5 beat A. VT beat #110 3rd beat G. 1l beat n T- 1 - Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 f ar H. Recovery of Atrial Pacing d hont D. 4u beat B. 6m beat FIG 6. Activation patterns during termination of ventricular tachycardia (VT). lsochronal activation maps were derived from transmembrane depolarizations for the 1 1 0th cycle of VT (A), consecutive cycles of VT during the delivery of subthreshold stimulation (B through F), and the recovery to atrial rhythm (H) (arrows, bottom right, Fig 4). The 1 1 0th beat of VT (A) and the third beat before termination (E) each show two early activation sites that resulted in wave-front collisions. The major axis of the wave fronts of most beats (A through C and E through G) aligned with the longitudinal fiber axis of the epicardium. Termination of VT resulted in the immediate recovery of the atrial pacing activation pattern (H). Activation began at the solid dot and spread according to isochronal line (shown 1 millisecond apart). four optical recordings of electrical activity (Nos. 19, 21, 43, and 47) and a ventricular bipolar electrogram were not significantly altered by the firing of STS delivered to the epicardium (bottom tracing). In this case, the electrode delivering STS was located at diode 45 between diode tracings 43 and 47, shown in Fig 7. Fig 7a depicts an activation pattern recorded during VT, and Fig 7b depicts a pattern recorded during VT plus STS applied at diode 45 (square pulse). The location of the STS electrode was changed to various sites on the epicardium; however, STSs at all epicardial sites were equally ineffective at interrupting VT. More precisely, STS BASE a 19 J 21 i f r 2 2 cc cc W L 43 a ~~~~~~~~~~~4 APEX VT beat b 47'' -S S~ BE ; I- ii L STS 1-I STS on the epicardium STS + VT FIG 7. Subthreshold stimulation (STS) delivered to the epicardium failed to interrupt ventricular tachycardia (VT). VT was induced in a guinea pig heart as described for Fig 4, and attempts were made to terminate VT by STS delivered to the epicardium. Recordings from arbitrarily chosen diodes (Nos. 19, 21, 43, and 47) and a recording of a ventricular bipolar electrogram (BE) detected multiple cycles of VT. The logic pulses denoting the delivery of STS on the epicardium (bottom tracing) indicated the onset of STS (50 milliseconds between pulses). a, The activation pattern measured during a cycle of VT (arrow a on tracing 43) propagated according to the epicardial fiber axis. b, The activation pattern measured during a cycle of VT plus STS shows a slight disturbance of the pattern near the STS electrode site (square pulse) but did not interrupt VT, even when the stimulation voltage was increased to 6x threshold. Activation began at diode No. 102 (*) and spread according to isochronal line (shown 1 millisecond apart). 614 Circulation Research Vol 74, No 4 April 1994 0 CU 0 C: c c VCO 0~~2 > Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 > ~~~~10 C~ ~ ~ / 0Ua F-~ 3 K £.*j~~~ 1.i..y~~~.... ~~~ (~~~~~~~~~~~~~~ Cf U) ~~~.~ ~ ~ ~ ~ ~ 2 S~ ~ ~ ~ ~ *~~a~~~~~~~c). (1$.. O~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~a5))t oa)5 ( (2~~~~~~~~~~~~~~~~~~~~-5(t aCOC 0 Ca) 0'~ ( K~~~~~~~~~~~~~~~~~~0U b---C4a1 2 ~~~~~~~~~~~~~~~~~2e-o w at( .) a)C - CU C IO-~ O.°:3( O LL]~ CO a h) c) 0 Salama et al Subthreshold Stimulation Interrupts VT BASE 12 Q E 0 p. rE jI B. Atrial Pacing + STS A. Atral Pacing Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 FIG 9. Effects of subthreshold stimulation (STS) on the epicardium during atrial pacing. Bipolar pacing leads were attached to the right atrium and epicardium. A, Activation pattern measured during atrial pacing had the expected apparent conduction velocity and orientation. B, Simultaneous application of atrial pacing and endocardial STS (at square-pulse symbol at diode 102) caused a local increase in apparent velocity. This resulted in an increase in the number of photodiodes detecting earlier activation times not seen with atrial stimulation alone. On cessation of STS, apparent velocity and the activation pattern reverted immediately back to the control value as in panel A. Numbers indicate activation time delays in milliseconds. failed to interrupt VT when the STS electrode was located at various positions on the apex, base, and anterior and posterior regions, as well as the center of the left and right epicardia. Six hearts were thus tested with STS electrodes located at a minimum of 24 sites on the epicardium. STS Increases Local Apparent Conduction Velocity To elucidate the mechanism whereby STS interrupts VTs, STS was applied on the endocardium under right atrial pacing and during VT to examine the spatial heterogeneities of electrical responses induced by STS. In