Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
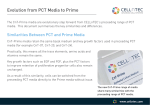
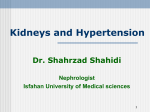
44. Chuang CH, Velott DL, Weisman CS. Exploring knowledge and attitudes relating to pregnancy and preconception health in women with chronic medical conditions. Matern Child Health J 2009; 14: 713–719 45. Giurgescu C, Penckoger S, Maurer MC et al. Impact of uncertainty, social support, and prenatal coping on the psychological well-being of high-risk pregnant women. Nurs Res 2006; 55: 356–365 46. Griffiths F, Lowe P, Boardman F et al. Becoming pregnant: exploring the perspectives of women living with diabetes. Br J Gen Pract 2008; 54: 184–190 47. EBPG. European best practice guidelines for renal transplantation. Section IV: long-term management of the transplant recipient. IV.10. Pregnancy in renal transplant recipients. Nephrol Dial Transplant 2002; 17: 50–55 48. Kasiske BL, Zeier MG, Chapman JR et al. KDIGO clinical practice guideline for the care of kidney transplant recipients: a summary. Kidney Int 2010; 77: 299–311 Received for publication: 13.10.2014; Accepted in revised form: 14.11.2014 Nephrol Dial Transplant (2015) 30: 661–666 doi: 10.1093/ndt/gfu273 Advance Access publication 20 August 2014 Antiproteinuric effect of add-on paricalcitol in Fabry disease patients: a prospective observational study Antonio Pisani1, Massimo Sabbatini1, Giovanni Duro2, Paolo Colomba2 and Eleonora Riccio1 Nephrology, Department of Public Health, University Federico II, Naples, Italy and 2Institute of Biomedicine and Molecular Immunology “A. MONROY”, National Research Council, Palermo, Italy Correspondence and offprint requests to: Eleonora Riccio; E-mail: [email protected] A B S T R AC T Background. Proteinuria is the predominant risk factor for renal disease progression in Fabry disease (FD). When urine protein excretion is controlled to <0.50 g/24 h, the rate loss of glomerular filtration rate (GFR) is not significantly different from 0. However, enzyme replacement therapy (ERT) alone does not decrease proteinuria and it has been recommended that patients receiving ERT also receive anti-renin–angiotensin system (RAS) therapy. Emerging evidence show that paricalcitol (PCT) reduces proteinuria in the presence of intensified inhibition of RAS; however, there is no evidence in FD. We evaluated the antiproteinuric effect of PCT in FD patients with proteinuria >0.50 g/24 h persisting despite ERT and anti-RAS therapy titrated to maximum tolerated dosage. Methods. Fifteen FD patients were selected and studied in the first 6 months of add-on oral PCT (1 µg/day) and, in order to verify the dependence of proteinuria reduction on PCT, 3 months after drug withdrawal. Results. At baseline, proteinuria was 1.3 ± 0.6 g/24 h. Six months of add-on PCT significantly decreased proteinuria to 0.4 ± 0.3 g/24 h, with levels <0.50 g/24 h achieved in four patients at Month 1, six at Month 3, and in 12 by Month 6, in the absence of changes to BP and GFR. Proteinuria recovered to basal value after drug withdrawal. © The Author 2014. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. Conclusions. In conclusion, our study is the first evidence that PCT is effective in reducing proteinuria in FD patients in the presence of ERT and anti-RAS therapy. Keywords: enzyme replacement therapy, Fabry disease, paricalcitol, proteinuria INTRODUCTION Fabry disease (FD) is an X-linked disorder caused by lysosomal α-galactosidase A deficiency, with subsequent deposition of undegraded glycosphingolipid products in multiple organs. Progressive nephropathy is one of the main features of FD [1]. The decline