Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
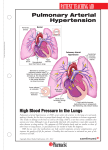
FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 2 Pulmonary Arterial Hypertension (PAH) FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 3 Contents 1. Introduction 3 2. What is PAH? 4 3. Classification of PAH 5 4. How is PAH severity classified? 7 5. How common is PAH? 7 6. Why does PAH develop? 8 7. What are the symptoms of PAH? 9 8. Early diagnosis and intervention is crucial 9 9. How is PAH diagnosed? 10 10. Screening in PAH: key to early diagnosis 12 11. Echocardiography – value as a screening tool 13 12. Right heart catheterisation – the diagnostic gold standard 14 13. Assessing PAH: 6-minute walk test – an evaluation of exercise capacity 15 14. How is PAH treated? 16 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 3 1. Introduction Pulmonary arterial hypertension (PAH) is a serious disease of the arteries connecting the heart to the lungs (the pulmonary arteries). As PAH develops, blood flow through the pulmonary arteries is restricted and the right side of the heart is put under increasing strain to pump blood through to the lungs. This leads to the main symptoms of PAH – breathlessness, chest tightness limited exercise capacity and fatigue. Untreated, PAH is a disease with a very poor prognosis. The early symptoms of PAH (such as breathlessness, chest tightness and fatigue) can be mild and are common to many other conditions. Reaching the diagnosis can be delayed and as a consequence patients with PAH may first present when the disease has already progressed. This brochure explains how PAH develops, describes the symptoms associated with this disease and outlines how it can be diagnosed and treated. Treatment is aimed at improving symptoms, exercise tolerance, long-term outcomes and quality of life. Until the mid-1980s there were limited treatment options for patients and PAH was associated with poor prognosis. Today, treatment options have improved the prognosis for patients with this condition. 3 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 4 2. What is PAH? Pulmonary Arterial Hypertension (PAH) is a syndrome characterised by a progressive increase in pulmonary vascular resistance leading to right ventricular overload and eventually to right ventricular failure and premature death.1 The increase in pulmonary vascular resistance is related to a number of progressive changes in the pulmonary arterioles, including: • • • • Vasoconstriction Obstructive remodelling of the pulmonary vessel wall through proliferation in the various layers of the blood vessel wall (smooth muscle cell and endothelial cell proliferation) Inflammation In-situ thrombosis The main histological features include medial hypertrophy, intimal thickening, adventitial thickening, plexiform lesions and in-situ thrombosis (Figure 1). The plexifom lesion represents a focal proliferation of endothelial and smooth muscle cells and is pathognomonic of PAH. PAH is defined as a sustained elevation of mean pulmonary arterial pressure to more than 25 mmHg at rest or to more than 30 mmHg while exercising, with a normal pulmonary wedge pressure (≤15 mmHg).2 In most cases the earliest symptom is dyspnoea on physical exertion. Other symptoms include syncope or near syncope, fatigue and peripheral oedema.3,4 Chest tightness and pain similar to angina may occur, particularly on physical exertion. Figure 1. 4 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 5 3. Classification of PAH Pulmonary Arterial Hypertension (PAH) represents Group 1 within the Pulmonary Hypertension WHO clinical classification system (Venice 2003 revision) and is one of five such groups. The groups are divided based on aetiology.5 Group I. Pulmonary arterial hypertension (PAH) • Idiopathic (IPAH) • Familial (FPAH) • Associated with (APAH): – Connective tissue disease – Congenital systemic-to-pulmonary shunts – Portal hypertension – HIV infection – Drugs and toxins – Other (thyroid disorders, glycogen storage disease, Gaucher’s disease, hereditary haemorragic telangiectasia, haemoglobinopathies, myeloproliferative disorders, splenectomy) • Associated with significant venous or capillary involvement – Pulmonary veno-occlusive disease (PVOD) – Pulmonary capillary haemangiomatosis (PCH) • Persistent pulmonary hypertension of the newborn (PPHN) Group II. Pulmonary hypertension associated with left