Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
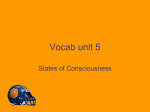
Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com 998 Thorax 1995;50:998-1004 Sleep-related breathing disorders * 4 Series editor: P M A Calverley Consequences of sleep disordered breathing Kathleen A Ferguson, John A Fleetham values.2 Blood pressure fluctuates considerably during REM sleep and is on average 5% higher than the preceding non-REM sleep.3 In patients with sleep disordered breathing there are brief phasic changes in blood pressure superimposed on a cyclical pattern which coincide with the upper airways obstruction (fig 2).4 The brief phasic changes in blood pressure are secondary to the large changes in intrathoracic pressure during obstructed respiration. Systemic blood pressure may increase by up to 20% during OSA and is maximal immediately after apnoea termination.56 The mechanism of the cyclical pattern in blood pressure during sleep disordered breathing is probably multifactorial in origin. Hypoxaemia, hypercapnic acidosis, increased respiratory effort, and the increased sympathetic activity associated with the awakening7 have all been proposed as mechanisms. Hypoxaemia does not appear to be a major causative factor as blood pressure remains unchanged in patients with OSA during Cardiac consequences SYSTEMIC HYPERTENSION supplemental oxygen therapy.8 Sympathetic Systemic blood pressure normally decreases nervous output and catecholamine production by 5-14% in non-rapid eye movement (non- are both increased during OSA.9 In patients REM) sleep compared with awake resting with OSA, catecholamine secretion decreases Sleep disordered breathing is common and may affect up to 24% of men and 9% of women.' There is a continuum in sleep disordered breathing associated with progressively more clinical consequences, from chronic snoring to obstructive sleep hypopnea to severe obstructive sleep apnoea (OSA). Although certain manifestations of sleep disordered breathing have been described for many years, a wider recognition of the clinical consequences has only occurred in the last decade. Sleep disordered breathing is characterised by recurrent upper airways obstruction which results in episodic asphyxia and interruption of the normal sleep pattern. The clinical consequences of sleep disordered breathing are quite diverse and are usually caused by either the recurrent asphyxia or sleep fragmentation (fig 1). Respiratory Division, Department of Medicine, Vancouver Hospital and Health Science Centre (UBC Pavilion), 2211 Wesbrook Mall, Vancouver, British Columbia, Canada V6T 2BS K A Ferguson J A Fleetham Reprint requests to: Dr J A Fleetham. Figure 1 Pathogenesis of the consequences of sleep disordered breathing. Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com 999 Consequences of sleep disordered breathing following effective treatment with either tracheostomy'0 or nasal CPAP therapy." Systemic hypertension occurs in 40-60% patients with OSA'2 and its severity is related to apnoea severity.'3 In contradistinction to normal subjects, blood pressure is higher in the moming than in the evening in patients with OSA.'4 Several studies have also shown that 22-30% of patients with systemic hypertension also have OSA.'"'7 These observations have led many to assume that the daytime systemic hypertension present in patients with sleep disordered breathing is due to the recurrent blood pressure increases during sleep. Most of the previous epidemiological studies did not, however, control for other confounding causes of hypertension. Obesity,""2' age, 1920 and alcohol consumption 'have subsequently been shown to be the major factors associated with systemic hypertension in patients with OSA, with apnoea severity a very much less important factor.'822 There is, however, some evidence for a causal association between OSA and systemic hypertension from studies in patients effectively treated with modalities other than weight loss. Nasal continuous positive airway pressure (CPAP) therapy acutely prevents the cyclical pattern of blood pressure changes during OSA.23 Long term treatment of OSA with tracheostomy24 and nasal CPAP25-27 reduces systemic blood pressure independently of any weight changes. The association between sleep disordered breathing and systemic hypertension appears to be mainly due to similar risk factors for both conditions. It is important to consider the diagnosis of sleep disordered breathing in patients with systemic hypertension, but further diagnostic studies are not indicated in the absence of other features of sleep disordered breathing. Systemic hypertension should be treated in patients with sleep disordered breathing, but there are no current data to recommend a specific antihypertensive approach in these patients. monary hypertension. Pulmonary artery pressure decreased in six patients with severe OSA following tracheostomy.3' A larger study found no significant decrease in pulmonary artery pressure