in renal function in FD is adversely affected by male gender, advanced chronic kidney disease (CKD), hypertension and, in particular, severe proteinuria. Studies of patients with FD have identified proteinuria as a major risk factor for renal disease progression. Therefore treatment of proteinuria is one of the goals in management of FD patients. When urine protein excretion is controlled to <0.50 g/24 h, the rate of loss of estimated glomerular filtration rate (eGFR) was not significantly different from 0 [2]. Currently, enzyme replacement therapy (ERT) is the only specific treatment for FD patients, which has been shown to slow the progression of Fabry nephropathy [3]. However, ERT alone does not appear to reduce proteinuria [4, 5] and it has been recommended that patients receiving ERT also receive 661 ORIGINAL ARTICLE 1 ORIGINAL ARTICLE angiotensin-converting-enzyme inhibitors or angiotensin receptor blockers (ACEi/ARBs). Multiple blockade of renin– angiotensin system (RAS) allows an additional decrement of proteinuria which is, however, still limited and heterogeneous, with many patients being left with significant residual proteinuria [6]; therefore, novel ways of proteinuria treatment are being studied. Recent studies have shown broad-ranging activities of vitamin D that extend beyond the regulation of calcium and phosphorus metabolism mediated by vitamin D receptor [7]. These so-called non-calcemic activities include regulation of renal and cardiovascular functions and modulation of immune responses. Several data have shown that paricalcitol (PCT) reduces proteinuria in several models of kidney disease, likely through the nuclear factor κB pathway and the RAS [8–12]. However, the effects of these strategies in patients with FD nephropathy are unknown. The aim of our study was to evaluate the effect of PCT on proteinuria in FD patients with proteinuria >0.5 g/24 h persisting despite the ERT and anti-RAS therapy titrated to maximum tolerated dosage. M AT E R I A L S A N D M E T H O D S Study population This is a prospective, observational study. Between December 2011 and December 2013, 49 patients with FD were seen at the Fabry Center of the Federico II University of Naples and considered for recruitment. The inclusion criteria were: (i) genetically proven FD, (ii) stable dose of ERT for at least 12 months, (iii) stable dose of ACEi or ARB titrated to maximum tolerated dosage for at least 6 months and (iv) persistent proteinuria >0.50 g/24 h despite the use of ERT and ACEi/ARBs in two consecutive samples within 12 weeks. Exclusion criteria were: steroid/immunosuppressive treatment, eGFR changes >30% in the past 3 months, parathormone (PTH) levels <20 pg/mL, serum phosphorus >5.0 mg/dL, serum calcium (adjusted for albumin) >10.0 mg/dL, active malignancy. On the basis of such criteria, 15 patients were enrolled in the study and written informed consent was obtained from all of them (Figure 1). The study was approved by the local medic ethics committee and was in adherence with the Declaration of Helsinki. Study procedures In patients identified by the inclusion criteria, data were collected at enrolment ( prior to ACEi/ARB maximum dosage therapy), at baseline ( prior to first administration of PCT), during administration of oral PCT (after 1, 3 and 6 months) and 3 months after PCT withdrawal. At baseline, 15 FD patients were selected and studied in the first 6 months of add-on oral PCT (1 µg/day) and, in order to verify the dependence of proteinuria reduction on PCT, 3 months after drug withdrawal. None of the patients had received a vitamin D analogue at least 1 month before beginning enrolment in the study. 