Fig 8, VT was induced by a single properly timed stimulus (not shown), and STS delivered on the Purkinje fibers lining the endocardium interrupted VT. Fig 8 compares the local effects of STS on depolarizing waves on the epicardium at sites close and farther from the stimulating electrodes. The STS electrode was placed on the endocardium at a site opposite the epicardium viewed by diode 69. Consequently, the optical tracings recorded by diodes 57, 69, and 81 corresponded to electrical activity near the STS site; those recorded by diodes 15, 25, and 49 were distant to the site of STS delivery. From the position of each diode on the array seen in Fig 2, the magnification of the image viewed by the array (ie, each diode viewed a lx 1-mm area of tissue), and the thickness of the left ventricle (1.8 mm), the activities recorded by diodes 69, 57, 81, 49, 25, and 15 were respectively 1.8, 2.04, 2.04, 4.82, 5.9, and 6.7 mm away from the STS electrode. As shown in Fig 8, STS interrupted VT; however, this did not occur instantaneously but gradually as the electrical activity near the site of STS exhibited a gradual increase in rate of rise and amplitude of depolarizations. This implied that STS increased the synchrony of depolarization and the apparent conduction velocity at local sites near the STS electrode. Sites more distant from the STS electrode were not altered by STS pulses, until the interruption of VT. Approximately 15±3 diode recordings nearest the location of the STS site exhibited increases in rate of 615 rise and amplitude (n=6). IC1 on Fig 8 recorded a polymorphic ventricular electrogram during VT, which abruptly changed to a standard right atrial rhythm electrogram waveform with a concordant T wave (lower right of bottom tracing). The effects of STS delivered to the endocardium during normal right atrial pacing rhythm are illustrated in Fig 9. Two bipolar pacing leads were attached to the heart, one on the right atrium (to mimic sinus rhythm) and the other on the endocardium (square-wave symbol). In panel A, the right atrium was paced at a 300-millisecond CL, resulting in the expected epicardial activation patterns (control) recorded during right atrial pacing with a rapid apparent conduction velocity of 2.64+0.14 m/s (n=6). In panel B, the electrode placed on the endocardium was turned on to deliver STS (voltage, 0.5 x threshold; 20 Hz; and duration, 5 milliseconds) during right atrial pacing (as in panel A). This resulted in a larger region of epicardium that fired synchronous APs; ie, a greater number of photodiodes detected APs that fired within the region of epicardium delineated by the 0- and 1-millisecond isochrones compared with the initial sites of activation measured during sinoatrial nodal stimulation alone (panel A). This demonstrated that STS induced a regional decrease in activation delays in a 4x4-mm patch of tissue, causing a local increase in apparent conduction velocity (3.63±0.21 m/s, n=6). On cessation of simultaneous STS, conduction velocity and activation patterns immediately reverted back to those seen with atrial stimulation alone (panel A). The instantaneous change of activation patterns from those shown in panels A and B on STS and the reversal from panel A to B on cessation of STS suggested that these changes were not caused by local release of catecholamine at the site where STS was applied. Termination of VT by Procainamide In contrast to the local increase in apparent conduction velocity by STS, VT could also be interrupted by slowing down AP upstrokes and propagation using procainamide. The induction of VT with a single premature beat and its termination with a bolus administration of procainamide are illustrated in Fig 10. The experimental protocol is similar to that shown in Fig 4, except that VT was induced by a single properly timed premature beat delivered during the relative refractory period of APs on the epicardium (Fig 10, bottom tracings, left). The firing of the extrastimulus is indicated by the solid arrow below 1C3 (Fig 10, bottom, left tracing), which monitored the stimulator output. As in Fig 4, the arrhythmia induced by a premature beat produced a polymorphic ventricular electrogram (IC1), whereas the atrial electrogram remained unaltered (IC2). This indicated that the electrical perturbation produced a VT and that the arrhythmia was not of supraventricular origin. Procainamide (2 ,ug/mL of perfusate) was injected at the cannula inlet in a bolus of perfusate (5 mL) at the time indicated by the arrow (Fig 10, bottom, right). VT was interrupted within 3 seconds after the delivery of procainamide. The termination of VT by procainamide within 3.0 seconds (Fig 10, bottom tracings, right) was remarkably fast, since the time required for the drug to travel from the injection site to the coronary circulation was --2.0 to 2.5 seconds. As a sodium channel antagonist, procain- 616 Circulation Research Vol 74, No 4 April 1994 / .