following chronic nasal CPAP therapy.32 However, many of these patients had mild OSA and there was a decrease in pulmonary artery pressure in those patients with pulmonary hypertension. Right heart failure and hypercapnic respiratory failure both occur in severe OSA. These patients tend to be more obese, with daytime hypoxaemia and associated airways obstruction.3336 Chronic alcohol consumption has also been reported to be more common in these patients.37 The presence ofpulmonary hypertension and associated right heart failure in patients with sleep disordered breathing is invariably indicative of severe disease which requires prompt diagnosis and treatment. It is important to consider the diagnosis of sleep disordered breathing in patients with unexplained pulmonary hypertension. However, further diagnostic studies are not indicated in the absence of other features of sleep disordered breathing. CARDIAC FUNCTION Cardiac output decreases during OSA due to a decrease in heart rate without a concomitant increase in stroke volume5 caused by a decreased left ventricular preload.38 Left ventricular afterload increases during OSA and it has been hypothesised that this would result in left ventricular hypertrophy or dysfunction. There are several reports of echocardiography in patients with OSA. Hedner and associates39 excluded patients with systemic hypertension and found a larger left ventricular mass in patients with OSA compared with control subjects. However, in a better controlled study Hanly and colleagues40 failed to show any difference in left ventricular size or function between snorers and patients with OSA. Treatment of sleep disordered breathing can improve cardiac function in selected patients. PULMONARY HYPERTENSION/RIGHT HEART FAILURE Pulmonary artery pressures usually remain relatively unchanged during sleep in normal sub- EKG jects.28 In contrast, pulmonary artery pressure Thermistor i, increases by up to 100% during REM sleep.6 Rib cage ij I ".'jU1Vi4,. The cyclical changes in pulmonary artery pressure parallel the changes in systemic blood pressure (fig 2). These changes are due both Abdomen " ' to the effects of obstructed inspiratory efforts on pulmonary and cardiac dynamics, and to PRA 20 0I.i -tr )\; (mm Hg) -20 pulmonary hypoxic vasoconstriction. _40 Pulmonary hypertension occurs in a sub60 40 stantial proportion of patients with sleep dis- PPA ordered breathing. The prevalence of (mm Hg) 0,Y% pulmonary hypertension in patients with OSA has been reported to be between 10% and 100 90 20%,29 but may be as high as 55% in moderate Sao2 80 (%) 70 60 s to severe disease.30 Many studies of pulmonary 90 hypertension in sleep disordered breathing have Svo2 70 (%) 50 excluded patients with chronic obstructive lung disease, though frequently these two diseases Figure 2 Changes in pulmonary artery (PPA) and right coexist. Several studies have evaluated the atrial (PRA) pressures during obstructive sleep apnoea. effect of long term treatment of OSA on pul- Reproduced from ref 108 with permission. Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com 1000 Ferguson, Fleetham Long term nasal CPAP therapy has been shown to result in a small increase in left ventricular ejection fraction in patients with OSA and normal cardiac function.4' Nasal CPAP therapy results in a significant increase in cardiac function in patients with a cardiomyopathy and associated OSA.42 Extrapolating from these data, nasal CPAP has been proposed as an adjunct therapy for nonOSA patients with congestive heart failure and Cheyne-Stokes respiration.43 Other reports4445 have failed to confirm any improvement in cardiac function and have found that many of these patients are unable to tolerate nasal CPAP therapy. Until definitive studies in this field are completed, the long term efficacy of nasal CPAP treatment on cardiac function in patients without OSA needs to be evaluated on an individual basis. intracranial pressure increases in a cyclical pattern in patients with OSA. This cyclical increase in intracranial pressure coincides with the OSA and is maximal immediately after apnoea termination.57 The increase in intracranial pressure is secondary to both the cerebral vasodilatation caused by hypercapnea and the apnoea related increases in systemic blood pressure and central venous pressure. The increased intracranial pressure is probably the major contributing cause of the nocturnal and morning headaches present in some patients with sleep disordered breathing. The increased intracranial pressure also results in raised intraocular pressure which may result in glaucoma which can be a rare clinical presentation of sleep disordered breathing.58 It is important to consider sleep disordered breathing in patients with nocturnal headaches or glaucoma which is refractory to treatment. Patients with sleep disordered breathing have ISCHAEMIC HEART DISEASE an increased cerebrovascular mortality and Sleep disordered breathing has been shown to morbidity,59 and 