Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
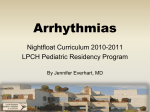
J.N. Wang, J.M. Wu, Y.C. Tsai, et al ECTOPIC ATRIAL TACHYCARDIA IN CHILDREN Jieh-Neng Wang, Jing-Ming Wu, Yu-Chien Tsai,1 and Chia-Shiang Lin Background and purpose: Ectopic atrial tachycardia (EAT) is an unusual and potentially risky arrhythmia that can result in left ventricular dysfunction if not properly managed. In adults, EAT is mainly caused by diseased atrial myocardium and responds poorly to antiarrhythmic drugs. The characteristics of EAT in children might be different from those in adults because of their immature myocardium and the different electrophysiologic characteristics of their conduction tissue. We examined the natural history and treatment of EAT in children. Methods and results: From June 1990 through June 1999, 24 children (8 girls and 16 boys; median age 4 mo [1 d–10 yr]) were admitted to our hospital with a diagnosis of EAT. Fifteen had healthy hearts, six had congenital heart disease, one had myocarditis, one had bronchopulmonary dysplasia with severe pulmonary hypertension, and one had hypertrophic cardiomyopathy. Thirteen patients presented with congestive heart failure. Only four patients had symptoms of prodromal airway infection. The maximum atrial rate was 244 ± 66 beats per minute. Atrioventricular block was documented at least once during tachycardia in 10 patients. Warm-up or cool-down phenomenon was seen at the initiation or termination of tachycardia in thirteen patients. Primary pharmacologic treatment was attempted in all patients. EAT was initially controlled in all patients using digoxin plus propranolol (18 patients), propranolol only (4), or digoxin plus procainamide (2). EAT was controlled using medication in 22 patients. Fifteen patients had sinus rhythm but did not receive medication for 39 ± 25 months. Two patients died of uncontrolled arrhythmia, and two of underlying disease. Recurrence was seen within 3 months after initial therapy in five patients. Surgery was performed to correct the underlying heart disease in three patients with frequently recurring EAT, all of whom remained tachycardia-free after surgery, without pharmacologic treatment. The spontaneous remission rate was 75% (18/24). Conclusion: EAT in children without underlying heart disease can be effectively treated using antiarrhythmic drugs. Spontaneous resolution of EAT after medication in children was frequent (75%) in this series. The results of this study suggest that a step-wise approach using digoxin, a beta-blocker, and a class I antiarrhythmic drug may be the most effective treatment for EAT. Ectopic atrial tachycardia (EAT) is an uncommon arrhythmia that occurs mostly in young children [1, 2]. Timely recognition of EAT is important because it can cause tachycardia-induced cardiomyopathy [3, 4]. Despite the fact that the clinical and electrophysiologic features of this arrhythmia have been extensively investigated [5, 6], little is known about the natural history of the disease, particularly in terms of spontaneous remission [7, 8]. (J Formos Med Assoc 2000;99:766–70) Key words: ectopic atrial tachycardia child In adults, EAT is known to be caused mainly by diseased atrial myocardium and local degenerative processes that do not regress, and patients with EAT respond poorly to antiarrhythmic drugs [8]. In children, the relatively immature myocardium and electrophysiologic characteristics of conduction tissue might indicate a different etiology and treatment response. Few reports of follow-up studies in children with EAT have shown resolution of the tachycardia after initial drug treatment [1, 2, 7, 8]. 1 Department of Pediatrics, National Cheng Kung University Hospital, Tainan; and Department of Pediatrics, Tainan Municipal Hospital, Tainan. Received: 24 December 1999. Revised: 1 March 2000. Accepted: 11 April 2000. Reprint requests and correspondence to: Dr. Jing-Ming Wu, Department of Pediatrics, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, 138 Sheng-Li Road, Tainan, Taiwan. 