662 F I G U R E 1 : Flow chart of patients selection. Intensification of anti-RAS therapy To achieve remission of proteinuria, anti-RAS therapy was titrated during enrolment to the full dose suggested by manufacturer’s recommendations, or at the highest tolerated dose ( presence of symptomatic hypotension, acute eGFR decrease >30% or serum potassium >5.5 mmol/L). The patients were first administered a single anti-RAS agent (either ACEi or ARB), opportunely titrated; if proteinuria still persisted above the target, ACEi with ARB were combined. In case of low blood pressure (BP) levels, antihypertensive drugs other than anti-RAS were downtitrated or eliminated. Add-on PCT PCT was administered at a dosage of 1 µg/day; this dosage was chosen as it is not associated with excessive decline of PTH levels in most patients [9, 11]. Data collection Demographic and clinical data were obtained at baseline (Tables 1 and 2). At each control a complete clinical evaluation was performed, including body weight, BP and adjustments of therapy. Moreover, we evaluated 24-h urinary proteins, and in venous plasma or serum the following chemistries: creatinine, calcium, phosphate, albumin and PTH. Renal function was expressed as eGFR, calculated with Modification of Diet in Renal Disease equation. Standard laboratory procedures were used for blood and urinary measurements. Urine collections were considered inaccurate, and repeated, if the value of measured creatinine excretion rate fell outside the normal range. Statistics Variables are reported as mean and standard deviation (SD) or as median and interquartile range. Means are A. Pisani et al. Table 1. Main characteristics of patients at enrolment Age (years) Gender (M/F) ERT (agalsidase alfa/beta) Body mass index (kg/m2) Diabetes (%) 25-OH-Vitamin D (ng/mL) eGFR (mL/min/1.73 m2) Serum albumin (g/dL) Proteinuria (g/24 h) Systolic BP (mmHg) Diastolic BP (mmHg) Antihypertensive drugs (n) Anti-RAS per patient (n) 42.7 ± 10.5 8/7 7/8 28.2 ± 7.4 7 22.17 ± 11.2 79.5 ± 25 4.1 ± 0.4 2.1 ± 0.6 124 ± 8 74 ± 8 1.1 ± 0.6 0.7 ± 0.5 Data are expressed as mean ± SD. ERT, enzyme replacement therapy; eGFR, estimated glomerular filtration rate; BP, blood pressure; Anti-RAS, angiotensin-converting enzyme or angiotensin receptor blockers. compared by paired or unpaired Student t-test and McNemar or chi-square test for categorical variables. ANOVA for repeated measures with Bonferroni as post hoc test are also used where appropriate. A two-tailed P-value of <0.05 is considered significant. Data are analysed using SPSS 20.0 (SPSS, Inc., Chicago, IL, USA). Data at enrolment We studied 15 patients identified by the inclusion criteria (Tables 2 and 3). At time of enrolment (9 months prior to study baseline), the median age for the eight men and the seven women was 42.7 ± 10.5 years. Eight families with distinct mutations were represented; the clinical manifestations were different, with multiple organ involvement in addition to Fabry nephropathy (Table 2). All patients were treated with a stable dose of ERT for at least 12 months. Eight patients were treated with agalsidase beta and seven with agalsidase alfa, and the mean duration of ERT was 72.1 ± 36.8 months (median 60 months). Most patients were on antihypertensive therapy before Data at baseline At baseline, the mean number of antihypertensive drugs was 1.7 ± 0.7. The increase in number of BP lowering drugs, observed at baseline versus enrolment visit, was due to the larger use of anti-RAS agents. At baseline, in fact, all patients were treated with anti-RAS therapy at full dose: nine patients were under