53% of male patients with a be a significant risk factor in the development cerebrovascular accident (CVA) were chronic of ischaemic heart disease.4647 The combined snorers'o in one report. Of these, 35% had their effects of systemic hypertension, hypoxaemia, CVA during sleep and snoring was the only and increased sympathetic activity during sleep factor which correlated with the diurnal variare thought to promote the development of ation in the time of CVA. Furthermore, in a atherosclerosis. ST depression is relatively case controlled study of 400 patients admitted common in patients with OSA during overnight to hospital with a CVA, snoring has been shown ECG monitoring, and the duration of this is to be both an important risk factor for the reduced by nasal CPAP therapy.48 This ST development of a CVA and to adversely affect depression may reflect myocardial ischaemia prognosis." or non-specific changes associated with OSA. Myocardial ischaemia is reported to have occurred during polysomnography in five of 20 EXCESSIVE DAYTIME SLEEPINESS patients with combined ischaemic heart disease Sleep disordered breathing frequently presents and OSA.49 with excessive daytime sleepiness which can be evaluated both subjectively and objectively. The Epworth Sleepiness Scale is a quesCARDIAC ARRHYTHMIA tionnaire which asks about the likelihood of Cardiac rate normally decreases by 5-10% dur- falling asleep in eight different situations.62 ing non-REM sleep, with a slight increase dur- Patients with OSA tend to have a higher score ing REM sleep.23 In patients with sleep which is related to apnoea severity and imdisordered breathing the vagal stimulation proves following nasal CPAP therapy. Excessive caused by inspiring against the upper airway daytime sleepiness can also be objectively conobstruction results in sinus bradycardia during firmed by multiple sleep latency testing the apnoea followed by a reflex tachycardia at (MSLT).6' Mean sleep latency is reduced in apnoea termination.50 The degree of brady- patients with OSA, but may not improve in cardia is related to the severity of the associated patients who say they are using the treatment.64 arterial oxygen desaturation5' and is blunted The maintenance of wakefulness test (MWT) by administration of both atropine and sup- involves asking the patient to stay awake for 40 plemental oxygen.52 Cardiac arrhythmias dur- minutes on four occasions during the daytime. ing sleep are present in up to 50% of patients Patients with OSA have a decreased ability to with OSA.5' These arrhythmias are more fre- stay awake which is related to both apnoea quent when the OSA is associated with arterial severity and arterial oxygen desaturation.65 In oxygen desaturation54 and resolve following general, there is no need to perform an MSLT effective treatment of the OSA.5' The cyclical or MWT in patients with sleep disordered changes in heart rate seen in patients with sleep breathing unless their daytime sleepiness fails disordered breathing can be confused with sick to improve with effective treatment. sinus syndrome resulting in inappropriate treatSleep fragmentation, lack of slow wave sleep, and recurrent hypoxaemia have all been proment with cardiac pacing. posed as the cause of the excessive daytime sleepiness present in sleep disordered breathing. It is a common clinical observation that Neurological consequences some patients with loud snoring and no OSA CEREBROVASCULAR DISEASE Cerebral blood flow and intracranial pressure may have excessive daytime sleepiness, whereas both decrease during non-REM sleep and in- some patients with severe OSA deny any sleepicrease in REM sleep in normal subjects.55 How- ness.66 Bedard and associates demonstrated a ever, cerebral blood flow decreases56 whilst relationship between the severity of sleep hyp- Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com Consequences of sleep disordered breathing oxaemia and objective tests of both sleepiness and alertness in patients with moderate to severe OSA.67 Apnoea severity was related to objective tests of alertness, but not to sleepiness. Subsequently, Guilleminault and colleagues have shown that patients with OSA and excessive daytime sleepiness have both more sleep fragmentation and higher apnoea/ hypopnoea indices.68 Sleep disruption and recurrent hypoxaemia appear to interact to cause the excessive daytime sleepiness present in patients with sleep disordered breathing. Excessive daytime sleepiness is a well recognised cause of both automobile and industrial accidents.69 Patients with untreated OSA are poor drivers and have 2-3 times more automobile accidents than other drivers.7>72 This poor driving has been confirmed with driving simulators and improves with effective treatment with nasal CPAP.7' Automobile accidents involving patients with OSA may result in serious injury or death.74 It is important to consider the diagnosis of sleep disordered breathing when examining patients who fall asleep while driving or at