Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
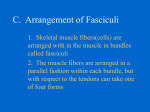
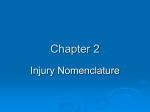
APPLIED SCIENCES Biodynamics Overuse injuries in youth sports: biomechanical considerations DAVID HAWKINS and JEFF METHENY Exercise Biology Program, Exercise Science Graduate Group, Biomedical Engineering Graduate Group, University of California, Davis, Davis, CA; and Sutter West Medical Group, Davis, CA ABSTRACT HAWKINS, D., and J. METHENY. Overuse injuries in youth sports: biomechanical considerations. Med. Sci. Sports Exerc., Vol. 33, No. 10, 2001, pp. 1701–1707. Many children today participate in highly organized sports programs that involve regimented year-round repetitive training. This type of training has led to an increased incidence of overuse musculoskeletal injuries. Sports physicians have dealt with sports injuries in children for many years and, on the basis of their clinical experience, have developed guidelines to treat and to try and prevent these injuries. The purpose of this article is to provide a biomechanical perspective of sports injuries in young athletes and blend ideas from this perspective with more traditional clinical perspectives that dominate the literature relative to this topic. Basic tissue and gross movement mechanics principles are used to identify growth, morphological, and movement factors that may predispose a child to an overuse injury. Several biomechanical analyses of simple movement tasks are presented to quantify the forces developed in various tissues and to illustrate the effects that growth can have on these forces. Guidelines are given for developing injury prediction models that may be used in the future to establish safe and effective training guidelines for children. Key Words: MECHANICS, CHILDREN, ATHLETICS, YOUTH, MUSCULOSKELETAL, TRAUMA A prevention guidelines. Biomechanical analysis techniques are used to identify various factors that may contribute to overuse injuries, to illustrate how injury sites may be predicted, and to describe what is needed to develop reliable injury prevention guidelines in the future. large number of children are injured each year as a result of participation in strenuous physical activities. Treating these injuries is costly and the injuries can lead to long-term health problems (10,13). Reducing the incidence of these injuries may be achieved by identifying factors that may predispose a child to injury and through proper training, technique, and fitness. Efforts to reduce these injuries are warranted both to ensure the long-term health of children and to reduce medical costs. Ideally, we would like to have a simple set of guidelines that outline exactly how often a child can exercise, at what intensity, and for what duration to optimize the physical and psychological benefits of exercise and to minimize the risk of overuse injuries. Such guidelines are elusive but may be achievable through the collective efforts of scientists and clinicians. Numerous articles have been written over the past 20 yr discussing overuse injuries in children from a clinical perspective (2,8,11,12,16,28,29). Most of these articles have been written by physicians on the basis of their clinical observations and experience. The purpose of this report is to evaluate overuse injuries in children from a biomechanical perspective and to provide direction for developing injury HISTORICAL PERSPECTIVE Children’s physical activities today are much different than they were 50 –100 yr ago; 100 yr ago, physical chores, free play, and sandlot sports dominated the spare time of American children. Now, children participate in organized and regimented physical activities. The number of children participating in organized sports programs has increased considerably over the past 70 yr from practically zero in 1930 (before the establishment of organized sports programs such as Pop Warner football and Little League baseball) to approximately 50% today (26,27). There were approximately 60 million children between 5 and 18 yr of age living in the United states in the year 2000 (25). Approximately 38% of high school children (27) and 34% of middle school children (1) will sustain a physical activity related injury that will be treated by a doctor or nurse. It is likely that the actual number of injuries incurred by these children is larger than cited because of the fact that many injuries go unreported. Although younger children presumably sustain fewer sports related injuries compared 0195-9131/01/3310-1701/$3.00/0 MEDICINE & SCIENCE IN SPORTS & EXERCISE® Copyright © 2001 by the American College of Sports Medicine Submitted for publication September 2000. Accepted for publication January 2001. 