-z- I --- Z.'-- :~ l.' -- 1, Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 ,2 6 j ci 'V. t-, ,C lo. X a -1; -1 I C, Ar -f 0 3. - 7 _ OC 0\ c) .) k .t ;.1 $:. -i- 1 1 1,-. .k11 -YY1-i_ 1-1. _r- ' ' . ;1 Salama et al Subthreshold Stimulation Interrupts VT BASE "4,"-, ' .,1 t2-1 \ \ 0Wz_ip 7 F 181 111 TENlI 1. 18 50 36 IF f 2 APEX B. Procainamide A. Control Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 FIG 1 1. Procainamide decreases apparent conduction velocity during atrial stimulation. The heart was paced synchronously on the right atrium and the base of the left epicardium to measure action potential propagation and activation patterns of epicardial fibers. A, Epicardial excitation was initiated at the location of the electrode pacing the tissue (solid dot) and spread from base to apex as depicted by the isochronal lines of propagation. The directions of the longitudinal and transverse conduction velocities were tangential and perpendicular to the isochronal lines, respectively. B, After a 3-minute perfusion of the heart with perfusate containing 10 ,umol/L procainamide, activation spread at considerably slower velocities, :'2.3 times slower than control conduction velocities. Numbers indicate activation time delays in milliseconds. amide produced the expected decreases in the rate of rise of AP upstrokes and also decreased the amplitude of optical APs. The decrease in AP amplitude occurred because each photodiode recorded the sum of APs from cells in a patch (1 x 1 x0.144 mm) of tissue, and procainamide decreased propagation and the synchrony of AP firing (n=6). When procainamide (10 ,umol/L) was administered to hearts during epicardial pacing (S,, 300 milliseconds), the refractory period on the epicardium did not change significantly, increasing slightly from 88±1.0 to 92±2.0 milliseconds (n=6). On the other hand, the transverse conduction velocity decreased by more than 50% from 0.57±0.15 to 0.25±0.08 m/s (Fig 11). These changes in refractoriness and conduction velocity were reversed by washing out the drug (not shown). In the present experiments, VT induced by extraimpulses were self-sustained, continued for up to an hour, and typically progressed to VF, unless interrupted by STS or procainamide (n=6). These preparations could remain normoxic and survived long periods of VT and VF, because in Langendorff-perfused hearts, coronary perfusion is artificially maintained by the peristaltic pump and the perfusion pressure, which deliver perfusate to the coronary vessels. In the more physiological in situ studies of VT, recoil of blood from the left ventricular ejection fraction provides the driving force for coronary perfusion. Thus, in studies of arrhythmias in situ, VT was shown to decrease, and VF stopped cardiac output and coronary perfusion.25 Discussion The main results are that arrhythmias (most likely VT) can be reliably induced in guinea pig hearts by premature extraimpulse(s) and terminated by STS applied on the endocardium but not on the epicardium. The mapping of APs with voltage-sensitive dyes and imaging techniques provided measurements of activation patterns from the epicardial surface with high 617 spatial and temporal resolution. Activation patterns measured from two-dimensional surfaces on the epicardium were strongly dependent on the stimulation protocol. Control activation maps measured under atrial stimulation were anisotropic with the orientation and apparent propagation velocity typical of activation observed after the direct stimulation of Purkinje fibers lining the surface of the endocardium. In right atrial pacing, epicardial activation patterns were anisotropic (ie, elliptical), and the major and minor axes (ie, longitudinal and transverse conduction velocities) were aligned according to the endocardial fibers, which receive synchronous excitation from Purkinje fibers.21 In contrast, direct stimulation of the epicardium produced anisotropic activation patterns with considerably slower values for Omax and Omin, which were oriented parallel to the longitudinal and transverse axes epicardial fibers, respectively. During VT, activation patterns had orientations and propagation velocities similar to those measured during stimulation of the epicardium or intermediate layers within the ventricular free wall. A most critical observation was that, during VT, activation patterns indicated that Purkinje fibers failed to drive the excitation of the ventricular free wall. Furthermore, activation patterns during VT were most likely