multiple blockade of RAS, and the remaining six were under a single anti-RAS agent. Intensification of RAS therapy was also obtained in these six patients administered a single anti-RAS agent; at enrolment, in fact, these drugs were not used in five patients or used at low dosage in the remaining patients, while at baseline all patients were treated with RAS blockers at full dose. In these six patients, combined therapy was considered unfeasible because adding the second antiRAS agent had been associated with hypotension (n = 5) and hyperkalaemia (n = 1). Intensification of RAS was associated with a significant decrease in proteinuria (1.34 ± 0.6 mg/24 h, P < 0.001 versus enrolment), which still remained >0.5 g/24 h, and of BP (108/63 ± 6/4 mmHg, P < 0.001 versus enrolment), without changes in GFR (P = 0.3) (Table 3). Data at follow-up As reported in Table 4, add-on PCT was associated with a progressive decline in PTH levels that, however, did not decrease below the lower limit of normal range (20 pg/mL) in any patient. Serum calcium and phosphate remained within normal range in all patients (Tables 3 and 4). Add-on PCT induced a progressive decrease of proteinuria to 0.4 ± 0.3 g/24 h (P < 0.001) (Table 4). The individual values at enrolment, at baseline and at the end of follow-up period are shown in Table 3 and in Figure 2. Remission of proteinuria to values <0.5 g/24 h was achieved in four patients at Month 1 (26.7%), six at Month 3 (40%) and in 12 at Month 6 (80%). The mean reduction of proteinuria after 6 months of PCT was 68%. No correlation was found between percentage change in proteinuria, BP and eGFR (r = 0.16, P = 0.34). Table 2. Genetic and clinical characteristics of the patients at enrolment ID Age (gender) Family group (mutation) Clinical manifestations of FD ERT (Mo) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 45 (M) 53 (F) 54 (F) 32 (M) 36 (F) 49 (M) 18 (M) 52 (F) 53 (M) 36 (F) 32 (M) 33 (M) 44 (F) 51 (F) 53 (M) 1 (c.1066C>T) 2 (p.R35W) 3 (c.901C>T) 3 (c.901C>T) 1 (c.1066C>T) 4 (p.A288D) 5 (IVS4+5G>T) 6 (c.740G>A) 4 (p.A288D) 1 (c.1066C>T) 7 (c.680G>C) 2 (p.R35W) 1 (c.1066C>T) 8 (c.1133C>G) 1 (c.1066C>T) ACR; CKD LVH ANG, CKD ACR, ANG, LVH ACR, CKD ACR, ANG, CAD, CKD, CVA, LVH LVH CAD, CKD, LVH ACR, ANG, CAD, CVA, LVH CAD, CKD, LVH ACR, LVH ACR, ANG, CW, LVH CKD, LVH ANG, CKD, CVA, LVH ACR, LVH Agalsidase alfa (61) Agalsidase beta (20) Agalsidase beta (108) Agalsidase beta (108) Agalsidase alfa (55) Agalsidase beta (57) Agalsidase alfa (41) Agalsidase beta (131) Agalsidase alfa (50) Agalsidase alfa (60) Agalsidase alfa (121) Agalsidase beta (17) Agalsidase beta (58) Agalsidase alfa (132) Agalsidase beta (63) ACR, acroparesthesias; ANG, angiokeratomas; CAD, coronary artery disease; CKD, chronic kidney disease; CVA, cerebrovascular accident; CW, corneal whirls; LVH, left ventricular hypertrophy. Paricalcitol in Fabry disease 663 ORIGINAL ARTICLE R E S U LT S enrolment; the mean number of antihypertensive drugs was 1.1 ± 0.6; ACEi/ARBs, however, were not used in five patients or used at low dosage in the remaining 10 patients (Table 3). Table 3. Individual modifications of proteinuria, glomerular filtration rate (eGFR), use of angiotensin-converting-enzyme inhibitor (ACEi), angiotensin receptor blocker (ARB) and blood pressure (BP) during the different phases of the study ID Enrolment 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 a Baseline Final visit Withdrawal Proteinuria (g/24 h) eGFR (mL/ min) BP Antihypertensive (mmHg) drugsa (ACEi/ ARBs) Proteinuria (g/24 h) eGFR (mL/ min) BP Proteinuria (mmHg) (g/24 h) eGFR (mL/ min) BP Proteinuria (mmHg) (g/24 