766 J Formos Med Assoc 2000 • Vol 99 • No 10 Ectopic Atrial Tachycardia in Children Because of the paucity of data on the long-term effectiveness of pharmacologic and non-pharmacologic therapies, management strategies in patients with this type of tachycardia are not well defined. The purpose of this study was to examine the natural history of the disease, the effectiveness of treatment, and the findings of clinical follow-up in children with EAT. Materials and Methods From June 1990 through June 1999, 24 consecutive patients treated in the National Cheng Kung University Hospital who were under the age of 15 years at the time of diagnosis of EAT were included in this study. Detailed clinical history and physical examination results were obtained on admission. Chest radiography, echocardiography, 12-lead electrocardiography (ECG), and 24-hour Holter monitor examinations were performed. EAT was diagnosed if patients met any one of the following three criteria: wide range of atrial heart rate during tachycardia with or without abnormal P wave morphology; tachycardia with ‘warm-up’ and/or ‘cooldown’ phenomenon; or second-degree atrioventricular block without interruption of the atrial rhythm [1]. According to the findings of continuous ECG monitoring during admission or 24-hour ambulatory Holter monitoring, the tachycardia was further classified as incessant if it was present for more than 90% of the time, or as repetitive if it was frequently interrupted by short sequences of sinus rhythm recurring constantly during the day [2]. Congestive heart failure was assumed to be present when the cardiothoracic ratio on the chest radiograph was at least 0.55 and/or the left ventricular ejection fraction on two-dimensional echocardiography was 50% or less, combined with clinical symptoms and signs of heart failure [9]. Patients with hypertrophic cardiomyopathy and patients without obvious congestive heart failure were initially treated with a beta-blocking agent alone. In patients with transposition of the great arteries after Senning operation, both digoxin and procainamide were used. In other patients, digoxin was used first; a beta-blocking agent and procainamide were added if the rate of the EAT was not under control. Tachycardia was considered to be under control if the minimum, average, and maximum heart rates were within the reference range for the patient’s age and no significant periods of second-degree atrioventricular block during antiarrhythmic therapy were observed. The tachycardia was considered to be in spontaneous remission if no arrhythmia was observed after medication had been discontinued for at least 6 months [7]. J Formos Med Assoc 2000 • Vol 99 • No 10 Results The study group consisted of 24 children (8 girls and 16 boys) with a median age of 4 months (range, 1 d to 10 yr) (Table 1). Fetal arrhythmia was recognized in one patient at the gestational age of 32 weeks but was not treated during pregnancy. Tachycardia occurred soon after birth in this patient. Fifteen of the 24 patients had healthy hearts, six had congenital heart disease (3 developed EAT after cardiac surgery), one had myocarditis, one had bronchopulmonary dysplasia with severe pulmonary hypertension, and one had hypertrophic cardiomyopathy. Thirteen of the 24 patients presented with congestive heart failure, and four patients had prodromal signs of upper respiratory tract infection. EAT was incessant in 10 and repetitive in 14 patients. Nine of the 10 patients with incessant EAT were symptomatic, while only four of the 14 patients with repetitive EAT had symptoms. Symptoms consisted of tachypnea and feeding problems in infants and toddlers, while school-aged children experienced fatigue and exercise intolerance. The ECG characteristics, mode of EAT, and presence of congestive heart failure in the study patients are summarized in Table 2. The maximal atrial rate of EAT ranged from 166 to 300 beats per minute, with a median of 244 beats per minute. Warm-up and/or cool-down phenomenon was observed during tachycardia in 13 patients, and abnormal P waves were found in 18 patients. Second-degree atrioventricular block was found in 13 patients, only four of whom had congestive heart failure. The flow diagram of our treatment protocol is shown in the Figure. Both digoxin (10–20 µg⋅kg–1⋅d–1) and propranolol (3–6 mg⋅kg–1⋅d–1) were