1701 with older children because of differences in size and strength, a conservative estimate of the number of children that will incur and be treated for a sports/physical activity related injury this year is 18 million (30% of 60 million). It is estimated that approximately 50% of these injuries (9 million) can be attributed to overuse-type mechanisms (2). The total cost to treat these potentially preventable overusetype injuries is approximately $1.8 billion (assuming an average cost for treatment of $200 (1) and 9 million preventable injuries per year). The cost and long-term health risks associated with overuse injuries in children warrants developing tools or strategies that can be used to prevent and treat these injuries. Biomechanical analysis techniques provide one such tool. BIOMECHANICAL ANALYSIS Biomechanical analysis techniques provide a way to estimate the forces and deformations experienced by various tissues during human movement. Understanding the physical principles involved in these techniques is useful for identifying factors that may contribute to injury mechanisms. The body and individual limb segments move according to basic physical principles. According to Newton’s second law, the sum of all forces (⌺F) acting on a rigid body is equal to the product of the body’s mass (m) and its linear acceleration (a) (i.e., ⌺F ⫽ ma). Similarly, the sum of all moments (M), or torques, acting on a body is equal to the product of the body’s moment of inertia (I), which is a measure of the radial distribution of mass about an axis of rotation, and its angular acceleration (␣) (i.e., ⌺M ⫽ I␣). The resultant forces and moments that act on a limb segment result from external loads applied to the segment, as well as forces developed in muscle-tendon units, ligaments, and bones associated with the segment. If the kinematics (e.g., the position, velocity, and acceleration) of a segment are known, then the resultant forces and moments acting on the segment to cause that motion can be determined. Such an analysis is called inverse dynamics. Once the resultant forces and moments are known, then they can be distributed among individual tissues if the structural properties (i.e., mechanical behavior that depends on the properties of the material constituting the tissue as well as the tissue’s size and shape) of these tissues are known along with the relative location and direction of ligament and tendon attachments to bone. This is referred to as a distribution problem analysis. A different approach called forward dynamics prescribes the forces developed by individual muscles and determines how the body moves on the basis of Newton’s laws and the forces induced in bones, tendons, and ligaments. Relative to injury mechanisms, the forces and deformations developed in the muscles, tendons, ligaments, and bones are of interest as well as the tolerance these tissues have to such forces and deformations. The physical principles described above indicate that to understand and predict injury mechanisms in the growing child requires an understanding of 1) limb inertial properties (i.e., mass, center of mass location, moments of inertia); 2) muscle strength; 3) bone, ligament, and 1702 Official Journal of the American College of Sports Medicine FIGURE 1—Body height growth rate for five different males illustrating the variability in growth rate and timing. These curves were constructed from data published by Tanner (21). tendon structure and structural properties; 4) external loading conditions; and 5) how all these factors change with age and exercise. A review of these relevant topics is given below. GROWTH AND DEVELOPMENT Gross properties. Overall body height and mass increase during childhood, often at sporadic rates. Body mass increases on average from 18 kg to 55 kg in females and 18 kg to 73 kg in males between 5 and 18 yr of age. Body height increases from 110 cm for males and females to 160 cm in females and 175 cm in males over this same age range. Girls tend to reach their peak body height and mass around 15 yr of age, whereas boys continue to increase their body mass and height beyond age 18 (9,18,19,21). An important aspect of growth that may increase the risk of injury is the growth rate. The growth rate of an individual is not accurately characterized by average growth curves. The growth spurt in boys may occur any time between 10 