Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
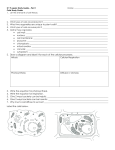
POSTEROLATERAL CORNER • Complex anatomy and infrequent lessions but with clinical relevance. • Their injuries are usually associated with rupture of one or both cruciate ligaments. Particularly PCL (62%). • Mechanism of injury: Most common: direct blow to the anteromedial proximal tibia, directed posterolaterally, with the knee near full extension or a noncontact, external rotation hyperextension injury. • The significance of a missed PCL injury can have serious consequences such as chronic instability, degenerative changes or predispose to failure of the cruciate reconstruction. Components of the PLC • Superficial layer -Iliotibial band -Biceps femoris tendon -Lateral gastrocnemius tendon o Deepest layer v Fibular collateral ligament v Fabellofibular ligament (inconstantly) v Popliteal tendon-muscle unit: consist of q Popliteus muscle and tendon q Popliteofibular ligament q Arcuate ligament q Posterolateral joint capsule Specific components that can be identified on MRI ü Fibular collateral ligament ü Popliteal tendon muscle unit including popliteofibular ligament ü Biceps femoris tendon. Iliotibial band ü Fabello fibular ligament ü Arcuate and Segond Fractures MRI protocols • We strongly suggest the application of 1.5 or 3 Tesla scanners. • We perform a routine knee protocol that includes axial, sagital and coronal DP or T2 FAT SAT 3mm sequences, a sagital DP, a coronal T1 WI 3mm, sagital T2 FAT SAT WI 3mm and a axial STIR 3mm sequences. • We recommend performing coronal oblique images in order to improve the examination showing the arcuate and popliteofibular ligaments. Anatomic illustration of posterolateral corner of the knee demonstrating most of the components and their relation with other structures. Fibular collateral ligament BICEPS FEMORIS TENDON Normal FCL: Consecutive coronal FSE T1 weighted images The lateral collateral ligament originates from the lateral femoral epicondyle and extends distally and posteriorly over an oblique course to insert on the lateral aspect of the fibular head, anterior and distal to the tip of the fibular styloid process. FIBULAR COLLATERAL LIGAMENT FIBULAR STYLOID PROCESS Sagital FSE T1 weighted image Distally, fibular collateral ligament often joins with biceps femoris tendon Biceps Femoris Tendon The long and short heads of the biceps femoris tendon typically join above the knee and course distally to insert predominantly into the lateral aspect of the fibular styloid Normal BFT: Consecutive coronal FSE T1 weighted images Coronal fat-suppressed fast spin-echo T2-weighted images shows fluid signal extending along the fibular collateral ligament and the biceps femoris tendon consistent with slight injury Coronal FS FSE T2–weighted MR image shows avulsion and retraction of biceps femoris tendon (arrows). Avulsion of biceps femoris tendon. Coronal fatsuppressed T2-weighted image shows distal tear of this structure from fibular head (arrow) Avulsion of lateral collateral ligament and biceps femoris tendon. Consecutive axial fat-suppressed T2weighted image show distal tear of both structures from fibular head (arrow) Avulsion of lateral collateral ligament and biceps femoris tendon. Coronal FSE T1 weighted image and sagital fat-suppressed T2-weighted image depict distal tear of both structures from fibular head (arrows). Popliteus muscle-tendon unit The popliteus muscle is a major dynamic stabilizer of the lateral knee and arises from the posterior medial tibia, extending superiorly and laterally to form a tendon that continues into the joint through the popliteal hiatus, deep in relation to the fabellofibular and arcuate ligaments to insert onto the lateral surface of the femoral condyle. Popliteus muscle-tendon unit POPLITEUS TENDON Normal popliteus muscle-tendon: Consecutive axial FS FSE DP weighted images POPLITEUS MUSCLE Popliteus injuries. Coronal fat-suppressed fast spin-echo T2-weighted images depict fluid signal extending along margins of popliteus muscle belly (arrow), consistent with partial tear. Popliteus injuries. Axial and sagital fatsuppressed fast spin-echo T2-weighted images show edema at myotendinous junction of popliteus (arrows), consistent with partial tear in this region. ASSOCIATE LESSIONS WITH POPLITEUS MUSCLE-TENDON UNIT Calcific tendinitis of popliteus muscle-tendon. Coronal FS FSE T2 weighted image depicts small areas of low-signal present within the popliteus muslce and tendon that was suspected to be calcification. Ganglion of the popliteus tendon Axial and coronal FS FSE images of a knee show a small cystic structure (arrows) within and over the anterior margin of the popliteus tendon, reflecting a ganglion cyst. Normal popliteofibular ligament. Coronal T1-weighted image and anatomic illustration depict this structure which originates near the popliteus musculotendinous junction and courses laterally to attach to the medial aspect of the fibular styloid process (arrow) Popliteofibular ligament Torn of popliteofibular ligament. Coronal fatsuppressed fast spin-echo T2-weighted image shows avulsion of distal popliteofibular ligament (arrow) from fibular styloid process. Fabello fibular ligament Normal fabello fibular ligament: Coronal FSE T1 weighted image shows this variably present ligament which extends from the fabella to the styloid process (arrow). This ligament arises from