heart diseases Group III. Pulmonary hypertension associated with respiratory diseases and/or hypoxemia (including chronic obstructive pulmonary disease) Group IV. Pulmonary hypertension due to chronic thrombotic and/or embolic disease Group V. Miscellaneous group • eg. sarcoidosis, histiocytosis X and lymphangiomatosis Idiopathic PAH (IPAH), which by definition has no identifiable underlying cause, is one of the more common types of PAH. Familial PAH (FPAH) accounts for at least 6% of cases of IPAH and mutations in the bone morphogenetic protein receptor 2 (BMPR2) have been identified in the majority of cases of FPAH.6,7 PAH can also be associated with a number of conditions (Associated Pulmonary Arterial Hypertension – APAH), which together account for most other cases of PAH. These conditions include: 1. Connective Tissue Diseases • including systemic sclerosis (scleroderma) and systemic lupus erythematosus (SLE) 2. Congenital Heart Disease • including Eisenmenger’s syndrome 3. Human immunodeficiency virus (HIV) infection 4. Sickle Cell Disease 5 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 6 PAH is also a rare side effect of certain anorexigenic agents, such as fenfluramine and dexfenfluramine. However, the incidence of drug-induced PAH is decreasing as these agents are no longer available. 1. PAH associated with connective tissue disease PAH is a well-recognised complication of connective tissue diseases such as systemic sclerosis and SLE and in affected patients may also occur in association with interstitial lung disease. The prevalence of PAH in patients with systemic sclerosis has been reported to be up to 16%8 and in systemic sclerosis patients, pulmonary complications, such as interstitial lung disease and PAH, are now the leading causes of death. Patients with PAH associated with systemic sclerosis have a particularly poor prognosis compared to those with systemic sclerosis without PAH.9 2. PAH associated with congenital heart disease Congenital heart disease is relatively common, affecting around 1% of the population. Within this population 15% will go on to develop PAH.10 As determined by the level of pulmonary vascular resistance, the most severe form of PAH is Eisenmenger’s syndrome, which is associated with the reversal of an initial left to right shunt causing cyanosis and limited exercise capacity.11 3. PAH associated with HIV infection PAH is a rare (estimated prevalence in patients with HIV: 0.5%)12 but relatively well-documented complication of HIV infection. With the advent of highly active anti-retroviral therapy (HAART) and markedly improved survival, PAH and other non-infectious manifestations of HIV infection are increasingly responsible for HIV-associated morbidity and poor prognosis. In patients with HIV, the HIV-1 envelope glycoprotein GP120 may stimulate the production of endothelin by macrophages.13 HIV-associated PAH shows a similar clinical picture to IPAH and seems to be independent of the degree of immunosuppression. 4. PAH associated sickle cell disease Sickle cell disease (SCD) is a genetic disorder of the haemoglobin which results in a chronic haemolytic anaemia. Over time and due to the chronic haemolysis the vasculature becomes damaged and pulmonary hypertension can develop. The prevalence of PAH in sickle cell patients is 20–40%.14 The two year mortality rate of pulmonary hypertension related to SCD is reported up to 50% and is one of the leading causes of death in SCD.15 6 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 7 4. How is PAH severity classified? PAH is usually classified according to a functional class system initially devised by the New York Heart Association (NYHA) for Chronic Heart Failure and then adapted for PAH by the World Health Organisation (WHO). WHO functional class (WHO FC) measures the severity of PAH and reflects the impact on a patient’s life in terms of physical activity and symptoms. There are four classes; class I being the least severe and class IV being the most advanced (Table 1).4 Table 1. Class Symptomatic profile Class I Patients with pulmonary hypertension but without resulting limitation of physical activity. Ordinary physical activity does not cause dyspnoea or fatigue, chest pain or near syncope. Class II Patients with pulmonary hypertension resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnoea or fatigue, chest pain or near syncope. Class III Patients with pulmonary hypertension resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes undue dyspnoea or fatigue, chest pain or near syncope. Class IV Patients with pulmonary hypertension with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. Dyspnoea and/or fatigue may even be present at rest. Discomfort is increased by any physical activity. 