caused by a reentry mechanism, since a minimum dimension of the heart was critical to establish sustained arrhythmias. The present study demonstrates that extrastimuli reliably induce VT in a nonhypoxic nonischemic mammalian heart and that STS delivered on the endocardium interrupts VT, whereas STS applied elsewhere failed to terminate VT. Leading Circle VT in the Nonischemic Nonhypoxic Heart The present data raise an important question regarding the nature of the arrhythmias initiated by premature extrastimuli in nonhypoxic nonischemic guinea pig hearts: did premature impulses induce a VT, a VF, or a VT that progressed to VF? This question is not easily resolved, because there are no unique methods to distinguish VT from VF by standard electrogram recordings.26'27 An essential feature of VT is the induction of one primary depolarizing wave front that propagates repeatedly along a reentrant pathway. In one form of VT (ie, circus movement), slow conduction around a ring of tissue and an anatomic barrier are required to maintain a single reentrant loop.13 An important feature of circus-movement VT is that activation wave fronts propagate repeatedly along the same path, resulting in monomorphic electrogram signals. The concept of circus movement had prevailed as the dominant form of VT until the demonstration of leading-circle or leadingedge reentry.16 Leading-circle reentry (single-wave front VT) was characterized by the absence of an excitable gap, because the moment a region of tissue would repolarize, it would depolarize. Another important feature of leading-circle reentry is the lack of anatomic blocks such that VT could be induced in healthy (nonischemic) myocardium.'6 In contrast, VF has been defined as multiple random reentrant wave fronts with so many propagating wave fronts that the mutual extinction of these wavelets becomes improbable.28 However, there were no estimates of the number of simultaneous wavelets necessary to achieve VF. 618 Circulation Research Vol 74, No 4 April 1994 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 In the present studies, the polymorphic ventricular electrogram responses would be interpreted as VF. However, the optical activation maps indicated the occurrence of VT rather than VF, because each cycle of depolarization produced a finite number (one to three) of activation wave fronts that propagated across the left epicardium. The activation map for each cycle of arrhythmia exhibited a different pattern of depolarization but did not reveal a large number of simultaneous propagating waves as postulated by Moe et al.28 Furthermore, these arrhythmias qualify as VT rather than VF because precise activation patterns and propagation velocities were measured for any given cycle of the arrhythmia. Activation exhibited systematic time delays from the first to last region to depolarize, which indicated that the first region to depolarize initiated a wave of depolarization that propagated to the surrounding tissue. Activation wave fronts propagated anisotropically with apparent Omax and Omin values similar to those observed by direct stimulation of the subendocardium (Fig 5B and 5F, Fig 6D), midwall (Fig 5G), or epicardium (Fig SC, SD, 5E, and 5H; Fig 6A, 6B, 6C, 6F, and 6G).21 Activation maps during VT indicated that the Purkinje fibers failed to synchronize the ventricular depolarization because of the longer activation time delays across the epicardium and the shift in the orientation of isochronal lines. The orientation of activation patterns varied from cycle to cycle, but the predominant orientation indicated that activation was guided by the epicardial fiber structure. Optical APs indicated that the moment ventricular cells repolarized, they depolarized with no detectable excitable gap between waves of depolarization. Thus, cells in the process of repolarization are reexcited near their relative refractory period by the next wave of excitation and depolarize almost immediately before establishing a resting potential. This class of VT resulted in polymorphic electrogram recordings, because activation pathways changed from beat to beat and on occasion multiple wave fronts propagated simultaneously and collided. In contrast, VT produced by reentry around an anatomic block (ie, circus movement) would produce monomorphic recordings, because the singleactivation wave front travels along a fixed path, is reproducible from beat to beat, and exhibits an excitable gap between cycles of depolarization. Put together, the best interpretation is that these VTs fell into the category of leading-circle VT. The major limitation of the present study and of the interpretation of the type of arrhythmia induced by a premature beat is that the