used in the 18 patients with mild to moderate congestive heart failure at the time of initial treatment. Four of these patients died within 1 to 2 months: two patients died of uncontrollable EAT that caused the underlying cardiopulmonary function to deteriorate (1 with myocarditis and 1 with bronchopulmonary dysplasia); and two patients died of unrelated diseases (1 of asplenic syndrome with complex heart disease and 1 of interrupted aortic arch with ventricular septal defect). In the remaining 14 patients, digoxin and propranolol treatment was effective in 13 and ineffective in one. Procainamide (15–40 mg⋅kg –1⋅d–1) was added to this patient’s treatment protocol to control his EAT. EAT recurred after discontinuing medication for 1 to 3 months in three patients, who reverted to sinus rhythm after restarting digoxin and propranolol. However, EAT was only partially controlled in two of these three patients. In one patient with underlying heart 767 J.N. Wang, J.M. Wu, Y.C. Tsai, et al Table 1. Clinical characteristics of children with ectopic atrial tachycardia Sex F F M M F M M M M M M F F F M M M M M M M M F F Age 1 1 1 7 1 1 1 2 2 2 3 4 4 6 7 9 18 21 29 30 6 6 8 10 d d d d mo mo mo mo mo mo mo mo mo mo mo mo mo mo mo mo years years years years CHF URI Underlying disease Drugs Outcome – – + – – + + – + – + – – + + + + – + + + + – – – – – – – – – – – – + – – – – – – + + – – – – – – – – – – – HCM – VSD, interrupted aortic arch – Myocarditis – ASD II Right isomerism – – BPD, severe PAH – PA, intact IVS s/p TGA s/p Senning TGA s/p Senning – – – D, I D, I D, I I D, I D, I I D, I, P D, I I D, I D, I D, I D, I D, I D, I D, I D, I D, I D, P, I D, P, I D, I D, I I SR SR SR SR SR SR Continued treatment SR Died SR Died SR SR Died SR SR Died SR SR SR SR SR SR Continued treatment CHF = congestive heart failure; URI = upper respiratory tract infection; D = digoxin; I = propranolol; SR = spontaneous remission; HCM = hypertrophic cardiomyopathy; P = procainamide; VSD = ventricular septal defect; ASD = atrial septal defect; BPD = bronchopulmonary dysplasia; PAH = pulmonary hypertension; PA = pulmonary atresia; IVS = interventricular septum; s/p = post operative; TGA = transposition of great arteries. disease (pulmonary atresia with intact ventricular septum after Brock’s procedure), balloon dilation was performed because of severe residual pulmonary stenosis. EAT was not observed again in this patient during 2 years of follow-up. In two patients with severe congestive heart failure, both of whom had transposition of the great arteries after Senning operation, digoxin and procainamide were started. Because EAT could only be partially controlled, propranolol was added later to the treatment of both patients. Because of marked right atrial chamber dilation due to severe tricuspid valve regurgitation, both of these patients received mechanical valve replacement. EAT was not observed again in these two patients after surgery, during 15 to 19 months’ followup, even after discontinuing drugs. In four patients without heart failure, we used propranolol to control EAT. It was fully effective in three and partially effective in one. Two patients were symptom-free and propranolol was discontinued 3 months after initiation in these patients. Propranolol treatment was continued in one patient because of hypertrophic cardiomyopathy. The remaining patient received medication during 16 months of follow-up. 768 Overall, antiarrhythmic drugs were successful in controlling EAT in 22 of the 24 patients. During the follow-up period of 43 ± 31 (mean ± standard deviation) months (range, 13 mo to 8 yr), 18 of the 24 patients had spontaneous remission. Discussion Even though EAT may present at any age, it is predominantly seen in young infants and children [1, 2]. In this study, 16 of 24 patients were under 1 year of age at the time of diagnosis. Seven newborns were noted to have tachycardia within 1 month after birth, but fetal arrhythmia was found in only one patient. Although no association between EAT and congenital heart disease has been previously reported [2], the incidence of congenital heart disease was 25% in this series. Donnerstein et al suggested that respiratory syncytial