and 18 yr of age (Fig. 1) and may reach a peak value of 8 to 12 cm·yr⫺1. Growth spurts may result in changes in the ratios of muscle strength to body or limb mass and moments of inertia, and soft tissues may experience increased stress and strain (discussed later in this section). Limb length, mass, and moments of inertia change with age (Table 1) (4,5,19). On average, limb lengths increase by a factor of about 1.4 between 6 and 14 yr of age. Limb masses increase by more than 3-fold over this same age range. Limb moments of inertia increase with age as a result of increased limb length and mass. Limb moments of inertia, TABLE 1. Limb length, mass, and moment of inertia change with age: the ratios of these quantities at age 14 compared with age 6 are listed. Lower leg Thigh Forearm Upper arm Torso a Length Ratioa Mass Ratiob Itransverse Ratioc 1.4 1.4 1.4 1.4 1.3 3.4 3.8 3.2 3.5 2.7 10.0 12.9 10.0 10.0 6.0 Snyder et al., 1977; b Jensen, 1987; c Jensen and Nassas, 1988. http://www.acsm-msse.org FIGURE 2—Biomechanical analysis of a stationary knee extension task. A free-body diagram of the lower leg is shown on the middle left. Newton’s equations are shown on the middle right. F, resultant force; m, lower leg plus foot mass; a, lower leg acceleration (equal to zero in this example); T, resultant torque; I, moment of inertia of the lower leg plus foot about its center of mass; ␣, lower leg angular acceleration (equal to zero in this example); Fx and Fy, horizontal and vertical components, respectively, of the resultant force acting on the proximal end of the lower leg; L, distance from the knee joint center to center of mass of the lower leg plus foot; g, gravitational acceleration; Tm, muscular torque acting at the knee. The 6-yr-old must generate a knee extension torque equal to 2.2 Nm to hold the lower leg horizontal, whereas the 14-yr-old must generate a 10.3-Nm torque. relative to a transverse axis, increases on average by a factor of 10 between 6 and 14 yr of age. The rate at which these quantities change depends on the child. The affect these changes have on movement performance and muscle strength requirements can be illustrated by analyzing a simple movement task. Consider the task of holding the lower leg horizontal while sitting in a chair. The quadriceps muscles need to generate 4.7 times (10.3 Nm vs 2.2 Nm) more knee extension torque to hold the limb stationary at age 14 compared with age 6 (on the basis of a biomechanical analysis, a 140% increase in leg length, and a 340% increase in limb mass; Fig. 2 and Table 1). There is an increase in muscle moment arm during the aging process that allows a 4.7-fold increase in joint torque to be generated by a 3.9-fold increase in muscle force. The increase in muscle force required to accelerate the leg during dynamic actions is even greater than the 3.9-fold increase required for static conditions. Therefore, if the same activities are to be performed at age 14 as were performed at age 6 without increased muscle fatigue or increased stress in tendons and apophyses, then there must be an increase in muscle strength and a corresponding increase in the strength of muscle-tendon junctions, the tendons, and the apophyses. Quadriceps muscle BIOMECHANICAL PERSPECTIVES OF SPORTS INJURIES strength increases on average about 3.3-fold between 6 and 14 yr of age (17). This average strength change is similar to the change in static strength needed to perform the knee extension task described above, and suggests that on average muscle strength increases appropriately to match changes in limb inertial properties in the long term. Relative to injury mechanisms, it is important to understand how limb growth affects the muscle forces that must be generated by a child to perform a movement task, but it is also important to understand how growth affects the strength of tendon, apophysis, ligaments, and bone. The acute and chronic changes experienced by these tissues relative to each other are important. A muscle group may adapt quickly to accommodate increased demands created either by changes in limb inertial properties or changes in physical activity and generate greater force either by increasing its size or activating a greater portion of its mass. If the tendons and apophyses associated with that muscle group adapt slowly, then the stress induced in the tendons and apophyses will increase in response to the increased muscle force and perhaps lead to injury. Unfortunately, data on the relative strengths and rate of strength changes between muscle, tendon, ligament, and