work. Patients with sleep disordered breathing should be warned about the risks of driving, whilst seriously impaired drivers with sleep disordered breathing should be kept from driving until the sleep disordered breathing is effectively treated. Every physician involved in the management of patients with sleep disordered breathing should know and follow the local regulations for notifying licensing authorities about impaired drivers.75 1001 sleep disordered breathing in patients with Alzheimer's disease,87 whereas others have shown more sleep disordered breathing in patients with multi-infarct and Alzheimer's dementia.88 Currently there is no justification to screen elderly or demented patients for sleep disordered breathing, but it is important to consider this diagnosis in any patient with associated symptoms consistent with sleep disordered breathing. Endocrine consequences Decreased libido and/or impotence are frequently associated with sleep disordered breathing. Of 50 patients with severe OSA, 44% were reported to have either diminished sexual interest or performance."2 This sexual dysfunction is probably related in part to the daytime sleepiness or depression associated with sleep disordered breathing. There are, however, two reports8990 which suggest that sleep disordered breathing causes hypothalamic-pituitary dysfunction which is reversible following effective treatment. This reversible neuroendocrine dysfunction may contribute to the decreased libido and impotence in patients with sleep disordered breathing. Haematological consequences Secondary polycythaemia may occur in patients with sleep disordered breathing although this is uncommon in the absence of associated lung disease. Serum erythropoietin concentrations are not increased in patients with OSA or Psychological/psychiatric consequences related to the degree of nocturnal hypIntellectual deterioration, personality, and be- oxaemia.9 However, the normal diurnal rehavioural changes are well recognised features duction in serum erythropoietin concentrations of sleep disordered breathing. There are also during sleep does not occur in patients with significant psychological consequences of sleep OSA, and this may be sufficient to cause secdisordered breathing related to interpersonal ondary polycythaemia.92 Nasal CPAP therapy relationships at work and at home. Psycho- does reduce haematocrit acutely,9" but this is logical testing in patients with sleep disordered probably more related to changes in intrabreathing has demonstrated significant deficits vascular volume than erythropoietin conin thinking, perception, memory, and the ability centrations. The degree of hypoxaemia in to learn.76 Cognitive impairment is related to with sleep disordered breathing may the severity ofthe sleep hypoxaemia77 and sleep patients not be sufficient to stimulate erythropoietin fragmentation.78 Treatment of sleep disordered production and cause polycythaemia unless asbreathing may improve psychological status sociated with daytime hypoxaemia due to coand result in less anxiety and depression.79 disease. Sleep disturbances are a common feature existing lung of psychiatric disease, usually presenting as disorders of initiating and maintaining sleep. Sleep disordered breathing can also present Nephrological consequences with psychiatric disease such as depression80 Patients with sleep disordered breathing comand psychosis8' which then improve with monly complain of nocturia which then imeffective treatment.82 Sleep disordered breath- proves with effective treatment.24 Atrial ing may coexist with psychiatric illness, and natriuretic peptide concentrations are inrecognition ofthis will lead to appropnate treat- creased during sleep in patients with sleep disment. ordered breathing94 and decrease with nasal Sleep disordered breathing is more common CPAP therapy.95-97 The frequent nocturia in in the elderly, but the impact of this on daytime patients with sleep disordered breathing is function is unclear. Apnoea/hypopnoea severity probably related to diuresis and natriuresis in the elderly does not appear to be related caused by the recurrent hypoxaemia.9899 to daytime neuropsychological dysfunction.83-85 Patients with sleep disordered breathing are Similarly, the relationship between sleep dis- also more prone to have proteinuria which ordered breathing and dementia is con- improves with effective treatment.100101 The troversial.86 Some studies find no increase in mechanism of this proteinuria is unclear. Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com Ferguson, Fleetham 1002 KAF was a Glaxo/Canadian Medical Research Council Fellow. This study was supported by the British Columbia Health Research Foundation. 1-0! 1 Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. N Englj Med 1993;328:1230-5. 2 Khatri IM, Freis ED. Hemodynamic changes during sleep. J Appl Physiol 1967;22:867-73. 3 Snyder F, Hobson JA, Morrison DF, Goldfrank F. Changes in respiration, heart rate, and systolic blood pressure in human sleep. J Appl Physiol 1964;19:417-22. 