5. How common is PAH? Although PAH is a rare disease, with an estimated prevalence of 30–50 cases per million,16 the prevalence of PAH in certain at-risk groups is substantially higher. For example, in HIV-infected patients the prevalence is 0.5%,12 in patients with sickle cell disease the prevalence is 20–40%14 and in patients with systemic sclerosis the prevalence has been reported to be up to 16%.8 Idiopathic PAH is more common in young women with a mean age of diagnosis of 36 years.3 However it can occur at any age.3 Idiopathic PAH is twice as common in women as in men.3 Although the true relative prevalence of IPAH, FPAH and APAH are unknown, it is likely that IPAH accounts for at least 40% of cases, and APAH for most of the remaining cases.17 Due to the non-specific nature of the symptoms, PAH is most frequently diagnosed when patients have reached a more advanced stage of disease (WHO Functional Class III and IV),17 suggesting that the true prevalence may be higher than documented in the literature. 7 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 8 6. Why does PAH develop? The exact cause behind the development of PAH remains unknown. However, research has led to a better understanding of the underlying mechanisms. PAH is recognised as a complex, multi-factorial condition involving numerous biochemical pathways and different cell types. Endothelial dysfunction is believed to occur early on in disease pathogenesis, leading to endothelial and smooth muscle cell proliferation and structural changes or ‘remodelling’ of the pulmonary vascular bed resulting in an increase in pulmonary vascular resistance. Vascular remodeling itself involves all layers of the vessel wall and is characterised by proliferative and obstructive changes involving many cell types, including endothelial, smooth muscle and fibroblasts. Inflammatory cells and platelets may also play a significant role in PAH. Endothelial cell dysfunction results in reduced production of vasodilators,such as nitric oxide (NO) and prostacyclin, and over production of vasoconstrictors, such as thromboxane A2 and endothelin-1 (ET-1). ET-1, NO and prostacyclin have been the principal focus of research into new treatment options for patients with PAH. Endothelin Endothelin is produced by the endothelial cells and is essential for maintenance of normal vascular tone and function. However, high levels of endothelin are seen in patients with PAH due to various aetiologies18–20 and correlate with disease severity,21 resulting in a number of detrimental effects, primarily in the vasculature:3 • • • Fibrosis Hypertrophy and proliferation of cells, which can lead to thickening, narrowing and occlusion of blood vessels Inflammation • Vasoconstriction Endothelin binds to 2 receptors, ETA and ETB. Both receptors are implicated in PAH and mediate the deleterious effects of endothelin.22 Endothelin receptor antagonism can either mitigate the effects of only one (single ETA antagonist) or both (dual ETA and ETB receptor antagonist) receptor types. Prostacyclin Prostacyclin is a potent vasodilator as well as an inhibitor of platelet activation. It is believed that patients with PAH have low levels of prostacyclin, which could result in vasoconstriction in the pulmonary vasculature and a tendency for smooth muscle cell proliferation and platelet activation, encouraging the formation of thrombi in both the micro-circulation and the pulmonary arteries.23–25 Therapy with synthetic forms of prostacyclin can help to correct this deficiency, although administering this form of treatment is complex.26–28 8 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 9 Nitric oxide Nitric oxide is an endothelial-derived substance that, like prostacyclin, is a potent vasodilator and also possesses anti-proliferative properties. PAH patients appear to produce insufficient NO and this may contribute to the development of PAH.3 The vasodilatory effect of NO is mediated by cGMP, which is rapidly degraded by phosphodiesterases. The inhibition of the degradation of cGMP with