insertional zones are lacking for both humans and animals (discussed in the next section). Although acute limb anthropometry and muscle strength data are not readily available, a simple biomechanical example illustrates how tissue forces must increase during a growth spurt to maintain a certain movement performance. Imagine that a child’s lower leg grows from 26 cm to 30 cm in length during a growth spurt. If muscles and tendons lengthen during the growth spurt, but they do not hypertrophy until some time after the growth spurt, then because of the increased limb mass and moment of inertia the muscles will need to develop a greater percentage of their maximum force to produce movements similar to those performed before the growth spurt. The increased muscle forces will cause the tendons to experience increased stresses. Using conservative estimates of the changes in limb mass that might occur for the lower leg length change stated and solving the equations of motion for the lower leg (see Fig. 2) indicates that the thigh muscles need to develop about 30% more force after the growth spurt to develop the same lower leg angular acceleration that might be required during a kicking movement. The child may or may not be able to produce this additional force. If the task required a muscular effort near maximum before the growth spurt, then the child will not be able to perform the task after the growth spurt. If the child can produce the needed force, then the tendons and apophyses will be subjected to greater stresses/strains until they can adapt to the new loading conditions. Muscle fatigue and/or overuse injuries may result if this activity is performed repetitively (e.g., swinging the leg repetitively to kick a soccer ball). An interesting concept that has received very little attention relative to injury mechanisms is tissue preload (i.e., the amount of force sustained by a tissue in a normal relaxed state of the body). The higher a tissue’s preload, the higher the acute and chronic force that tissue will apply to other Medicine & Science in Sports & Exercise姞 1703 tissues. A muscle-tendon unit may experience an increased preload if the bone grows faster than the muscle-tendon unit. Consider the 4-cm growth spurt of the lower leg described previously. The plantar flexor and dorsi flexor muscles and tendons act in a lengthened position as a result of the bone growth. Presumably, these muscle-tendon units increase their length over time to restore their “preferred” preload, but it is likely that initially these muscle-tendon units act in a stretched position and experience an increased preload. This would result in a chronic increase in force applied through the tendons and apophyses. No studies have been performed to test this idea, but the incidence of apophysitis in growing children suggests that increased tendon preload may be a contributing factor to the injury. A gross measurement that can indicate changes in tissue preload is flexibility. A reduced flexibility may result from an increase in tissue preload, an increase in tissue stiffness, and/or an increase in bony and cartilage geometry around the joint. Interestingly, boys tend to lose back and leg flexibility between 8 and 13 yr of age (9). This may predispose boys to lower extremity tendon and apophysis injuries. Tissue properties. Structural properties describe the mechanical behavior of the whole tissue, whereas material properties describe the mechanical behavior of the material constituting the tissue. The integrity of a functional unit such as a bone-ligament-bone (BLB) or muscle-tendonbone (MTB) complex depends on the relative structural properties of the individual tissues. Structural properties are affected by the tissue’s material properties and the tissue’s geometry (e.g., length and cross-sectional area). The relative structural properties of tissues acting in series need to be matched (e.g., muscle-tendon-insertion) to minimize the risk of injury. Unfortunately, very little information is available regarding tissue structural properties for the growing child. There is even less information about the interaction between exercise, growth and development, and tissue properties. Limited human data suggest that muscle and tendon do not grow proportionally. Elbow flexion (21) and knee extension (17) strength increase on average by a factor of 1.8 between 10 and 15 yr of age. However, hamstring muscle tendons and biceps brachii tendons increase in cross-sectional area by a factor of about 1.5 during this same time frame (6). These