4 Mateika JH, Matieka S, Slutsky AS, Hoffstein V. The effect of snoring on mean arterial blood pressure during nonREM sleep. Am Rev Respir Dis 1992;145:131-46. 5 Stoohs R, Guilleminault C. Cardiovascular changes associated with obstructive sleep apnea syndrome. J Appl r 0.9 0.1 2 0-8 E 0.6 0 1 2 3 6 5 4 Interval (years) 7 8 9 Figure 3 Probability of cumulative survival for patients with obstructive sleep apnoea who were either untreated (A, n=244) or treated with uvulopalatophatyngoplasty (, n= 149) or nasal CPAP (E) n = 126). Reproduced from ref 105 with permission. Physiwl 1992;72:583-9. 6 Coccagna G, Mantovani M, Brignani F, Parchi C, Lugaresi E. Continuous recording of the pulmonary and systemic arterial pressure during sleep in syndromes of hypersomnia with periodic breathing. Bull Eur Physiopathol Respir 1972;8:1159-72. 7 Hedner JA, Wilcox I, Laks L, Grunstein RR, Sullivan CE. A specific and potent pressor effect of hypoxia in patients with sleep apnea. Am Rev Respir Dis 1992;146:1240-5. 8 Ringler J, Basner RC, Shannon R, Schwartzstein R, Manning H, Weinberger SE, et al. Hypoxemia alone does not explain blood pressure elevations after obstructive apneas. J Appl Physiol 1990;69:2143-8. 9 Marrone 0, Riccobone L, Salvaggio A, Mirabella A, Bonanno A, Bonsignore MR. Catecholamines and blood pressure in obstructive sleep apnea syndrome. Chest 1993; 103:722-7. 10 Fletcher EC, Miller J, Schaaf JW, Fletcher JG. Urinary catecholamines before and after tracheostomy in patients with obstructive sleep apnea and hypertension. Sleep 1987;10:35-44. Mortality There are limited retrospective data on the mortality asociated with sleep disordered breathing, but most studies suggest a decreased long term survival. Partinen and colleagues'02 reported decreased five year survival in patients with untreated OSA compared with both patients treated by tracheostomy and the US age adjusted survival curve. He and coworkersl03 demonstrated a decreased survival in patients with untreated OSA with an apnoea index of >20/hour. This difference was most evident in patients below 50 years of age. The major cause of increased mortality in sleep disordered breathing appears to be cardiovascular in nature.104 There is no difference in the long term survival of patients with OSA treated with either corrective upper airway surgery or nasal CPAP (fig 3). 105 In elderly patients the effect of sleep disordered breathing on long term survival is less clear. Ancoli-Israel and colleagues106 showed an association between OSA and decreased survival in elderly women but not in men. Bliwise and coworkers107 demonstrated no difference in mortality in a group of treated and untreated elderly patients with OSA compared with control subjects. Conclusions Sleep disordered breathing causes episodic asphyxia and sleep fragmentation which result in many protean multisystem consequences. The immediate consequences of sleep disordered breathing have been extensively studied, but the long term significance of these consequences has not been well established. This would require long term prospective controlled studies in matched groups of treated and untreated patients with sleep disordered breathing. Such studies are no longer feasible because the currently available effective treatments could not ethically be withheld for prolonged periods of time. 11 Jennum P, Wildschi0dtz, Christensen NJ, Schwartz T. Blood pressure, catecholamines, and pancreatic polypeptide in obstructive sleep apnea with and without nasal continuous positive airway pressure (nCPAP) treatment. Am J Hypertens 1989;2:847-52. 12 Guilleminault C, Tilkian A, Dement WC. The sleep apnea syndromes. Ann Rev Med 1976;27:465-84. 13 Lavie P, Yoffe N, Berger I, Peled R. The relationship between the severity of sleep apnea syndrome and 24-h blood pressure values in patients with obstructive sleep apnea. Chest 1993;103:717-21. 14 Hoffstein V, MateikaJ. Evening-to-morning blood pressure variations in snoring patients with and without obstructive sleep apnea. Chest 1992;101:379-84. 15 Kales A, Bixler EO, Cadieux RJ, Schneck DW, Shaw LC III, Locke TW, et al. Sleep apnoea in a hypertensive population. Lancet 1984;ii:1005-8. 16 Lavie P, Ben-YosefR, RubinAE. Prevalence of sleep apnea syndrome among patients with essential hypertension. Am HeartJ 1984;108:373-6. 17 Fletcher EC, DeBehnke RD, Lovoi MS, Gorin AB. Undiagnosed sleep apnea in patients with essential hypertension. Ann Intern Med 1985;103:190-5. 18 Hoffstein V, Rubinstein I, Mateika S, Slutsky AS. Determinants of blood pressure in snorers. Lancet 1988;ii: 992-4. 19 Rauscher H, Popp W, Zwick H. Systemic hypertension in snorers with and without sleep apnea. Chest 1992;102: 367-71. 20 Milhman RP, Redline S, Carlisle CC. Assaf AR, Levinson PD. Daytime hypertension in obstructive sleep apnea prevalence and contributing risk factors. Chest 1991;99: 861-6. 