phosphodiesterase 5 inhibitors promotes the accumulation of intracellular cGMP, resulting in vasodilatation.29 7. What are the symptoms of PAH? The changes to the pulmonary vasculature described above lead to the typical symptoms of PAH. The symptoms are caused by the high resistance to blood flow through the lungs and result in increased stress on the heart. This can severely impact the ability to exercise or carry out normal daily activities. Common early symptoms include:3,4 • • • • • • Breathlessness (dyspnoea), particularly on physical activity Fatigue Dizziness Syncope, also on physical activity (rare) Peripheral oedema Chest pain, again particularly during physical activity The symptoms may not be obvious at first and are often attributed to more common conditions such as asthma, general fatigue, or lack of physical fitness. Over time, however, they can become more severe and begin to limit normal activities. As the disease progresses, some patients may experience constant dyspnoea and fatigue so that even simple tasks such as getting dressed and walking short distances become difficult. 8. Early diagnosis and intervention is crucial Early diagnosis and intervention is important in PAH as without treatment the median survival of patients is 2.8 years, which is comparable with some malignancies.30–32 However, diagnosis is complex and can be delayed for months or even years as early PAH symptoms are mild and non-specific. This means that PAH is frequently not recognised until the disease is relatively advanced.3 In fact, the average time from onset to diagnosis is estimated to be approximately 2 years.17 Although patients progress at different rates, mildly symptomatic PAH patients still have a devastating condition, which can progress rapidly. Recognising and treating PAH early is therefore crucial to changing the course of the disease. Marked improvements in prognosis and survival have been shown for patients who begin targeted therapy in less severe stages of PAH (WHO FCI/II) compared with those in a more severe stage (WHO FCIII/IV).33 9 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 10 9. How is PAH diagnosed? The non-specific nature of symptoms associated with PAH means that the diagnosis cannot be made on symptoms alone. A series of investigations is required to make an initial diagnosis, to refine that diagnosis in terms of clinical class of pulmonary hypertension and to evaluate the degree of functional and haemodynamic impairment (Figure 2). Consequently, it can be useful to adopt a four stage approach: 1. Clinical suspicion of pulmonary hypertension • • • Breathlessness (dyspnoea) without overt signs of specific heart or lung disease Screening of patients with associated conditions (Connective Tissue Disease, Congenital Heart Disease, HIV, Sickle Cell Disease) Incidental findings on examination for other clinical reasons 2. Detection of pulmonary hypertension • • • ECG (echocardiogram) Doppler echocardiogram (Figure 2) Chest radiograph, may show evidence of cardiomegaly and enlarged pulmonary arteries (Figure 3) 3. Identify other causes of pulmonary hypertension • • • • Pulmonary function tests (PFTs) and arterial blood gas samples Ventilation and perfusion lung scan High resolution computed tomography (HRCT) Pulmonary angiography 4. PAH evaluation and classification (type, functional capacity, haemodynamics) • • • 10 Blood tests and immunology, HIV test, abdominal ultrasound scan 6 minute walk test (6-MWT) and peak VO2 Right heart catheterisation and vasoreactivity testing FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 11 Figure 2. Figure 3. 11 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 12 10. Screening in PAH: key to early diagnosis The key to early diagnosis is introducing screening for high risk patient populations if they are asymptomatic. High risk patient populations include: • • • • Family members of a patient with familial Pulmonary Arterial Hypertension (FPAH) Patients with systemic sclerosis (SSc) Patients with HIV Patients with portopulmonary hypertension (PoPH) The results of a disease registry in France indicated that without screening, the majority of patients were diagnosed in a more severe stage of PAH (WHO FC III/IV), and only 25% of patients were in early stage PAH (WHO FC I/II).17 Furthermore, the results of a French national screening program in a high-risk population indicated that it