h) eGFR (mL/ min) BP (mmHg) 2.1 2.4 1.4 2.7 0.7 2.5 1.4 2.1 1.9 2.3 2.3 1.7 1.7 3.6 2.5 73 90 52 101 68 61 135 70 96 69 93 105 50 34 95 120/80 120/70 120/80 130/80 100/60 130/80 125/80 130/80 135/80 120/60 120/70 130/70 120/60 130/70 130/85 1.2 1.6 0.6 2 0.8 2 0.6 1.3 1.3 1.4 1.4 0.9 0.9 2.8 1.3 70 93 50 104 67 60 138 68 94 69 92 103 48 34 94 110/70 110/60 105/70 115/70 100/60 120/65 110/70 110/70 115/60 105/55 100/60 110/55 100/50 115/60 120/70 70 91 51 106 67 61 137 67 93 68 90 103 51 36 93 100/65 110/65 100/65 115/70 105/65 120/60 100/65 110/65 110/60 110/55 100/70 105/60 105/60 115/60 115/65 68 91 50 104 67 63 137 66 94 68 91 105 50 35 93 105/70 110/65 105/65 110/70 100/65 120/65 115/70 110/60 105/65 110/60 100/70 100/55 100/60 120/60 120/65 2 (2) 1 (1) 2 (2) 1 (1) 1 (1) 3 (2) 1 (1) 2 (2) 2 (2) 2 (2) 1 (1) 2 (2) 3 (2) 2 (2) 1 (1) 0.4 0.6 0 1 0 0.4 0.2 0.5 0.3 0.4 0.5 0.2 0.2 1 0.4 1.1 2 0.6 1.8 0.8 1.9 0.6 1.2 1.1 1.3 1.4 1 1 2.4 1.4 Numbers in brackets refer to number of ACEi and/or ARBs at patients’ highest tolerated doses. ORIGINAL ARTICLE Table 4. Overall changes of main clinical and laboratory data before PCT treatment (enrolment, baseline), during PCT treatment (Month 1–6) and 3 months after PCT withdrawal SBP/DBP (mmHg) eGFR (mL/min/1.73 m2) PTH (pg/mL) ALP (U/L) Serum calcium (mg/dL) Serum phosphorus (mg/dL) Proteinuria (g/24 h) Enrolment Baseline Month 1 Month 3 Month 6 Withdrawal 124 ± 8/74 ± 8 79.5 ± 25 74 ± 21 85 ± 33 9.2 ± 0.7 3.9 ± 0.6 2.1 ± 0.6 110 ± 6/63 ± 6b 78.9 ± 26 72 ± 25 84 ± 31 9.3 ± 0.6 3.9 ± 0.7 1.3 ± 0.6b 112 ± 9/64 ± 7 79.2 ± 25.4 67 ± 22a 77 ± 35 9.3 ± 0.6 3.9 ± 0.8 0.9 ± 0.4a 110 ± 9/64 ± 8 78.7 ± 24.2 54 ± 21a 73 ± 21 9.4 ± 0.5 4.0 ± 0.7 0.7 ± 0.4a 108 ± 6/63 ± 4 78.9 ± 25.2 45 ± 19a 67 ± 17 9.4 ± 0.4 4.0 ± 0.7 0.4 ± 0.3a 109 ± 7/64 ± 4 78.8 ± 25.6 61 ± 23a 71 ± 19 9.4 ± 0.3 4.0 ± 0.7 1.3 ± 0.5 Data are expressed as means ± SD. SBP/DBP, systolic/diastolic blood pressure; eGFR, estimated glomerular filtration rate; PTH, parathormone; ALP, alkaline phosphatase. a Significantly different versus baseline (P < 0.05, minimum value). b Significantly different versus enrolment (P < 0.05, minimum value). The first dose of PCT (1 µg/day) did not change throughout the 6 months of follow-up in all the patients. Data after PCT withdrawal To verify the dependence of proteinuria reduction on PCT, we evaluated the change of proteinuria 3 months after drug withdrawal. In all the patients, proteinuria recovered to baseline (Tables 3 and 4 and Figures 2 and 3). DISCUSSION This study has shown that treatment with 1 µg PCT significantly reduces proteinuria in patients with FD nephropathy who were on a stable dose of ACEi and/or ARBs titrated to maximum tolerated dosage. Early observational studies of vitamin D supplementation in patients have indicated the capacity of activators of the vitamin D receptor (VDRA) to decrease proteinuria (range 17–61%) in a number of kidney disease, irrespective of the level of renal insufficiency (stage 2–5), of its primary diagnosis 664 and of the previous or concomitant use of anti-RAS agents [8–12]. Of note, higher doses of PCT (2 versus 1 µg/day) in diabetic CKD patients further decreased urinary protein excretion with no additional metabolic or clinical side effects, suggesting the possibility of safely increasing PCT doses, if needed. However, the exact effect of PCT in patients with FD nephropathy was undefined. The presence of proteinuria >0.5 g/24 h identifies a subgroup of FD patients which carries the highest risk of renal disease progression. In these patients, minimizing RAS activity is a main target of treatment. Moreover, recent