21 StradlingJR, CrosbyJH. Relation between systemic hypertension and sleep hypoxaemia or snoring: analysis in 748 men drawn from general practice. BMJ' 1990;300:75-8. 22 Kiselak J, Clark M, Pera V, Rosenberg C, Redline S. The association between hypertension and sleep apnea in obese patients. Chest 1993;104:775-80. 23 Ali JN, Davies RJO, Fleetham JA, Stradling JR. The acute effects of continuous positive airway pressure and oxygen administration on blood pressure during obstructive sleep apnea. Chest 1992;101:1526-32. 24 Guilleminault C, Simmons FB, Motta J, Cummiskey J, Rosekind M, Schroeder JS, et al. Obstructive sleep apnea syndrome and tracheostomy - long-term follow-up experience. Arch Intern Med 1981;141:985-8. 25 Suzuki M, Otsuka K, Guilleminault C. Long-term nasal continuous positive airway pressure administration can normalize hypertension in obstructive sleep apnea patients. Sleep 1993;16:545-9. 26 Wilcox I, Grunstein RR, Hedner JA, Doyle J, Collins FL, Fletcher PJ, et al. Effect of nasal continuous positve airway pressure during sleep on 24-hour blood pressure in obstructive sleep apnea. Sleep 1993;16:539-44. 27 Mayer J, Becker H, Brandenburg U, Penzel T, Peter JH, Wichert Pv. Blood pressure and sleep apnea: Results of long-term nasal continuous positive airway pressure therapy. Cardiology 1991;79:84-92. 28 Lugaresi E, Coccagna G, Mantovani M, Lebrun R. Some during drowsiness and sleep periodic phenomena arising Clin Neurophysiol 1972;32:701in man. 5. 29 Weitzenblum E, Krieger J, Apprill M, Vallee E, Ehrhart M, Ratomaharo J, et aL Daytime pulmonary hypertension in patients with obstructive sleep apnea. Am Rev Respir Dis 1988;138:345-9. Elctoencephalogr Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com 1003 Consequences of sleep disordered breathing 30 Schroeder JS, Motta J, Guilleminault C. Hemodynamic studies in sleep apnea. In: Guilleminault C, Dement WC, eds. Sleep apnea syndromes. New York: Alan Liss, 1978: 177-99. 31 Motta J. Guilleminault C, Schroeder JS, Dement WC. Tracheostomy and hemodynamic changes in sleep-induced apnea. Ann Intern Med 1978;89:454-8. 32 Sforza E, KreigerJ, Weitzenblum E, Apprill M, Lampert E, Ratamaharo J, Long-term effects of treatment with nasal continuous positive airway pressure on daytime lung function and pulmonary hemodynamics in patients with obstructive sleep apnea. Am Rev RespirDis 1990; 141:866-70. 33 Krieger J, Sforza E, Apprill M, Lampert E, Weitzenblum E, Ratomaharo J. Pulmonary hypertension, hypoxemia, and hypercapnia in obstructive sleep apnea patients. Chest 1989;96:729-37. 34 BradleyTD, Rutherford R, Lue F, Moldofsky H, Grossman RF, Zamel N, et al. Role of diffuse airway obstruction in the hypercapnia of obstructive sleep apnea. Am Rev Respir Dis 1986-134:920-4. 35 Leech JA, Onal E, Baer P, Lopata M. Determinants of hypercapnia in occlusive sleep apnea syndrome. Chest 1987;92:807-13. 36 Bradley TD, Rutherford R, Grossman RF, Lue F, Zamel N, Moldofsky H. Role of daytime hypoxemia in the pathogenesis of right heart failure in the obstructive sleep apnea syndrome. Am Rev Respir Dis 1985;131:835-9. 37 Chan CS, Grunstein RR, Bye PTP, Woolcock AJ, Sullivan CE. Obstructive sleep apnea with severe chronic airflow limitation. Am Rev Respir Dis 1989;140:1274-8. 38 Tolle FA, Judy WV, Yu P-L, Marka ON. Reduced stroke volume related to pleural pressure in obstructive sleep apnea. J Appl Physiol 1983;55:1718-24. 39 HednerJ, Ejnell H, Caidahl K. Left ventricular hypertrophy independent of hypertension in patients with obstructive sleep apnoea. J Hypertens 1990;8:941-6. 40 Hanly P. Sasson Z, Zubeeri N, Alderson M. Ventricular function in snorers and patients with obstructive sleep apnea. Chest 1992:102:100-5. 41 KriegerJ, Grucker D, Sforza E, Chambron J, Kurtz D. Left ventricular ejection fraction in obstructive sleep apnea: effects of long-term treatment with nasal continuous positive airway pressure. Chest 1991;100:917-21. 42 Malone S. Liu PP, Holloway R, Rutherford R, Xie A, Bradley TD. Obstructive sleep apnoea in patients with dilated cardiomyopathy: effects of continuous positive airway pressure. Lancet 1991;338:1480-4. 43 Bradley TD, Holloway RM, McLaughlin PR, Ross BL, Walters J, Liu PP. Cardiac output response to continuous positive airway pressure in congestive heart failure. Am Rev Respir Dis 1992;145:377-82. 44 Buckle P, Millar T, Kryger M. The effect of short-term nasal CPAP on Cheyne-Stokes respiration in congestive heart failure. Chest 1992;102:31-5. 45 Davies RJO, Harrington KJ, Ormerod OJM, Stradling JR. Nasal continuous positive airway pressure in chronic heart failure with sleep-disordered breathing. Am Rev Respir Dis 1993;147:630-4. 46 Kosenvuo M, Kaprio J, Telakivi T, Partinen M, Heikkila K, Sarna S. Snoring as a risk factor for ischaemic heart disease and stroke in men. BMJ 1987;294:16-9. 47 Hung J, Whitford EG, Parsons RE, Hillman DR. Association of sleep apnoea with myocardial infarction in men. Lancet 1990;336:261-4. 48 Hanly P, Sasson Z, Zuberi N, Lunn K. ST-segment depression during sleep in obstructive sleep apnea. Am 7 Cardiol 1993;71:1341-5. 