Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
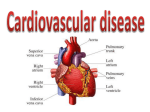
1082 Special Report Prevention of Rheumatic Fever A Statement for Health Professionals by the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Adnan S. Dajani, MD, Chairman; Alan L. Bisno, MD; Kyung J. Chung, MD; David T. Durack, MD, DPhil; Michael A. Gerber, MD; Edward L. Kaplan, MD; H. Dean Millard, DDS, MS; Martin F. Randolph, MD; Stanford T. Shulman, MD; Chatrchai Watanakunakorn, MD revention of both initial and recurrent attacks of acute rheumatic fever depends on control of Group A j-hemolytic streptococcal upper respiratory tract infections. These include tonsillopharyngitis (strep throat) and associated conditions such as otitis, sinusitis, and mastoiditis. Prevention of first attacks (primary prevention) is accomplished by proper identification and adequate antibiotic treatment of these streptococcal infections. The individual who has suffered an attack of rheumatic fever is inordinately susceptible to recurrences following subsequent Group A streptococcal upper respiratory tract infections and needs continuous protection to prevent recurrences (secondary prevention). The current recommendations reflect the fact that the incidence of rheumatic fever remains quite low in most areas of the country. These recommendations may not apply to certain areas of the United States where sharp increases in incidence of rheumatic fever have been noted recently, or regions of the world that continue to have a high incidence of the disease. Reappearance of acute rheumatic fever in a specific geographic region should draw attention to therapeutic, preventive, and epidemological measures as well as stimulate use of these recommendations. P Prevention of Initial Attacks (Primary Prevention) Group A streptococcal infections of the upper respiratory tract are the precipitating cause of rheumatic fever. During epidemics, as many as 3% of untreated acute streptococcal sore throats may be followed by rheumatic fever; in endemic infections, attacks of rheumatic fever may be fewer. AppropriThis report is an update of the 1984 statement, "Prevention of Rheumatic Fever," published in Circulation (70:1118A-1121A). Reprint requests should be addressed to the Office of Scientific Affairs, American Heart Association, 7320 Greenville Ave, Dallas, TX 75231. ate antibiotic treatment of streptococcal upper respiratory tract infection prevents acute rheumatic fever in most cases. Unfortunately, it is not uncommon for episodes of acute rheumatic fever to result from inapparent streptococcal infections for which patients do not seek medical care. These episodes, therefore, are not preventable. Diagnosis of Streptococcal Infections Prevention of initial episodes of acute rheumatic fever requires accurate recognition and proper antibiotic treatment of Group A streptococcal upper respiratory tract infections. Streptococcal skin infections (impetigo or pyoderma) do not lead to acute rheumatic fever and are not discussed here. Symptoms common in individuals with streptococcal pharyngitis or tonsillitis include sore throat (generally of sudden onset), headache, and fever of varying degree (usually from 101°~-104° F). Abdominal pain, nausea, and vomiting may occur, especially in children. Clinical signs suggesting streptococcal infection include anterior cervical lymphadenitis (tender lymph nodes), inflamed throat, tonsillopharyngeal exudate, excoriated nares (especially in infants), and a scarlatiniform rash. However, most of these manifestations are nonspecific and may be associated with respiratory tract infections from other causes. Signs and symptoms usually not associated with streptococcal infection are simple coryza, hoarseness, cough, conjunctivitis, anterior stomatitis, and diarrhea. Throat Culture Acute pharyngitis is more often caused by a virus rather than Group A streptococci. It is often difficult to differentiate on clinical grounds alone among infections caused by these etiologic agents. Group A streptococci are not a common cause of pharyngitis in children less than three years of age, and rheumatic fever is rare in this age group in the AHA Scientific Council Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 United States. First attacks of rheumatic fever are also rare in older adults. Throat cultures are valuable in establishing diagnosis of streptococcal infection and management of the patient with pharyngitis. Group A streptococci are virtually always found on a throat culture obtained during an active infection in an untreated patient. Unfortunately, the culture does not reliably distinguish between acute streptococcal infections and streptococcal carriers with concomitant viral infections. Nevertheless, the culture allows the physician to withhold antibiotic therapy safely in the majority of patients with sore throat, that is, those with negative cultures for Group A streptococci. Rapid antigen detection tests for diagnosis of Group A streptococcal pharyngitis are now available commercially and can provide results in minutes compared with the 24-48 hours required to obtain results of a throat culture. Most of these tests have a high degree of specificity; therefore, treatment is indicated for the patient with acute pharyngitis who has a positive test result. Physicians should be aware that most of these tests have less than the desired degree of