apparatus did not record activity from other regions of the heart. Nevertheless, activation maps from the left epicardium included a significant part (40%) of the total epicardial surface and were most likely representative of activation patterns occurring elsewhere on the heart. Thus, it is unlikely that more complex (ie, multiple, random) activation wave fronts occurring on the right epicardium would not influence measurements on the left epicardium over the span of several hundred cycles of arrhythmia. Sustained VTs were only obtained in hearts with minimum dimensions, which also indicated that a reentrant mechanism was responsible for these rhythm disturbances and that a minimum reentry path length was required to sustain VT. Thus, premature stimuli delivered to normal guinea pig hearts induced a form of reentrant arrhythmia, most likely polymorphic leading-circle VT. Termination of VT STS delivered to the endocardium of guinea pig hearts interrupted VT within 3 seconds but failed to significantly alter VT when delivered to the epicardium. By changing the location of the electrode delivering STS to the endocardium, it appeared that STS delivered to the Purkinje fibers lining the endocardium was required to interrupt VT. STS frequencies previously reported to be effective at interrupting VT were selected in the present study (CL, 25 to 50 milliseconds). Different STS frequencies were tested on the same hearts to interrupt VTs. In this range of frequencies, there were no frequency-dependent effects in the likelihood of interrupting VT with STS. The actions of STS were also consistent with the generation of a local electrotonic depolarization, which failed to capture and propagate but enhanced the local conduction velocity. As shown in Fig 8, there was an abrupt increase in the rate of rise and amplitude of the upstrokes of APs recorded near the STS site (Nos. 57, 69, and 81). In Fig 9, the simultaneous application of STS during atrial pacing (panel B) caused an increase in the number of photodiodes detecting earlier activation times that were not detected with atrial stimulation alone (panel A). Alternatively, STS may elicit the release of catecholamine from local neurons, which in turn increased the local conduction velocity.29 Activation maps recorded during atrial pacing (Fig 9A) were immediately modified by turning on the endocardial STS (Fig 9B) and reversed back to atrial activation patterns (as in Fig 9A) within one beat (CL, 300 milliseconds), a time course too fast to be attributed to catecholamine release. The latency of onset of a catecholamine response after a burst of sympathetic stimulation is '-1.0 to 1.5 seconds, whereas the response lasts :20 seconds.3031 Even if catecholamine release is involved in the termination of VT by STS, it is not a sufficient criterion because STS delivered to the epicardium should also elicit catecholamine release yet fail to interrupt VT. Shenasa et al0 suggested that STS is only effective on the endocardium because the endocardium is the site responsible for the initiation of reentrant VTs. Although this hypothesis cannot be entirely excluded, the patterns of activation during VT indicate that the initiation site varies from beat to beat and in many cases appears to originate at the left epicardium. Acknowledgments This study supported by American Heart Association (AHA) grant 87-1065, the Western Pennsylvania Affiliate, Inc, of the AHA, and the Whitaker Research Foundation (Dr Salama). The authors would like to thank Dr Mohammed Shenasa for suggesting these experiments, Richard A. Lombardi and William Bolish for the development of software to analyze activation patterns, and William Hughes for machining the experimental chamber and optical components. was References 1. Lewis T, Drury AN. Revised review of the refractory period in relation to drug reputed to prolong it, and in relation to circus movement. Heart. 1926;13:95-100. 2. Tamargo J, Moe B, Moe GK. Interaction of sequential stimuli applied during the relative refractory period in reiation to deter- Salama et al Subthreshold Stimulation Interrupts VT 3. 4. 5. 6. 7. 8. 9. 10. Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 11. 12. 13. 14. 15. 16. mination of ventricular fibrillation in the canine ventricle. Circ Res. 1975;37:534-541. Prystowsky EN, Zypes DP. Inhibition in the human heart. Circulation. 1983;68:707-713. Skale BT, Kallok MJ, Prystowsky EN, Gill RM, Zypes DP. Inhibition of premature ventricular extrastimuli by subthreshold conditioning stimuli. J Am Coll Cardiol. 1985;6:133-140. Von Leitner ER, Linderer T. Subthreshold burst pacing, a new method for termination of ventricular and supraventricular tachycardia. J Am Coil Cardiol. 