data suggest that tendon may operate closer to its failure limits as maturity is reached, or the material properties of tendons change during maturation, resulting in an increase in the strength of the material. Despite the lack of direct information about tissue properties in children, data from animal and cadaver studies provide insight into the complex interactions between age, activity, and modes of injury for various functional units such as BLB and MTB (7,14,15,20,22–24,30 –33). Ligaments and tendons become stiffer and stronger during maturation (31,33). These tissues withstand greater stress and strain before failure as the loading rate increases (33). BLB complexes tend to fail by avulsion in immature animals and by midsubstance tears in mature animals (31). There are differences in the strain induced in different regions of BLB 1704 Official Journal of the American College of Sports Medicine and MTB complexes. The tendon insertion zone appears to experience twice as much strain as the tendon under moderate stress (20). Tendons become stronger in response to long-term exercise, but the cross-sectional area of the tendon does not necessarily increase in proportion to the strength gain (30). This suggests that the material properties of the tendon change in response to exercise. These studies highlight the important and asynchronous rates of tissue changes that likely occur in the growing child. The examples given above illustrate relative changes in muscle and tendon size during maturation, but they do not indicate the absolute stress that a muscle might induce in a tendon. A biomechanical analysis of a simple movement task provides some insight in this area. Consider the forcegenerating potential of the triceps surae muscle group of a 6-yr-old girl. The girl generated an 18-Nm plantar flexion torque during an isometric effort. On the basis of her anatomy, a 1000-N triceps surae force was required to generate that torque. Her Achilles tendon had a cross-sectional area of approximately 35 mm2 (on the basis of ultrasound measurements). A 28-MPa stress was induced in the tendon and insertion zone during the plantar flexion effort, assuming the tendon-bone insertion cross-sectional area is similar to the tendon cross-sectional area. The ultimate tendon and insertion failure stresses are estimated to be 50 MPa and 45 MPa, respectively, on the basis of tissue properties obtained in the various animal studies described above (33). It should be recognized that tissue failure stresses vary considerably with age and loading rate in young children. The plantar flexion effort would induce 63% and 56% of ultimate stresses in the bone and tendon, respectively. Tendon tests suggest that little damage is created for strains less than 3% and stresses less than 40 to 50% of ultimate stress (6). Thus, the 63% of ultimate stress calculated in the above example suggests that if this child were to perform this activity repetitively, she may be at risk for sustaining an apophysis overuse injury. INJURY PREVENTION MODEL The previous discussions highlight only a few of the factors that may contribute to childhood overuse injuries, but they provide a foundation and direction for future endeavors that may lead to injury prediction models. There are many factors that contribute to tissue injury, including the strength of the tissue, the magnitude of the loads applied to the tissue, the number of loading cycles, the recovery period between loading bouts, and the rate of tissue repair. Unfortunately, because of the complex interactions between these various factors, there do not exist quantitative models for predicting conditions that lead to injury. Our current injury prevention guidelines, such as the 10% rule or the limits set for the number of allowable pitches that can be thrown by young baseball pitchers (28), are derived from clinical observations and epidemiological data, not an understanding of basic physiology and mechanics. If we are to develop injury prediction models for musculoskeletal tissues, then we must 1) characterize tissue structural properties, 2) characterize tissue rates of adaptive rehttp://www.acsm-msse.org repair rate was insufficient to cause complete recovery between exercise bouts: DF ⫽ N䡠⑀q/K FIGURE 3—Illustration of an injury prediction model. This model estimates the amount of damage that a tissue will incur during an exercise bout as a function of the number of loading cycles and the level of strain induced in the tissue during each loading cycle. The number of loading cycles would