the fabella, if a fabella is present, or from the posterior aspect of the supracondylar process of the femur to insert distally on the posterior and lateral edges of the fibular styloid process, anterolateral to the insertion of the popliteofibular ligament. Lateral gastrocnemius tendon PLANTARIS BICEPS FEMORIS Is a superficial muscle which arises from the supracondylar tubercle of the lateral condyle. Then spreads out into an aponeurosis Axial FS FSE DP images and coronal FSE T1 weighted image shows the lateral gastrocnemius muscle-tendon which extends near the plantaris and biceps femoris muscle-tendons (red arrows). The iliotibial band is a combination of the tendon of the tensor fascia lata and the deep and superficial fibers of the gluteus major. Consists of deep and superficial layers. The superficial layer is the main tendinous component and inserts onto Gerdy’s tubercle on the anterior lateral tibia. The deep layer inserts on the distal femur. Isolated tears of the iliotibial band are rare, but these tears may occur in patients with injuries to multiple ligaments of the knee. Coronal FS FSE proton density and FSE T1 weighted MR images illustrate fluid signal extending along margins of the superficial layers of the iliotibial band (arrows) consist of disruption of fibers (partial tear). Arcuate ligament Drawing of posterolateral corner of the knee demonstrating the Y shaped of the arcuate ligament which arises from the fibular styloid and divides into two limbs. The lateral extends superiorly to merge with the posterior capsule, whereas the medial limb extends superomedially, over the popliteus, to join fibers with the oblique popliteal ligament Arcuate ligament Intact arcuate ligament . Axial fat-suppressed fast spin-echo T2-weighted image at level of joint line shows arcuate ligament with no signs of injury Torn arcuate ligament . Axial fat-suppressed fast spin-echo T2-weighted image shows tear of posterolateral joint capsule (arrows) at level of joint, which is consistent with arcuate ligament tear. Drawings of the fibula showing the insertions of ligaments and tendons. Popliteofibular ligament inserts in upper facet of apex of fibular head, just medial to insertions of fabellofibular and arcuate ligaments. Lateral collateral ligament and direct arm of long head of biceps femoris tendon are attached to lateral margin of fibular head. Arcuate fracture Coronal FSE T1 weighted image shows a small fracture (arrows) at the medial aspect of the fibular head. The “arcuate” sign or fracture is an avulsion fracture of the fibular head and styloid. Could be comprise the attachment of the lateral collateral ligament, biceps femoris tendon and arcuate ligament complex.It is usually associated with cruciate ligament injury (mostly PCL) The importance of this injury is that if it is not diagnosed acutely, posterolateral instability could develop and may result in failed cruciate ligament reconstruction Sagital, coronal and axial FS FSE T2weighted MR images illustrates bone bruises (arrows) at the level of the medial aspect of the fibular head. In this case there were not assocciate ligament or tendon injuries. Segond fracture Segond fracture is an avulsion fracture of the knee which involves the lateral aspect of the tibial plateau, and is particularly frequently (75% of cases) associated with disruption of the anterior cruciate ligament. However, there are additional frequently encountered injuries. Other assocciate injuries include: ü Avulsion of the biceps femoris tendon ü Avulsion of the fibular collateral ligament ü Avulsion of the iliotibial band ü Medial or lateral meniscal tear Segond fracture Axial, sagital and coronal FS FSE T2-weighted MR and coronal FSE T1 images illustrates bone bruises (arrows) at the level of the lateral aspect of the tibia plateau in a 21-year-old woman with acute posterolateral corner injury Typically these injuries are seen in two settings: Ø falls Ø sports: especially skiing, basketball and baseball Associate lessions with PLC Injuries of posterior cruciate ligament. Sagital FSE T2 and sagital FS FSE DP weighted images show mid intrasubstance increased signal present in the PCL (arrow) compatible with an interstitial partial tear. Injury of anterior cruciate ligament. Sagital FSE T2 weighted image depicts disruption of fibers (arrow) in the proximal and mid ACL consistent with complete tear. Medial femoral condyle contusion. Axial FS FSE T2weighted image shows increased signal intensity within bone marrow of anterior aspect of medial femoral. condyle SUMMARY • The knowledge of the normal and abnormal MRI appearances of the structures of the PLC of the knee as well as the patterns of injury will help radiologist suggest the diagnosis of PLC injury even when is not clinically suspected. • Tears of 2 or more PLC components suggest the diagnosis of high grade PLC injury and should direct the orthopedic to consider surgical tratment (especially when fibular collateral ligament and the poplteus musculotendinous unit including PFL and arcuate ligament are injuried). • This diagnosis is utterly significant in the setting of combined injuries (PCL-ACL). Furthermore, unrecognizes high grade PLC injuries may lead to significant graft failures, instability and also osteoarthritis. • Conversely, injury to only one of the PLC structures, depending on the associated injuries can often be successfully treated nonsurgically.