is possible to detect Pulmonary Arterial Hypertension (PAH) in an earlier stage in a high-risk population34 (Figure 4). International guidelines now recommend annual screening high-risk groups with Doppler echocardiography.2,8,35 Doppler echocardiography is currently the most effective method for screening, however, for a definitive diagnosis right heart catheterisation has to be performed. Figure 4. No screening17 12 With screening34 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:17 Page 13 11. Echocardiography – value as a screening tool Transthoracic Doppler-echocardiography (TTE) is a non-invasive screening test for pulmonary arterial hypertension. TTE is able to estimate pulmonary arterial systolic pressure, which is equivalent to right ventricular systolic pressure in the absence of pulmonary outflow obstruction. It can provide additional information about the cause and consequences of PH, including right and left ventricular dimensions and function, heart valve abnormalities, right ventricular ejection and left ventricular filling characteristics and presence of a pericardial effusion. In the initial investigation of patients with PAH it is important to obtain adequate images of the right heart. Pulmonary arterial pressure can be estimated from the tricuspid regurgitant (TR) jet (Figure 5). Figure 5. 13 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:17 Page 14 12. Right heart catheterisation – the diagnostic gold standard Right heart catheterisation is required for a definitive diagnosis of PAH (Figure 6 and 7)3,4 to assess the severity of haemodynamic impairment and to test the vasoreactivity of the pulmonary circulation. The following parameters should always be assessed: right atrial pressure (RAP), pulmonary arterial pressure (PAP [systolic, diastolic and mean]), pulmonary capillary wedge pressure (PCWP), cardiac output/index, pulmonary (PVR) and systemic vascular resistance, blood pressure and arterial and mixed venous oxygen saturation. PAH is defined as a sustained elevation of mean pulmonary arterial pressure to >25 mmHg at rest or to >30 mmHg while exercising, with a mean pulmonary wedge pressure or left ventricular end-diastolic pressure of ≤15 mmHg and pulmonary vascular resistance of ≥3 woods units.2 A positive vasoreactive response is defined as a reduction in mean pulmonary artery pressure (mPAP) ≥10 mmHg to reach an absolute value of mPAP ≤40 mmHg with an increase or unchanged cardiac output. A positive response is shown in only 10–15% of patients, and sustained response is shown in even fewer (less than 7%).1 Figure 6. 14 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:17 Page 15 Figure 7. 13. Assessing PAH: 6-minute walk test – an evaluation of exercise capacity In patients with PAH, the 6-MWT to evaluate exercise capacity is reflective of activities of daily living;36 the distance a PAH patient can walk in 6 minutes is a critical endpoint in studies evaluating the benefit of different therapeutic options. To allow meaningful comparisons, it is important that the 6-MWT be performed under supervision according to a standardised protocol.37 • • • • • • • A 30 m corridor should be available, marked at 3 m intervals The patient should rest for at least 10 minutes prior to the test and should not have performed any rigorous exercise within the previous 2 hours The patient should be asked to rate their baseline dyspnoea The patient should be instructed to walk to their maximum capacity but not to run or jog; they should be permitted to rest as necessary The supervisor should count each lap as the patient finishes it The patient should be asked to rate their dyspnoea at the end of the test The test should be repeated at approximately the same time of day on each occasion 15 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:17 Page 16 14. How is PAH treated? There is currently no cure for PAH but advances in understanding how the disease develops (see section: Why does PAH develop?) means that there are now treatments available which have helped to improve prognosis for patients with this disease. Prognosis is influenced by the status of WHO FC when treatment is started – patients who start therapy in functional class I or II demonstrate a better prognosis than those whose therapy is started in more severe stages (WHO FC III or IV).33 Early treatment may delay disease progression By recognising and treating