virus infection can trigger EAT [10]. In our series, only four patients had prodromal signs of upper respiratory tract infection, but no virus was identified. Although the exact pathogenic mechanism of EAT J Formos Med Assoc 2000 • Vol 99 • No 10 Ectopic Atrial Tachycardia in Children Table 2. Electrocardiographic characteristics, mode of ectopic atrial tachycardia (EAT), and presence of congestive heart failure (CHF) in children with EAT Age Abnormal P wave Mode of EAT Warm up or cool down 2nd degree AVB Max atrial rate, bpm CHF 1 day 1 day 1 day 7 days 1 month 1 month 1 month 2 months 2 months 2 months 3 months 4 months 4 months 6 months 7 months 9 months 18 months 21 months 29 months 30 months 6 years 6 years 8 years 10 years + – + – + + + – + + + – + + + + + – + + + + + + Repetitive Incessant Incessant Repetitive Repetitive Incessant Incessant Repetitive Incessant Repetitive Incessant Repetitive Repetitive Repetitive Incessant Incessant Incessant Repetitive Repetitive Repetitive Incessant Repetitive Repetitive Repetitive – – + – – + + + – – + – – – + – + + – + + + + + + + – + – – – + + + – + + + – + – + – – – + + – 250 300 197 210 250 200 210 200 214 250 270 200 210 214 250 210 239 210 300 200 210 200 166 220 – – + – – + + – + – + – – + + + + – + + + + – – AVB = atrioventricular block; bpm = beats per minute. EAT (n = 24) ECG, CXR, Holter, Echocardiography (CHF) D+P (n = 2) (no CHF) D+I (n = 18*) I (n = 4) Clinical follow-up 1–3 months EAT (+) (n = 2) EAT (+) (n = 1) EAT (-) (n = 13) EAT (-) (n = 3) EAT(+) (n = 1) DC drug Subsided Recurrence (n = 10) (n = 3) D+I+P (n = 3) D+I (n = 3) Surgery DC drug (n = 2) (n = 1) Surgery (n = 1) Subsided Continued drug (n = 2) (n = 2) DC drug (n = 1) Continued drug (n = 1) Figure. Flow diagram of treatment protocol and patient follow-up. EAT = ectopic atrial tachycardia; ECG = electrocardiogram; CXR = chest radiograph; CHF = congestive heart failure; D = digoxin; I = propranolol; DC = discontinued; P = procainamide. *Four patients died within 1 to 2 months. J Formos Med Assoc 2000 • Vol 99 • No 10 is uncertain, warm up at tachycardia onset and cool down during the termination stage strongly suggests that this is an automatic arrhythmia [1, 2, 9]. In our study, this phenomenon was observed in 54% of patients. As noted by Mehta et al, the upper right atrium appears to be the most common site of origin of EAT [2]. In this setting, differentiation from sinus tachycardia can be difficult. Therefore, spontaneous episodes of second-degree atrioventricular block during tachycardia provide a critical clue for the diagnosis of EAT [1]. In our study, 54% of patients exhibited this diagnostic evidence. The results of this study suggest that the majority of children with EAT may be treated conservatively using drugs only. Although digoxin alone may slow down the heart rate [11], it has not been useful in controlling EAT [2, 4, 8, 9]. However, digoxin may be beneficial in temporarily managing coexisting heart failure. Because EAT is most often caused by an abnormal automaticity mechanism, which is a catecholamine-sensitive tachycardia, beta-receptor blocking agents are usually tried in children, with varying degrees of success [2, 11–13], especially in young infants [2]. Beta-blocking agents are usually given in combination with digoxin to counteract its negative inotropic effect, which might be 769 J.N. Wang, J.M. Wu, Y.C. Tsai, et al detrimental in patients with EAT and evidence of left ventricular dysfunction [9]. Class IA antiarrhythmic agents, particularly quinidine and procainamide, are known to prolong atrial refractory periods and suppress automaticity; however, neither of these agents was successful in suppressing EAT in various studies reported in the literature [2, 11]. In our study, we also found partial control with the use of procainamide. The class III antiarrhythmic agent amiodarone has been reported to be the most effective drug in treating children with EAT [2, 8, 12]. However, the value of amiodarone is somewhat limited by the frequency of undesired side-effects [9]. None of our patients underwent catheter or surgical ablation of the ectopic focus, although surgery was performed in three patients