be determined from the activity. The strain induced in the tissue would be determined from biomechanical analysis techniques and information about the structural and material properties of the tissue. The contour plot shown was derived for cortical bone. sponses, 3) predict the loading profiles that tissues are exposed to during various activities, and 4) develop more complete injury tracking systems. Efficient methods need to be developed to characterize the structural properties of specific tissues constituting functional units (e.g., MTB) and to track how these properties change with maturation and in response to exercise. We need to characterize how tissues respond to various loading parameters (e.g., the load magnitude, duration, and frequency) as well as the repair rates for these tissues. This will require integrating information from both clinical observations and basic research. Tissue properties and the rates at which they adapt to altered loading conditions can be quantified using animal models and perhaps human studies. Human studies may involve noninvasive imaging technology combined with specialized joint strength testing equipment (3). Musculoskeletal modeling and computer simulation techniques are approaching the sophistication needed to quantify the forces induced in individual tissues during prescribed movements. Injury tracking systems need to become more comprehensive and include information that may be used to test injury prediction models such as the loading history before an injury. A simplistic injury prediction model is given in equation 1 and illustrated in Figure 3. This model is derived from basic fatigue fracture studies of bone, expanded to characterize other tissues. This model considers the number of loading cycles (N) and the strain (⑀) induced in the tissue during each loading cycle. The coefficients q and K would be different for each tissue and likely depend on age. The model does not consider repair rates or the time between exercise bouts. Repair could be expressed as a function of time and damage accumulation could be modeled if the BIOMECHANICAL PERSPECTIVES OF SPORTS INJURIES (1) where DF is a damage factor ranging from 0 to 1 (1 representing complete or 100% damage), N is the number of loading cycles during a bout of exercise, K is constant (approximately 6 ⫻ 1019 for cortical bone), q is constant (5 ⬍ q ⬍ 15), and ⑀ is strain in microstrain. Experimental studies need to be performed to establish the coefficients in equation 1, but clinical information is equally important for establishing the starting point for experimental studies directed in this area. Clinical observations that identify different modes of injury for different sporting activities or for different ages may provide the scientists with clues about how different tissues respond to different loading stimuli. For example, if children that perform relatively slow loading rate resistance training experience a high incidence of tendonitis injuries and children involved with kicking or throwing sports (faster loading rates) experience more apophysitis, then this might suggest that apophyses are more influenced by loading rate than are tendons. If the type of injuries experienced by long distance runners (e.g., stress fractures) and long distance swimmers (e.g., rotator cuff) are different, then this may provide clues about the interactions between loading magnitude, the number of loading cycles, and tissue injury. This information can help define tissue-specific coefficients in injury prediction models. SUMMARY Epidemiology data suggest that 9 million children will sustain preventable injuries this year. The annual cost to treat these injuries exceeds $1.8 billion. The long-term health and fitness ramifications of these injuries are not known, but reducing the incidence of these injuries is certainly desirable. A variety of biomechanical concepts have been presented to illustrate how biomechanics can be used to identify factors that contribute to overuse injuries in children and to identify information that is needed to develop reliable injury prevention guidelines for our youth. Limb length, mass, and moment of inertia increase during growth. These quantities interact but not necessarily in a linear manner. They affect limb dynamics and the muscle forces required to perform a movement task. Muscle strength increases during growth, but it may not increase in proportion to limb inertial properties. Joint flexibility may change during growth. This may indicate changes in tissue preloads. Reduced