patients as early as possible, disease progression may be delayed. Without treatment, patients in WHO FC II can rapidly deteriorate within 6 months to more advanced Pulmonary Arterial Hypertension (PAH) as evidenced by progression of symptoms.38 Treatment options have progressed considerably in the last decade, especially those which target the underlying mechanisms of the disease. The main medical treatment options for patients with PAH are:39 Treatments that are routinely used but with little evidence of a positive impact on the disease progression • • • • 16 Anticoagulants, such as warfarin, to address the observed thrombotic changes and potential predisposition in the pulmonary microcirculation for in-situ thrombosis Calcium-channel blockers (CCBs). Less than 10% of IPAH patients benefit from CCB therapy. This figure is even lower in other forms of PAH. If not used in appropriate candidates (patients with demonstrated vasoreactivity during right heart catheterisation), CCBs can decrease cardiac output and systemic vascular resistance without any improvement in PAP and PVR and therefore may be deleterious1 Diuretics, for treatment of right heart failure Oxygen therapy, to maintain oxygen saturation at >90% at all times FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:17 Page 17 Treatments that have been specifically studied in PAH • • • Endothelin receptor antagonists – endothelin is implicated in the pathogenesis of PAH through actions on the pulmonary vasculature. Endothelin is found to be elevated in patients with PAH and levels of endothelin are directly related to disease severity and prognosis. Endothelin receptor antagonists (ERAs) are oral treatments that either block the ETA receptor alone or both the ETA and ETB receptors22 Phosphodiesterase 5 inhibitors – oral agents which induce relaxation and antiproliferative effects on vascular smooth muscle cells by preventing the reduction in levels of cGMP29 Prostacyclin analogues – may be delivered by continuous intravenous or subcutaneous infusion or via an intermittent nebuliser39 In very severe cases surgical options may be considered: • • Balloon atrial septostomy Heart and lung transplantation However, the use of transplantation is constrained by the limited number of donor organs. 17 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:17 Page 18 References 1. Sitbon O, Humbert M, Jaïs X et al. Long-term response to calcium channel blockers in idiopathic pulmonary arterial hypertension. Circulation 2005; 111: 3105–3111. 2. Galiè N, Torbicki A, Barst RJ, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension: The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension of the European Society of Cardiology. Eur Heart J 2004; 25: 2243–2278. 3. Gaine SP, Rubin LJ. Primary Pulmonary Hypertension. Lancet 1998; 352: 719−725. 4. Barst RJ, McGoon M, Torbicki A et al. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2004; 43(Suppl S): 40S–47S. 5. Simonneau G, Galiè N, Rubin LJ et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004; 43(Suppl S): 5S−12S. 6. Lane KB, Machado RD, Pauciulo MW et al. Heterozygous germline mutations in BMPR2, encoding a TGFbeta receptor, cause familial primary pulmonary hypertension. The International PPH Consortium. Nat Genet 2000; 26(1): 81–84. 7. Deng Z, Morse JH, Slager SL et al. Familial primary pulmonary hypertension (gene PPH1) is caused by mutations in the bone morphogenetic protein receptor-II gene. Am J Hum Genet 2000; 67(3): 737–744. 8. McGoon M, Gutterman D, Steen V et al. Screening, early detection, and diagnosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004; 126(1 Suppl) :14S−34S. 9. Koh ET, Lee P, Gladman DD, Abu-Shakra M. Pulmonary hypertension in systemic sclerosis: an analysis of 17 patients. Br J Rheumatol 1996; 35(10): 989–993. 10. Beghetti M, Barst RJ, Naeije R, Rubin LJ. Pulmonary arterial hypertension related to congenital heart disease. Elsevier 2006. 11. Diller GP, Dimopoulos K, Okonko D et al. Exercise intolerance in adult congenital heart disease: comparative severity, correlates, and prognostic implication. Circulation 2005; 112(6): 828–835. 12. Sitbon O, Lascoux-Combe C, Delfraissy JF et al. Prevalence of HIV-related pulmonary arterial hypertension in the current antiretroviral therapy era. AJRCCM 2008; 177: 108–113. 13. Sitbon O, Gressin V, Speich R et al. Bosentan for the treatment of human immunodeficiency virusassociated pulmonary arterial hypertension. Am J Respir Crit Care Med 2004; 170(11): 1212–1217. 