to correct the underlying cardiac disease. After the procedure, the dilated cardiac chambers regressed in these patients and EAT was not observed during the follow-up period of 15 to 24 months. Although chronic tachycardia has sometimes been associated with signs and symptoms of heart failure mimicking dilated cardiomyopathy [1, 2, 4], the pathophysiologic link between chronic incessant tachycardia and ventricular dysfunction is not clear [4]. It is possible that chronic tachycardia and heart failure may be interrelated, and that control of one may help control the other. Spontaneous remission of EAT during long-term follow-up was not uncommon in our series. Many researchers also emphasize that EAT can disappear spontaneously [1, 2, 7, 8]. This may explain why EAT is only rarely diagnosed in adults. Klersy et al found that the age at onset of arrhythmia was the single covariate able to independently predict the possibility of remission [7]. The higher rate of spontaneous remission among younger patients suggests that immature cardiac tissue or an inflammatory process with subsequent healing may be responsible for the rhythm disorder in this age group [7]. In older patients, EAT may be caused by a local degenerative process that does not regress, and therefore does not allow spontaneous remission and displays poor control [7]. On the basis of our findings, we suggest antiarrhythmic drug therapy for children with EAT. Beta-blocking agents were effective in the control of EAT in children in this series. For EAT patients who respond poorly to beta-blocking agents, other drugs such as class I or class III antiarrhythmic agents or radiofrequency ablation could be used as alternative treatments. Because our study was retrospective and not placebo controlled, we cannot exclude the possibility of spontaneous EAT 770 resolution in some patients whose EAT was believed to have been controlled with drugs, especially in view of the high resolution rate. ACKNOWLEDGMENT: We are grateful to Professor Ming-Lon Young (University of Miami) for reviewing this manuscript. References 1. Koike K, Hesslein PS, Finlay CD, et al: Atrial automatic tachycardia in children. Am J Cardiol 1988;61:1127–30. 2. Mehta AV, Sanchez GR, Sacks EJ, et al: Ectopic automatic atrial tachycardia in children: clinical characteristics, management and follow up. J Am Coll Cardiol 1988;11: 379–85. 3. Garson A Jr, Gillette PC, McNamara DG: Supraventricular tachycardia in children: clinical features, response to treatment, and long-term follow-up in 217 patients. J Pediatr 1981;98:875–82. 4. Packer DL, Bardy GH, Worley SJ, et al: Tachycardiainduced cardiomyopathy: a reversible form of left ventricular dysfunction. Am J Cardiol 1986;57:563–70. 5. Goldreyer BN, Gallagher JJ, Damato AN: The electrophysiologic demonstration of atrial ectopic tachycardia in man. Am Heart J 1973:85:205–15. 6. Scheinman MM, Basu D, Hollenberg M: Electrophysiologic studies in patients with persistent atrial tachycardia. Circulation 1974;50:266–73. 7. Klersy C, Chimienti M, Marangoni E, et al: Factors that predict spontaneous remission of ectopic atrial tachycardia. Eur Heart J 1993;14:1654–6. 8. Bauersfeld U, Gow RM, Hamilton RM, et al: Treatment of atrial ectopic tachycardia in infants < 6 months old. Am Heart J 1995;129:1145–8. 9. Bernuth GV, Engelhardt W, Kramer HH, et al: Atrial automatic tachycardia in infancy and childhood. Eur Heart J 1992;13:1410–5. 10. Donnerstein RL, Berg RA, Shehab Z, et al: Complex atrial tachycardia and respiratory syncytial virus infections in infants. J Pediatr 1994;125:23–8. 11. Ludomirsky A, Garson A Jr: Supraventricular tachycardia. In: Gillette PC, Garson A Jr, eds. Pediatric Arrhythmias: Electrophysiology and Pacing. Philadelphia: W.B. Saunders, 1990:380–426. 12. Wren C: Incessant tachycardias. Eur Heart J 1998;19:E32–6. 13. Naheed ZJ, Strasburger JF, Benson DW, et al: Natural history and management strategies of automatic atrial tachycardia in children. Am J Cardiol 1995;75:405–7. 14. Shinbane JS, Wood MA, Jensen DN, et al: Tachycardiainduced cardiomyopathy: a review of animal models and clinical studies. J Am Coll Cardiol 1997;29:709–15. J Formos Med Assoc 2000 • Vol 99 • No 10