evidence highlighted the very high prevalence of vitamin D insufficiency and deficiency in FD patients [13]. In fact, due to symptoms such as heat intolerance and the inability to sweat, Fabry patients tend to avoid sunlight exposure. Often, patients also suffer from malabsorptive gastrointestinal disease. Both conditions may contribute to a deficiency in vitamin D. It has been recently evidenced, moreover, that vitamin D deficiency is strongly associated with cardiomyopathy and adverse clinical symptoms in FD patients [14]. A. Pisani et al. F I G U R E 2 : Proteinuria levels for individual patients at enrolment, before (baseline), after 1-, 3- and 6-month add-on PCT (T1, T3 and T6, respectively), and after 3-month drug withdrawal. Each patient is shown as an individual regression line. evidence that low-dose PCT, given in the absence of exogenous calcium loading, is not associated to excessive suppression of bone turnover [19]. Interpretation of results is limited by the small sample size and the absence of control group; nevertheless, the remarkable antiproteinuric response and the recovery of proteinuria to baseline after 3 months of drug withdrawal support the validity of our observations. Regarding the recovery of proteinuria after drug withdrawal, however, we cannot exclude some degree of escape of proteinuria which is not an uncommon finding when inhibition of RAS is intensified [20, 21]. Furthermore, more prolonged follow-up is required to verify efficacy and safety of this approach over the long term. Finally, we did not assess systemic RAS activity. In conclusion, our study suggests that, in patients with FD and persisting proteinuria despite ERT and maximal tolerated anti-RAS therapy, add-on PCT safely allows a reduction of proteinuria with a remarkable achievement of levels <0.5 g/24 h in more than two-thirds of cases. PCT therefore represents a potential additional therapeutic option to be considered when intensified anti-RAS treatment is not completely efficacious or unfeasible because of adverse effects. Whether the antiproteinuric effect of PCT translates into improvement of prognosis of these high-risk patients is worth investigating. None declared. F I G U R E 3 : Proteinuria levels measured in patients before (baseline), after add-on PCT (Month 6), and after 3-month drug withdrawal. Data are mean ± SD. VDRAs appear to mediate antiproteinuric effects by several mechanisms. First, in cultured human podocytes, VDRA prevented lyso-Gb-3-induced, TGFβ1-mediated, up-regulation of extracellular matrix proteins [15]. Experimental studies have shown that vitamin D acts as a strong negative endocrine regulator of the RAS and functions mainly to suppress renin production [14]. Therefore, the effects on RAS inhibition represent an important target in the treatment of patients with FD nephropathy. Nonetheless, our data show that RAS inhibition in our patients was not optimal, since its maximization determined a significant decrease in urinary protein excretion; this strongly suggests that medical intervention in these patients should be more aggressive. Another important conclusion of our study is that PCT does not affect BP; this means that the reduction of proteinuria is not BP dependent. The significant antiproteinuric effect of PCT was not impaired by major adverse effects, thus extending to this subgroup of high-risk and poly-treated patients the favourable safety profile of PCT previously reported [8–12, 16–18]. PTH and alkaline phosphatase (ALP) remained in the normal range in most patients. This finding supports the experimental Paricalcitol in Fabry disease REFERENCES 