14. Lin EE, Rodgers GP, Gladwin MT. Hemolytic anemia-associated pulmonary hypertension in sickle cell disease. Curr Hematol Rep. 2005; 4(2): 117–125. 15. Castro, O. Hoque M, Brown B.D. Pulmonary hypertension in sickle cell disease: cardiac catheterisation results and survival. Blood 2003; 101: 1257–1261. 16. Peacock AJ. Treatment of pulmonary hypertension. BMJ 2003; 326: 835–836. 17. Humbert M, Sitbon O, Chaouat A et al. Pulmonary Arterial Hypertension in France: Results from a National Registry. Am J Respir Crit Care Med 2006; 173(9): 1023–1030. 18. Stewart DJ, Levy RD, Cernacek P et al. Increased plasma endothelin-1 in pulmonary hypertension: marker or mediator of disease? Ann Inter Med 1991; 114: 464–469. 19. Vancheeswaran R, Magoulas T, Efrat G et al. Circulating endothelin-1 levels in systemic sclerosis subsets-a marker of fibrosis or vascular dysfunction? J Rheum 1994; 21: 1838–1844. 20. Yoshibayashi M, Nishioka K, Nakao K et al. Plasma endothelin concentrations in patients with pulmonary hypertension associated with congenital heart defects. Evidence for increased production of endothelin in pulmonary circulation. Circulation 1991; 84: 2280–2285. 18 FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:17 Page 19 21. Galie N, Grigioni F, Bacchi-Reggiani L et al. Relation of endothelin-1 to survival in patients with primary pulmonary hypertension. Eur J Clin Inves 1996; 26: A48. 22. Channick RN, Simonneau G, Sitbon O et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 2001; 358: 1119–1123. 23. MacGreggor AJ, Canavan R, Knight C et al. Pulmonary hypertension in systemic sclerosis: risk factors for progression and consequences for survival. Rheumatology (Oxford) 2001; 40(4): 453–459. 24. Loyd JE, Butler MG, Foround TM et al. Genetic anticipation and abnormal gender ratio at birth in familial primary pulmonary hypertension. Am J Respir Crit Care Med 1995; 152: 93–97. 25. Rubin LJ. Therapy of pulmonary hypertension: the evolution from vasodilators to antiproliferative agents. Am J Respir Crit Care Med 2002; 166: 1308–1309. 26. Ono F, Nagaya N, Okamura H et al. Effect of orally active prostacyclin analogue on survival in patients with chronic thromboembolic pulmonary hypertension without major vessel obstruction. Chest 2003; 123: 1583–1538. 27. Galie N, Manes A, Branzi A. Emerging medical therapies for pulmonary arterial hypertension. Prog Cardiov Dis 2002: 45: 213–224. 28. Clapp LH, Finney P, Turcato S et al. Differential effects of stable prostacyclin analogs on smooth muscle proliferation and cyclic AMP generation in human Pulmonary artery. Am J Resp Cell Mol Biol 2002; 26: 194–201. 29. Galiè N, Ghofrani HA, Torbicki A et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med 2005; 353: 2148–2157. 30. D'Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991; 115: 343–349. 31. Kato I, Severson RK and Schwartz AG. Conditional median survival of patients with advanced carcinoma: surveillance, epidemiology, and end results data. Cancer 2001; 92: 2211–2219. 32. Bjoraker JA, Ryu JH, Edwin MK, et al. Prognostic significance of histopathologic subsets in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1998; 157: 199–203. 33. Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002; 40: 780–788. 34. Hachulla E, Gressin V, Guillevin L, et al. Early detection of pulmonary arterial hypertension in systemic sclerosis: a French nationwide prospective multicenter study. Arthritis Rheum 2005; 52: 3792–3800. 35. Hachulla E and Coghlan JG. A new era in the management of pulmonary arterial hypertension related to scleroderma: endothelin receptor antagonism. Ann Rheum Dis 2004; 63: 1009–1014. 36. Solway S, Brooks D, Lacasse Y, Thomas S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest 2001; 119(1): 256–270. 37. ATS. ATS statement: guidelines for the 6-minute walk test. Am J Respir Crit Care Med 2002; 166: 111–117. 38. Galiè N, Rubin LJ, Hoeper MM et al. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet 2008; 371: 2093–2100. 39. Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med 2004; 351: 1425–1436. FCII_disease_brochure_aw.qxd:FCII_disease_brochure_aw 26/9/08 15:16 Page 1 For further information visit www.pah-info.com © 2008 Actelion Pharmaceuticals Ltd. Gewerbestrasse 16 – CH-4123 Allschwil – Switzerland – www.actelion.com 08 382 01 00 0908