1984;3:472. Gang ES, Peter T, Nalos PC, Meesmann M, Hrayo S, Karaguezian HS, Mandel WJ, Oseran DS, Meyers MR. Subthreshold atrial pacing in patients with a left-sided accessory pathway: an effective new method for terminating reciprocating tachycardia. J Am Coll Cardiol. 1988;11:515-521. Johnson N, Danilo P Jr, Wit AL, Rosen MR. Characteristics of initiation and termination of catecholamine-induced triggered activity in atrial fibers of coronary sinus. Circulation. 1986;74: 1168-1179. Jalife J, Antezelevitch C. Phase resetting and annihilation of pacemaker activity in cardiac tissue. Science. 1979;206:695-697. Verrier RL, Lown B. Prevention of ventricular fibrillation by use of low intensity electrical stimulation. Ann N YAcad Sci 1982;382: 355-370. Shenasa M, Cardinal R, Kus T, Savard P, Fromer M, Pag P. Termination of sustained ventricular tachycardia by ultrarapid subthreshold stimulation in humans. Circulation. 1988;78:1135-1143. Windle JR, Miles WM, Zypes DP, Prystowsky EN. Subthreshold conditioning stimuli prolongs human ventricular refractoriness. Am J Cardiol. 1986;57:381-386. Rothschild R, Stevenson WG, Klitzner T, Weiss J. Enhancement of conduction in an accessory pathway by local noncapture stimuli. JAm Coll Cardiol. 1987;9:455-458. Mines GR. On dynamic equilibrium in the heart. J Physiol (Lond). 1913;46:349-382. Dillon SM, Allessie MA, Ursell PC, Wit AL. Influences of anisotropic tissue structure on reentrant circuits in the epicardial border zone of subacute canine infarcts. Circ Res. 1988;63:182-206. Allessie MA, Schalij MJ, Kirchhof CJHJ, Boesma L, Huybers M, Hollen J. Experimental electrophysiology and arrhythmogenicity: anisotropy and ventricular tachycardia. Eur Heart J. 1989;10(suppl E):2-8. Allessie MA, Bonke FIM, Schopman FJG. Circus movement in rabbit atrial muscle as mechanism of tachycardia, III: the "leading circle" concept: a new model of circus movement in cardiac tissue 17. 18. 19. 20. 21. 22. 23. 24. 619 without the involvement of anatomical obstacles. Circ Res. 1977; 41:9-18. Salama G, Lombardi R, Elson J. Optical maps of action potential propagation and NADH fluorescence in intact working hearts. Am J Physiol. 1987;252H:384-394. Gregg DE, Khouri EM, Rayford CR. Systemic and coronary energetics in the resting unanesthetized dog. Circ Res. 1965;16:102-113. Berne RM, Rubio R. Coronary circulation. In: Berne RM, ed. Handbook of Physiology, Section 2: The Cardiovascular System, Volume I, The Heart. Bethesda, Md: American Physiological Society; 1979:873-952. Rodolphe R. Subthreshold stimulation of the heart: small but important. PACE Pacing Clin Electrophysiol. 1980;13:110-118. Kanai A, Salama G. Maps of optical action potentials and fiber structure in guinea pig ventricles. Circulation. 1988;78(suppl II): II-413. Abstract. Oppenheimer AV, Schafer RW. Digital Signal Processing. Englewood Cliffs, NJ: Prentice-Hall, Inc; 1975:26-30. Salama G, Rosenbaum D, Kanai A, Cohen RJ, Kaplan DT. Data analysis techniques for measuring spatial inhomogeneities in repolarization using optical transmembrane potentials. Proceedings of the International Conference of the IEEE Engineering in Medicine and Biology Society. 1989;11:222-223. Nielsen PMF, Le Grice IJ, Small BH, Hunter PJ. Mathematical model of geometry and fibrous structure of the heart. Am J Physiol. 1991;260:H1365-H1378. 25. Snyder R, Downey JM, Kirk ES. The active and passive components of the extravascular resistance. Cardiovasc Res. 1975;9: 161-166. 26. Cranefield PF, Wit AL. Cardiac arrhythmias. Annu Rev Physiol. 1979;41:459-472. 27. Spear JF, Moore EN. Mechanisms of cardiac arrhythmias. Annu Rev Physiol. 1982;44:485 -497. 28. Moe GK, Reinboldt WC, Abildskov JA. A computer model of atrial fibrillation. Am Heart J. 1964;67:200-220. 29. Wit AL, Hoffman BF, Rosen MR. Electrophysiology and pharmacology of cardiac arrhythmias, IX: cardiac electrophysiologic effects of beta-adrenergic receptor stimulation and blockade. Am Heart J. 1975;90:521-533. 30. Braunwald E, Harrison DC, Chidsey CA. The heart as an endocrine organ. Am J Med. 1964;36:1-4. 31. Spear JF, Moore EN. Influence of brief vagal and stellate nerve stimulation on pacemaker activity and conduction within the atrioventricular conduction system of the dog. Circ Res. 1973;32:27-41. Subthreshold stimulation of Purkinje fibers interrupts ventricular tachycardia in intact hearts. Experimental study with voltage-sensitive dyes and imaging techniques. G Salama, A Kanai and I R Efimov Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Circ Res. 1994;74:604-619 doi: 10.1161/01.RES.74.4.604 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1994 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/74/4/604 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/