Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
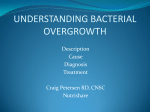
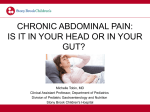
MGI Newsletter A Fresh Look at Breath Testing at MGI Vol. No. 4 Thomas R. McGinn, MD, FACP In This Issue... Breath Hydrogen New Physician Dr. Marc Scheer MGI's Newest Physician Quick Links MGI Home Page Our Locations Our Services MGI Support Groups Gas, bloating and abnormal bowel movements are common symptoms that motivate patients to see a gastroenterologist. The list of conditions that can cause these symptoms is extensive. Common disorders that may present with these symptoms include irritable bowel syndrome, celiac disease, carbohydrate malabsorption, and small intestinal bacterial overgrowth. A carefully performed history and physical exam and a few diagnostic tests can usually lead the clinician and patient to a diagnosis. Dr. Thomas R. McGinn One type of diagnostic study that MGI gastroenterologists are now performing in their office is hydrogen breath (H2B) testing. H2B tests measure the concentration of hydrogen and methane in the air we breathe out. The only source of hydrogen and methane in the exhaled breath is from gut bacteria metabolizing carbohydrates we ingest. H2B tests are especially helpful in diagnosing two types of disorders that can present as gas and bloating: carbohydrate malabsorption (ex. lactase deficiency) and bacterial overgrowth of the small bowel. A review of the pathophysiology of each of these conditions will help illustrate how hydrogen breath testing works. Normal human digestion is very efficient in absorbing protein and fat. Carbohydrate absorption is more variable and may result in unabsorbed carbohydrates reaching the colon where they undergo fermentation by colonic bacteria. The gas and liquid products of fermentation result in the symptoms of gas, bloating and diarrhea. Carbohydrates such as lactose, fructose and sorbitol have been extensively studied in functional bowel disorders, and their malabsorption may result in symptoms. H2B testing can be performed to assess for malabsorption of each of these sugars. Lactose, found in milk, is a disaccharide composed of galactose and glucose. It is digested by lactase which is found on the lining of the small bowel. Lactose malabsorption is common and is due to a lack of this enzyme. Because lactose is not absorbed, it passes through to the colon where through increased liquid and gas production, it causes symptoms of lactose intolerance. The most common test available today to diagnose lactose malabsorption is the lactose hydrogen breath test. In this test, a patient ingests 25 gm of lactose and end expiratory breath is sampled every 60 minutes for 3 hours, and the hydrogen concentration is measured. An abnormal test will result in a rise in breath hydrogen of 20 parts per million over baseline (Figure 1). This abnormal rise occurs because the malabsorption of lactose leads to more of the sugar getting to the colon and the bacteria that normally reside there. The same principle is utilized in testing for fructose and sorbitol malabsorption. At Midwest GI, the breath tests are performed by Theresa Link, RD, a registered dietitian with expertise in gastrointestinal nutrition. If carbohydrate malabsorption is identified, Theresa is able to give patients detailed dietary recommendations that can greatly lessen their symptoms. Figure 1 H2 breath testing can also help diagnose small intestinal bacterial overgrowth (SIBO). SIBO is a condition caused by an abnormal number of bacteria in the small intestine. Patients with this Page 1 of 2 condition may experience diarrhea, bloating, gas. SIBO has been found in a significant number of patients who previously had been diagnosed with irritable bowel syndrome. Finding treatable components of irritable bowel syndrome is a therapeutic goal for clinicians and patients. SIBO, if found, may offer a different treatment option. Small intestinal bacterial overgrowth is also a cause of malabsorption in the elderly and in patients with small intestinal conditions that result in stasis, which promotes the overgrowth of bacteria. In these conditions, weight loss and malnutrition may occur. The concentration of bacteria in the GI tract increases over its distance. The stomach is almost sterile, and the number of bacteria in the small bowel is small. Where the small bowel and the colon meet, a barrier called the ileocecal valve acts to keep bacteria in the colon from migrating up the small bowel. Normal gut motility also plays a role in keeping the small intestine relatively bacteria free. Testing for bacteria in the small intestine is difficult. Culturing fluid from the jejunum and small intestine is cumbersome and not very accurate. SIBO can be diagnosed indirectly relatively simply using H2 breath testing. In this test, a patient ingests a 10 gm. lactulose drink. Lactulose is used because it is not absorbed, and it is metabolized by gut bacteria into H2 or methane. Exhaled breath is then collected every 30 minutes for 3 hours and analyzed for H2 and methane. Under normal conditions, it takes about 90-120 minutes for the lactulose to make its way to the colon. Once in the colon, the breath H2 will rise. In SIBO, the rise in breath H2 is much earlier, classically followed by a second rise as the ingested lactulose gets to the colon (Figure 2). Up to 30% of the cases of SIBO are due to bacteria that produce methane; therefore, both gases are measured in the exhaled breath. Because this is an indirect test and many factors can affect the test results, false positive or false negative results can occur. The interpretation of the test results has to be incorporated into the overall clinical assessment. SIBO is a treatable condition. Ideally, a nonabsorbable antimicrobial agent is used to eliminate the offending gut bacteria. Often, a single course of oral antibiotics in the case of SIBO or a modest dietary change in the case of carbohydrate malabsorption can improve a patient's problem with chronic gas, bloating and abnormal bowel movements. Figure 2 Introducing Dr. Marc A. Scheer August 2012, Marc A. Scheer, DO became the newest addition to our team of GI Specialists. Dr. Scheer completed his Gastroenterology Fellowship at the University of Nebraska Medical Center. Click here to read more about Dr. Marc Scheer and all the physicians of MGI. Forward this email This email was sent to [email protected] by [email protected] | Update Profile/Email Address | Instant removal with SafeUnsubscribe™ | Privacy Policy. MGI | 8901 Indian Hills Drive | Omaha | NE | 68114 Page 2 of 2