1. Pisani A, Visciano B, Imbriaco M et al. The kidney in Fabry’s disease. Clin Genet 2014; 86: 301–309 2. Tahir H, Jackson LL, Warnock DG. Antiproteinuric therapy and Fabry nephropathy: sustained reduction of proteinuria in patients receiving enzyme replacement therapy with agalsidase-beta. J Am Soc Nephrol 2007; 18: 2609–2617 3. Pisani A, Visciano B, Roux GD et al. Enzyme replacement therapy in patients with Fabry disease: state of the art and review of the literature. Mol Genet Metab 2012; 107: 267–275 4. Banikazemi M, Bultas J, Waldek S et al. Agalsidase-beta therapy for advanced Fabry disease: a randomized trial. Ann Intern Med 2007; 146: 77–86 5. West M, Nicholls K, Mehta A et al. Agalsidase alfa and kidney dysfunction in Fabry disease. J Am Soc Nephrol 2009; 20: 1132–1139 6. Kunz R, Friedrich C, Wolbers M et al. Meta-analysis: effect of monotherapy and combination therapy with inhibitors of the rennin-angiotensin system on proteinuria in renal disease. Ann Intern Med 2008; 148: 30–48 7. Nagpal S, Na S, Rathnachalam R. Noncalcemic actions of vitamin D receptor ligands. Endocr Rev 2005; 26: 662–687 8. Agarwal R. Vitamin D, proteinuria, diabetic nephropathy, and progression of CKD. Clin J Am Soc Nephrol 2009; 4: 1523–1528 9. de Zeeuw D, Agarwal R, Amdahl M et al. Selective vitamin D receptor activation with paricalcitol for reduction of albuminuria in patients with type 2 diabetes (VITAL study): a randomised controlled trial. Lancet 2010; 376: 1543–1551 10. Alborzi P, Patel NA, Peterson C et al. Paricalcitol reduces albuminuria and inflammation in chronic kidney disease: a randomized double-blind pilot trial. Hypertension 2008; 52: 249–255 11. Fishbane S, Chittineni H, Packman M et al. Oral paricalcitol in the treatment of patients with CKD and proteinuria: a randomized trial. Am J Kidney Dis 2009; 54: 647–652 665 ORIGINAL ARTICLE C O N F L I C T O F I N T E R E S T S TAT E M E N T 17. Agarwal R, Acharya M, Tian J et al. Antiproteinuric effect of oral paricalcitol in chronic kidney disease. Kidney Int 2005; 68: 2823–2828 18. Cheng J, Zhang W, Zhang X et al. Efficacy and safety of paricalcitol therapy for chronic kidney disease: a meta-analysis. Clin J Am Soc Nephrol 2012; 7: 391–400 19. Slatopolsky E, Cozzolino M, Lu Y et al. Efficacy of 19-Nor-1,25-(OH)2D2 in the prevention and treatment of hyperparathyroid bone disease in experimental uremia. Kidney Int 2003; 63: 2020–2027 20. Müller DN, Luft FC. Direct renin inhibition with aliskiren in hypertension and target organ damage. Clin J Am Soc Nephrol 2006, 1: 221–228 21. Velez JC. The importance of the intrarenal renin-angiotensin system. Nat Clin Pract Nephrol 2009; 5: 89–100 Received for publication: 23.4.2014; Accepted in revised form: 6.7.2014 ORIGINAL ARTICLE 12. De Nicola L, Conte G, Russo D et al. Antiproteinuric effect of add-on paricalcitol in CKD patients under maximal tolerated inhibition of reninangiotensin system: a prospective observational study. BMC Nephrology 2012; 13: 150 13. Drechsler C, Schmiedeke B, Niemann M et al. Potential role of vitamin D deficiency on Fabry cardiomyopathy. J Inherit Metab Dis. 2014; 37: 289–295 14. Freundlich M, Quiroz Y, Zhang Z et al. Suppression of rennin-angiotensin gene expression in the kidney by paricalcitol. Kidney Int 2008; 74: 1394–1402 15. Sanchez-Niño MD, Sanz AB, Carrasco S et al. Globotriaosylsphingosine actions on human glomerular podocytes: implications for Fabry nephropathy. Nephrol Dial Transplant 2011; 26: 1797–1802 16. Agarwal R. Are vitamin D receptor agonists like angiotensin-converting enzyme inhibitors without side effects? Kidney Int 2010; 77: 943–945 666 A. Pisani et al.