49 Koehler U, Duibler H, Glaremin T, Junkermann H, Lubbers C, Ploch T, et alNocturnal myocardial ischemia and cardiac arrhythmia in patients with sleep apnea with and without coronary heart disease. Klin Wochenschr 1991; 69:474-82. 50 Guilleminault C, Connolly S, Winkle R, Melvin K, Tilkian A. Cyclical variation of the heart rate in sleep apnea syndrome. Lancet 1984;i: 126-31. 51 Hanly PJ, George CF, Millar TW, Kryger MH. Heart rate response to breath-hold, Valsalva and Mueller maneuvers in obstructive sleep apnea. Chest 1989;95:735-9. 52 Zwillich C, Devlin T, White D, Douglas N, Weil J, Martin R. Bradycardia during sleep apnea. J Clin Invest 1982; 69:1286-92. 53 Guilleminault C, Connolly SJ, Winkle RA. Cardiac arrhythmia and conduction disturbances during sleep in 400 patients with sleep apnea syndromne. Am J Cardiol 1983; 52:490-4. 54 Shepard J W, Garrison MW, Grither DA, Dolan GF. Relationship of ventricular ectopy of oxyhemoglobin desaturation in patients with obstructive sleep apnea. Chest 1985;88:335-40. 55 Munari C, Calbucci F. Correlations between intracranial pressure and EEG during coma and sleep. Electroencephalogr Clin Neurophysiol 1981;51:170-6. 56 Fischer AQ, Chaudary BA, Taormina MA, Akhtar B. Intracranial hemodynamics in sleep apnea. Chest 1992; 102:1402-6. 57 Jennum P, Borgesen SE. Intracranial pressure and obstructive sleep apnea. Chest 1989;95:279-83. 58 Walsh JT, Montplaisir J. Familial glaucoma with sleep apnoea: a new syndrome? Thorax 1982;37:845-9. 59 Smime S, Palazzi S, Zucconi M, Chierchia S, FeriniStrambi L. Habitual snoring as a risk factor for acute vascular disease. Eur Respir J 1993;6: 1357-61. 60 Palomaki H, Partinen M, Juvela S, Kaste M. Snoring as a risk factor for sleep-related brain infarction. Stroke 1989; 20:1311-5. 61 Spriggs DA, French JM, Murdy JM, Curless RH, Bates D, James OFW. Snoring increases the risk of stroke and adversely affects prognosis. Q J Med 1992;303: 555-62. 62 Johns MW. Reliability and factor analysis of the Epworth sleepiness scale. Sleep 1992;15:376-81. 63 The clinical use of the multiple sleep latency test. Report from the American Sleep Disorders Association. Sleep 1992;15:268-76. 64 Sangal RB, Thomas L, Mitler MM. Disorders of excessive sleepiness - treatment improves ability to stay awake but does not reduce sleepiness. Chest 1992;102:699-703. 65 Poceta JS, Timms RM, Jeong DU, Swui-ling H, Erman MK, Mitler MM. Maintenance of wakefulness test in obstructive sleep apnea syndrome. Chest 1992;101: 893-7. 66 Guilleminault C, Stoohs R, Clerk A, Cetel M, Maistros P. A cause of excessive daytime sleepiness: The upper airway resistance syndrome. Chest 1993;104:781-7. 67 Bedard MA, Montplaisir J, Richer F, Malo J. Nocturnal hypoxemia as a determinant of vigilance impairment in sleep apnea syndrome. Chest 1991;100:367-70. 68 Guilleminault C, Partinen M, Quera-Salva MA, Hayes B, Dement WC, Nino-Murcia G. Determinants of daytime sleepiness in obstructive sleep apnea. Chest 1988;94:32-7. 69 Mitler MM, Carskadon MA, Czeisler CA, Dement WC, Dinges DF, Graeber RC. Catastrophes, sleep and public policy: consensus report. Sleep 1988;11:100-9. 70 Findley LF, Unverzagt ME, Suratt PM. Automobile accidents involving patients with obstructive sleep apnea. Am Rev Respir Dis 1988;138:337-40. 71 Aldrich MS. Automobile accidents in patients with sleep disorders. Sleep 1989;6:487-94. 72 Haraldsson PO, Carenfelt C, Diderichsen F. Nygren A, Tingvall C. Clinical symptoms of sleep apnea syndrome and automobile accidents. ORL 1990;52:57-62. 73 Findley U, Fabrizio MJ, Knight H, Norcross BB, Laforte AJ, Suratt PM. et al. Driving simulator performance in patients with sleep apnea. Am Rev Respir Dis 1989;140: 529-30. 74 Findley U, Weiss JW, Jabour ER. Drivers with untreated sleep apnea. A cause of death and serious injury. Arch Intern Med 1991;151:1451-2. 75 Stradling JR. Obstructive sleep apnoea and driving. BMJ 1989;298:904-5. 76 Kales A, Caldwell AB, Cadieux RJ, Vela-Bueno A, Ruch LG, Mayes SD. Severe obstructive sleep apnea - II: Associated psychopathology and psychosocial consequences. J Chron Dis 1985;38:427-34. 77 Findley U, Barth JT, Powers DC, Wihoit SC, Boyd DG, Suratt P. Cognitive impairment in patients with obstructive sleep apnea and associated hypoxemia. Chest 1986;90:686-90. 78 Cheshire K, Engleman H, Deary I, Shapiro C, Douglas NJ. Factors impairing daytime performance in patients with sleep apnea/hypopnea syndrome. Arch Intern Med 1992;152:538-41. 79 Klonoff H, Fleetham J, Taylor DR, Clark C. Treatment outcome of obstructive sleep apnea - physiological and neuro-psychological concomitants. JNerv Ment Dis 1987; 175:208-12. 80 Fleming JAE, Fleetham JA. A case report of obstructive sleep apnea in a patient with bipolar affective disorder. Can 7 Psychiatry 1985;30:437-9. 81 Berretini WH. Paranoid psychosis and sleep apnea syndrome. Am Y Psychiatry 1980;137:493-4. 82 Millman RP, Fogel BS, McNamara ME, Carlisle CC. Depression as a manifestation of obstructive sleep apnea: reversal with nasal continuous positive airway pressure. Y Clin Psychiatry 1989;50:348-5 1. 