flexibility appears to be gender specific, occurring more in boys between 8 and 13 yr of age than in girls. Tissue loading depends on the dynamics of the movement; greater linear or angular accelerations lead to greater forces. Each child grows at his or her own rate, and individual responses should be considered when assessing a child’s risk for injury. Gross limb anthropometry, muscle strength, and joint flexibility are factors that can contribute to injury, but tissue mechanics also play an important role. Medicine & Science in Sports & Exercise姞 1705 Tissue structural and material properties change with maturation and training. Tissues become stronger but not necessarily at the same rate. During early stages of training, tendon and apophysis properties may lag behind muscle strength gains, causing asynchronous rates of strength gain. Tissue can accumulate damage during cyclic activities, but we do not know how easily different tissues are damaged by cyclic loading. Clinical evidence suggests that insertion sites are more easily damaged by cyclic loading compared with ligaments and tendons. There is considerable information that must be acquired and modeling approaches developed to formulate predictive models of injury mechanisms. This will involve collaborations between basic scientists, clinicians, athletes, and sports organizations. Ideally, extensive studies of the structural and material properties of functional units such as BLB and MTB will be performed to characterize the asynchronous rates of strength gain within these tissues as a function of age and altered activity level. Studies will be performed to characterize the injury response of tendons, bones, and ligaments to various loading stimuli (e.g., load magnitude, loading rate, number of loading cycles). Studies will characterize the damage repair rate of these tissues. These data will then be used to define the coefficients in tissue-specific injury prediction models. Biomechanical analysis techniques such as inverse dynamics and forward dynamics will be combined with appropriate musculoskeletal models to quantify the stresses and strains induced in specific tissues during various movement tasks. This approach will result in a powerful tool for identifying growth and movement related injury risk factors, and for prescribing safe movements and physical fitness training strategies for our youth. The material presented here represents a summary of material presented at the 19th Annual Meeting of the Southwest Chapter of the American College of Sports Medicine, November 12–13, 1999, San Jose, CA. Address for correspondence: Dr. David Hawkins, Exercise Biology Program, Room 275 Hickey Gym, University of California, Davis, Davis, CA 95616; E-mail: [email protected]. REFERENCES 1. AARON, D. J., and LAPORTE, R. E. Physical activity, adolescence, and health: an epidemiological perspective. In: Exercise and Sport Sciences Reviews, Vol. 25, J. O. Holloszy (Ed.). Baltimore: Williams & Wilkins, 1997, pp. 391– 406. 2. DALTON, S. E. Overuse injuries in adolescent athletes. Sports Med. 13:58 –70, 1992. 3. HAWKINS, D. A non-invasive approach for studying muscle-tendon interactions in-vivo. In: Skeletal Muscle Mechanics: From Mechanisms to Function, W. Herzog (Ed.). New York: John Wiley & Sons, 2000, pp. 305–326. 4. JENSEN, R. K. Growth of estimated segment masses between four and sixteen years. Hum. Biol. 59:173–189, 1987. 5. JENSEN, R., and G. NASSAS. Growth of segment principal moments of inertia between four and twenty years. Med. Sci. Sports Exerc. 20:594 – 604, 1988. 6. JóZSA, L., and P. KANNUS. Human Tendons: Anatomy, Physiology, and Pathology. Champaign, IL: Human Kinetics, 1997, pp. 98–111 and 178 –179. 7. LAROS, G. S., C. M. TIPTON, and R. R. COOPER. Influence of physical activity on ligament insertions in the knees of dogs. J. Bone Joint Surg. Am. 53:275–286, 1971. 8. MAFFULLI, N. Intensive training in young athletes: the orthopaedic surgeon’s viewpoint. Sports Med. 9:229 –243, 1990. 9. MALINA, R. M., and C. BOUCHARD. Growth, Maturation, and Physical Activity. Champaign, IL: Human Kinetics, 1991, pp. 128 –130 and 190 –193. 10. MARCHI, A. G., D. DI BELLO, G. MESSI, and G. GAZZOLA. Permanent sequelae in sports injuries: a population based study. Arch. Dis. Child. 81:324 –328, 1999. 11. MICHELI, L. J., and J. D. KLEIN. Sports injuries in children and adolescents. Br. J. Sports Med. 25:6 –9, 1991. 12. MICHELI, L. J., and A. F. FEHLANDT. Overuse injuries to tendons and apophyses in children and adolescents. Clin. Sports Med. 11:713–726, 1992. 