83 Berry DTR, Phillips BA, Cook YR, Schmitt FA, Gilmore RL, Patel R, et al. Sleep-disordered breathing in healthy aged persons: possible daytime sequelae. J Geront 1987; 42:620-6. 84 Knight H, Millman RP, Gur RC, Saykin AJ, Doherty JU, Pack Al. Clinical significance of sleep apnea in the elderly. Am Rev Respir Dis 1987;136:845-50. 85 Dickel MJ, Mosko SS. Morbidity cut-offs for sleep apnea and periodic leg movements in predicting subjective complaints in seniors. Sleep 1990;13:155-66. 86 Bliwise DL. Sleep in normal aging and dementia. Sleep 1993;16:40-81. 87 Bliwise DL, Yesavage JA, Tinklenberg JR, Dement WC. Sleep apnea in Alzheimer's disease. NeurobiolAging 1989; 10:343-6. 88 Erkinjuntti T, Partinen M, Sulkava R. Telakivi T, Salmi T, Tilvis R. Sleep apnea in multiinfarct dementia and Alzheimer's disease. Sleep 1987;10:419-25. 89 Santamaria JD, Prior JC, Fleetham JA. Reversible reproductive dysfunction in men and obstructive sleep apnoea. Clin Endocnnol 1988;28:461-70. 90 Grunstein RR, Handelsman DJ. Lawrence SJ, Blackwell C, Caterson ID, Sullivan CE. Neuroendocrine dysfunction in sleep apnea: reversal by continuous positive airways pressure therapy. J Clin Endocrinol Metab 1989; 68:352-8. 91 Goldman JM, Ireland RM, Berthon-Jones M, Grunstein RR, Sullivan CE, Biggs JC. Erythropoietin concentrations in obstructive sleep apnoea. Thorax 1991;46:25-7. 92 McKeon JL, Saunders NA, Murree-Allen K, Olson LG, Gyulay S, Dickeson J, et al. Urinary uric acid:creatinine ratio, serum erythropoietin, and blood 2,3-diphosphoglycerate in patients with obstructive sleep apnea. Am Rev Respir Dis 1990;142:8-13. 93 Krieger J, Sforza E, Delanoe C, Petiau C. Decrease in Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com Ferguson, Fleetham 1004 94 95 96 97 98 99 100 haemotocrit with continuous positive airway pressure treatment in obstructive sleep apnoea patients. Eur Respir 1992;5:228-33. Ichioka M, Hirata Y, Inase N, Tojo N, Yoshizawa M, Chida M, et al. Changes of circulating atrial natriuretic peptide and antidiuretic hormone in obstructive sleep apnea syndrome. Respiration 1992;59:164-8. Krieger J, Laks L, Wilcox I, Grunstein RR, Costas LJV, McDougall JG, et al. Atrial natriuretic peptide release during sleep in patients with obstructive sleep apnoea before and during treatment with nasal continuous positive airway pressure. Clin Sci 1989;77:407-11. Lin CC, Tsan KW, Lin CY. Plasma levels of atrial natriuretic factor in moderate to severe obstructive sleep apnea syndrome. Sleep 1993;16:37-9. Krieger J, Follenius M, Sforza E, Brandenberger G, Peter JD. Effects of treatment with nasal continuous positive airway pressure on atrial natriuretic peptide and arginine vasopressin release during sleep in patients with obstructive sleep apnoea. Clin Sci 1991;80:443-9. Warley ARH, Stradling JR. Abnormal diurnal variation in salt and water excretion in patients with obstructive sleep apnoea. Clin Sci 1988;74:183-5. Rodenstein DO, D'OdemontJP, Pieters T, Aubert-Tulkens G. Diurnal and nocturnal diuresis and natriuresis in obstructive sleep apnea. Am Rev Respir Dis 1992;145: 1367-71. Chaudhary BA, Sklar AH, Chaudhary TK, Kolbeck RC, Speir WA Jr. Sleep apnea, proteinuria, and nephrotic syndome. Sleep 1988;11:69-74. 101 Sklar AH, Chaudhary BA, Harp R. Nocturnal urinary protein excretion rates in patients with sleep apnea. Nephron 1989;51:35-8. 102 Partinen M, Jamieson A, Guilleminault CG. Long-term outcome for obstructive sleep apnea syndrome patients - mortality. Chest 1988;94:1200-4. 103 He J, Kryger MH, Zorick FJ, Conway W, Roth T. Mortality and apnea index in obstructive sleep apnea - experience in 385 male patients. Chest 1988;94:9-14. 104 Partinen M, Guilleminault C. Daytime sleepiness and vascular morbidity at seven-year follow-up in obstructive sleep apnea patients. Chest 1990;97:27-32. 105 Keenan SP, Burt H, Ryan CF, Fleetham JA. Long-term survival of patients with obstructive sleep apnea treated by uvulopalatopharyngoplasty or nasal CPAP. Chest 1994; 105:155-9. 106 Ancoli-Israel S, Klauber MR, Kripke DF, Parker L, Cobarrubias M. Sleep apnea in female patients in a nursing home: increase risk of mortality. Chest 1989;96: 1054-8. 107 Bliwise D, Bliwise N, Partinen M, Pursley A, Dement W. Sleep apnea and mortality in an aged cohort. Am Public Health 1988;78:544-7. 108 Shepard JW. Hemodynamics in obstructive sleep apnea. In: Fletcher E, ed. Abnormalities of respiration during sleep. Orlando, Florida: Grune and Stratton, 1986:46. Downloaded from http://thorax.bmj.com/ on May 2, 2017 - Published by group.bmj.com Sleep-related breathing disorders. 4. Consequences of sleep disordered breathing. K A Ferguson and J A Fleetham Thorax 1995 50: 998-1004 doi: 10.1136/thx.50.9.998 Updated information and services can be found at: http://thorax.bmj.com/content/50/9/998.citation These include: Email alerting service Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/