13. NATIONAL YOUTH SPORTS SAFETY FOUNDATION. Did you know. Side Lines 9:2, 2000. 14. NOYES, F. R., P. J. TORVIK, W. B. HYDE, and J. L. DELUCAS. Biomechanics of ligament failure, II: an analysis of immobilization, exercise, and reconditioning effects in primates. J. Bone Joint Surg. Am. 56:1406 –1418, 1974. 15. NOYES, F. R. Functional properties of knee ligaments and alterations induced by immobilization: a correlative biome- 1706 Official Journal of the American College of Sports Medicine 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. chanical and histological study in primates. Clin Orthop. 123: 210 –242, 1977. ORAVA, S., and J. SAARELA. Exertion injuries to young athletes: a follow-up research of orthopaedic problems in young track and field athletes. Am. J. Sports Med. 6:68 –74, 1978. PARKER, D. F., J. M. ROUND, P. SACCO, and D. A. JONES. A cross-sectional study of upper and lower limb strength in boys and girls during childhood and adolescence. Ann. Hum. Biol. 17:199–211, 1990. SINCLAIR, D., and P. DANGERFIELD. Human Growth After Birth, 6th Ed. Oxford: Oxford University Press, 1998, pp. 24 –37. SNYDER, R., L. SCHNEIDER, C. OWINGS, H. REYNOLDS, D. H. GOLOMB, and M. A. SCHORK. Anthropometry of Infants, Children, and Youths to Age 18 for Product Safety Design. Bethesda, MD: U.S. Consumer Product Safety Commission. Report No. UMHsri-77–17, prepared by the Highway Safety Research Institute, University of Michigan, Ann Arbor, MI, 1977. STOUFFER, D. C., D. L. BUTLER, and D. HOSNY. The relationship between crimp pattern and mechanical response of human patellar tendon-bone units. J. Biomech. Eng. 108:158 –165, 1985. TANNER, J. M. Growth At Adolescence, 2nd Ed. Oxford: Blackwell Scientific Publications, Ltd., 1962, pp. 1–27. TIPTON, C. M., S. L. JAMES, W. MERGNER, and T.-K. TCHENG. Influence of exercise on strength of medial collateral knee ligaments of dogs. Am. J. Physiol. 218:894 –902, 1970. TIPTON, C. M., R. D. MATTHES, J. A. MAYNARD, and R. A. CARNEY. The influence of physical activity on ligaments and tendons. Med. Sci. Sports 7:165–175, 1975. TIPTON, C. M., R. D. MATTHES, and R. K. MARTIN. Influence of age and sex on the strength of bone-ligament junctions in knee joints of rats. J. Bone Joint Surg. Am. 60:230 –234, 1978. UNITED STATES DEPARTMENT OF COMMERCE. Current Population Reports: Population Projections of the United States by Age, Sex, Race, and Hispanic Origin, 1995–2050. Washington, DC: U.S. Government Printing Office, United States Department of Commerce, Economics and Statistics Administration, Bureau of the Census, Current Population Reports, 1996, p. 52. UNITED STATES DEPARTMENT OF HEALTH AND HUMAN SERVICES. Youth Risk Behavior Surveillance: United Stated 1997. Washington, DC: U.S. Government Printing Office, United States Department of Health and Human Services, Centers for Disease Control and Prevention, CDC Surveillance Summaries, MMWR, 1998; 47(No. SS-3), August 14, 1998. http://www.acsm-msse.org 27. UNITED STATES DEPARTMENT OF HEALTH AND HUMAN SERVICES. Youth Risk Behavior Surveillance: United Stated 1999. Washington, DC: U.S. Government Printing Office, United States Department of Health and Human Services, Centers for Disease Control and Prevention, CDC Surveillance Summaries, MMWR, 2000; 49(No. SS5), June 9, 2000. 28. WHITESIDE, J. A., J. R. ANDREWS, and G. S. FLEISIG. Elbow injuries in young baseball players. Physician Sportsmed. 27:87–102, 1999. 29. WOJTYS, E. M. Sports injuries in the immature athlete. Orthop. Clin. North Am. 18:689 –708, 1987. 30. WOO, S. L.-Y., M. A. GOMEZ, Y.-K. WOO, and W. H. AKESON. Mechanical properties of tendons and ligaments, II: the relationships of immobilization and exercise on tissue remodeling. Biorheology 19:397– 408, 1982. BIOMECHANICAL PERSPECTIVES OF SPORTS INJURIES 31. WOO, S. L.-.Y, C. A. ORLANDO, M. A. GOMEZ, C. B. FRANK, and W. H. AKESON. Tensile properties of the medial collateral ligament as a function of age. J. Orthop. Res. 4:133–141, 1986. 32. WOO, S. L.-Y., M. A. GOMEZ, T. J. SITES, P. O. NEWTON, C. A. ORLANDO, and W. H. AKESON. The biomechanical and morphological changes in the medial collateral ligament of the rabbit after immobilization and remobilization. J. Bone Joint Surg. Am. 69: 1200 –1211, 1987. 33. WOO, S. L.-Y., K. AN, S. P. ARNOCZKY, J. S. WAYNE, D. C. FITHIAN, and B. S. MEYERS. Anatomy, biology, and biomechanics of tendon, ligament, and meniscus. In: Orthopaedic Basic Science, S. Simon (Ed.). Rosemont, IL: American Academy of Orthopaedic Surgeons, 1994, pp. 45– 87. Medicine & Science in Sports & Exercise姞 1707