sensitivity, particularly in instances where simultaneously obtained throat cultures show a sparse growth of Group A streptococci. Therefore, negative test results must be confirmed with a throat culture. Sparse growth of Group A streptococci does not necessarily reflect the carrier state and may indicate acute infection. Streptococcal Antibody Tests Streptococcal antibody tests are of no immediate value in diagnosis or management of acute streptococcal respiratory tract infections. However, antistreptolysin 0 (ASO), antideoxyribonuclease B (antiDNase B), and other streptococcal antibody tests are useful in confirming a recent Group A streptococcal infection. The tests are, therefore, helpful in patients who have possible nonsuppurative complications of streptococcal infections (acute rheumatic fever or acute glomerulonephritis). A commercially available agglutination test (such as the Streptozymes test), which is based on antibody agglutination of erythrocytes coated with a mixture of streptococcal antigens, is simpler to perform than traditional streptococcal antibody tests. However, the test suffers from significant variation in the potency of various lots, apparent lack of standardization, and poorly characterized antigenic composition, and is not recommended. Recommended Treatment Schedules Prevention of rheumatic fever requires eradication of Group A streptococci from the throat. Treatment should begin as soon as a definite diagnosis of Group A streptococcal infection is made (see Table 1). Penicillin, even when started several days after onset of acute illness, effectively prevents primary attacks of rheumatic fever; however, early diagnosis and therapy may reduce the period of infectivity Prevention of Rheumatic Fever 1083 TABLE 1. Primary Prevention of Rheumatic Fever (Treatment of Streptococcal Tonsillopharyngitis) Mode Duration Dose Agent intramuscular once Benzathine 600,000 units for patients <60 lb penicillin G 1,200,000 units for patients >60 lb or oral 10 days Penicillin V 250 mg 3 times daily (phenoxymethyl penicillin) For individuals allergic to penicillin: Erythromycin oral 10 days estolate 20-40 mg/kg/day 2-4 times daily (maximum 1 g/day) or oral 10 days ethylsuccinate 40 mg/kg/day 2-4 times daily (maximum 1 g/day) The following agents are acceptable but usually not recommended: amoxicillin, dicloxacillin, oral cephalosporins, and clindamycin. The following are not acceptable: sulfonamides, trimethoprim, tetracyclines, and chloramphenicol. as well as morbidity, allowing the patient to return to normal activity sooner. Virtually all patients are noncontagious 24 hours after initiation of therapy and may return to normal activities at that time, assuming that they complete the course of therapy. Penicillin is the drug of choice except in patients with allergic reactions.* Broad spectrum penicillins such as ampicillin and amoxicillin offer no advantages over penicillin in treatment of streptococcal pharyngitis. Penicillin may be administered intramuscularly or orally. Intramuscular administration of a single dose of benzathine penicillin G ensures adequate duration of treatment. If oral therapy is used, a full 10 days of treatment is necessary. Oral therapy requires patient compliance but may be associated with fewer allergic reactions. The choice between intramuscular and oral penicillin depends on the physician's assessment of the patient's likely compliance with an oral regimen and the risks of rheumatic fever in a particular population. Intramuscular Benzathine Penicillin G This formulation is preferred for patients who are unlikely to complete a 10-day course of oral therapy, patients with a personal or family history of rheumatic fever, and patients whose geographic or socioeconomic environment is at substantial risk for development of rheumatic fever. Injections that contain procaine penicillin in addition to benzathine penicillin G are less painful. If such mixtures are *Published reports conflict as to whether penicillin, especially ampicillin, interferes with effectiveness of oral contraceptives. The physician should advise the patient of childbearing age of possible drug interaction. The patient may choose to use a supplementary method of contraception while taking these antibiotics. 1084 Special Report Circulation Vol 78, No 4, October 1988 used, they should contain benzathine penicillin G in the following doses: The recommended dosage of benzathine penicillin G is 600,000 units intramuscularly for patients weighing 60 lb (27 kg) or less, and 1,200,000 units for patients weighing more than 60 lb. The combination of 900,000 units of benzathine penicillin G and 300,000 units of procaine penicillin G may be satisfactory in many smaller patients, but this dosage is based on limited data. The efficacy of this combination for heavier patients such as teenagers or adults requires further study. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Oral Penicillin The oral antibiotic of choice is penicillin V. Dosage for both children and adults is 250 mg, three times daily for 10 days. It is important to emphasize that patients should continue to take penicillin regularly for the entire 10-day period, even though they will likely be asymptomatic after the first few days. Other Antimicrobial Agents Antibiotics other than penicillin should be prescribed only for patients who are allergic to penicillin. Erythromycin is indicated for such patients and should be prescribed for 10 days. Erythromycin estolate (20-40 mg/kg/day) in two to four divided doses, or erythromycin ethyl succinate (40 mg/kg/day in two to four divided doses) is effective in treating streptococcal pharyngitis; however, efficacy of a twice-daily regimen in adults requires further study. The maximum dose of erythromycin is 1 g/day. Although strains of Group A streptococci resistant to erythromycin are prevalent in some areas of the world, they are rare in the United States. Oral cephalosporins, also given for 10 days, are acceptable alternatives for the patient allergic to penicillin. However, they should not be used in patients with immediate hypersensitivity to penicillin, and are more expensive. Certain antimicrobials are not recommended for treatment of streptococcal upper respiratory tract infections. Tetracyclines should not be used because of the high prevalence of strains resistant to this antibiotic. Sulfonamide drugs will not eradicate the streptococcus and should not be used to treat streptococcal infection, although they are effective as continuous prophylaxis for recurrent attacks of rheumatic fever (see below). Similarly, trimethoprimsulfamethoxazole should not be used to treat streptococcal pharyngitis. Prevention of Recurrent Attacks of Rheumatic Fever (Secondary Prevention) General Considerations A rheumatic patient who develops a streptococcal upper respiratory tract infection is at high risk of developing a recurrent attack of acute rheumatic fever. An infection need not be symptomatic to trigger a recurrence, which can strike even in optimally treated symptomatic infections. For these reasons, prevention of recurrent rheumatic fever depends on continuous antimicrobial medication rather than solely on recognition and treatment of acute episodes of streptococcal pharyngitis. In general, continuous antimicrobial prophylaxis is recommended for patients with a well-documented history of rheumatic fever (including cases manifested solely by Sydenham's chorea) and those with definite evidence of rheumatic heart disease. Such prophylaxis should be initiated as soon as acute rheumatic fever or rheumatic heart disease is diagnosed. A full therapeutic course of penicillin (as outlined under Recommended Treatment Schedules) should first be given to patients with acute rheumatic fever to eradicate Group A streptococci that may or may not be recovered on throat culture. Streptococcal infections occurring in family members of rheumatic patients should be treated appropriately. Duration of Prophylaxis Continuous antimicrobial prophylaxis provides the most effective protection from rheumatic fever recurrences. Risk of recurrence depends on several factors. For example, risk decreases as the interval since the most recent attack lengthens, while risk increases with multiple previous attacks. In addition, the patient's risk of acquiring a streptococcal upper respiratory tract infection must be considered. Adults with a high risk of exposure to streptococcal infections include parents of young children, teachers, physicians, nurses and allied health personnel, military recruits, and others living in crowded situations. Data also indicate a higher risk of recurrences in economically disadvantaged populations. Physicians must consider each patient's situation when determining appropriate duration of prophylaxis. Patients who have had rheumatic carditis are at a relatively high risk for recurrences of carditis and are likely to sustain serious cardiac involvement with each recurrence. Therefore, patients who have had rheumatic carditis should receive long-term antibiotic prophylaxis well into adulthood and perhaps for life. Prophylaxis should continue even after valve surgery, including prosthetic valve replacement, because these patients remain at risk of recurrence of rheumatic fever. In contrast, patients who have not had rheumatic carditis are at considerably less risk of cardiac involvement with a recurrence. Therefore, a physician may wish to discontinue prophylaxis in these patients after several years. In general, prophylaxis should continue until the patient is in his or her early 20s and five years have elapsed since the last rheumatic attack. The decision to continue prophylaxis should be made after discussion with the patient of potential risks and benefits and careful consideration of the epidemiological risk factors enumerated above. AHA Scientific Council TABLE 2. Secondary Prevention of Rheumatic Fever (Prevention of Recurrent Attacks) Agent Dose Mode Benzathine 1,200,000 units intramuscular every penicillin G four weeks* or Penicillin V 250 mg twice daily oral or Sulfadiazine 0.5 g once daily for oral patients <60 lb 1.0 g once daily for patients >60 lb For individuals allergic to penicillin and sulfadiazine: Erythromycin 250 mg twice daily oral *In high-risk situations, administration every three weeks is advised. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Choice of Program for Prevention of Recurrent Rheumatic Fever Intramuscular Benzathine Penicillin G An injection of 1,200,000 units of this long-acting penicillin preparation every four weeks is the recommended method of secondary prevention. In countries where incidence of acute rheumatic fever is particularly high, or in certain high-risk patients, use of benzathine penicillin G every three weeks may be warranted. Long-acting penicillin is of particular value in patients with a high risk of rheumatic fever recurrence, especially those with rheumatic heart disease in whom recurrence is more dangerous. In each patient, the advantages of benzathine penicillin G must be weighed against inconvenience to the patient and pain of injection, which may cause some patients to discontinue prophylaxis. Oral Agents Successful oral prophylaxis depends primarily on patient compliance. Patients need careful and repeated instructions about the importance of continuing prophylaxis. Most failures of prophylaxis occur in noncompliant patients. Even with optimal compliance, risk of recurrence is still higher in those on regular oral prophylaxis compared to those receiving intramuscular benzathine penicillin G. Oral agents are more appropriate for patients at lower risk for rheumatic recurrence. Accordingly, some physicians elect to switch patients to oral prophylaxis when they have reached late adolescence or young adulthood and have remained free of rheumatic attacks for at least five years. In the doses recommended below, sulfadiazine and oral penicillin are about equally effective. Sulfadiazine. The dosage is 1.0 g once daily for patients over 60 lb (27 kg) and 0.5 g once daily for patients under 60 pounds. Reactions are infrequent and usually minor. Blood counts may be advisable two weeks after starting prophylaxis, as leukopenia has been reported. Prophylaxis with sulfonamides is contraindicated in late pregnancy because of transplacental passage and competition with bilirubin for Prevention of Rheumatic Fever 1085 neonatal albumin-binding sites.* Data comparing sulfadiazine and other sulfonamides are not available. Penicillin V. The dosage is 250 mg twice daily. Penicillin V is the preferred form of oral penicillin because it is relatively resistant to gastric acid. Allergic reactions are similar to those with intramuscular penicillin. Anaphylaxis is rare in patients receiving oral penicillin. Note: Allergic reactions to penicillin are more common in adults than children. They occur in only a small percentage of patients, are more frequent after injection, and include urticaria and angioneurotic edema. A serum sickness-like reaction characterized by fever and joint pains may be mistaken for acute rheumatic fever. As with all penicillins, anaphylaxis, although rare, may occur. A careful history for allergic reactions to penicillin should be obtained. Other Drugs. For the exceptional patient who may be allergic to both penicillin and sulfonamides, erythromycin may be used. An appropriate dose has not been established, but 250 mg twice daily is suggested. Bacterial Endocarditis Prophylaxis Patients with evidence of rheumatic valvular heart disease also require additional short-term antibiotic prophylaxis before some surgical and dental procedures to prevent possible development of bacterial endocarditis. Antibiotic regimens used to prevent recurrences of acute rheumatic fever are inadequate for prevention of bacterial endocarditis. These patients should be protected by administration of appropriate antibiotics in recommended doses. Patients with prosthetic valves are at particularly high risk. The current recommendations of the American Heart Association concerning prevention ofbacterial endocarditis should be followed. Patients who have had rheumatic fever but do not have evidence of rheumatic heart disease do not need endocarditis prophylaxis. Special Problems There is uncertainty about the most appropriate management of treatment failures, chronic carriers, and contacts. Treatment Failures Failure to eradicate Group A streptococci from the throat usually occurs more frequently after oral antibiotic treatment than after administration of intramuscular benzathine penicillin G. Because risk of acute rheumatic fever is low in most US populations, and most patients who fail treatment are streptococcal carriers, post-treatment throat cultures are now indicated only in patients who are at unusually high risk for rheumatic fever, who remain symptom*Use of Sulfonamides for Rheumatic Fever Prophylaxis During Pregnancy. A statement by the Committee on Rheumatic Fever and Bacterial Endocarditis of the Council on Cardiovascular Disease in the Young: Ayoub EM, Shulman ST. Dallas, American Heart Association, 1981. 1086 Special Report Circulation Vol 78, No 4, October 1988 atic, or who develop recurring symptoms. Repeated courses of antibiotic therapy are not indicated in asymptomatic patients who continue to harbor Group A streptococci after appropriate therapy, except in rheumatic individuals, members of their families, or other epidemiological circumstances. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Carriers Chronic carriers usually do not need antibiotic treatment. However, a difficult diagnostic problem arises when carriers develop symptomatic upper respiratory tract viral infections. It is frequently not possible to determine whether Group A streptococci isolated from a carrier indicates current streptococcal infection or identifies that individual as a chronic carrier. Thus, it is often reasonable to administer a single course of therapy. Streptococcal carriers appear to pose little threat to themselves in developing sequelae of streptococcal infection, or in disseminating the organism to those who live and work around them. Therefore, streptococcal carriers usually do not need to be identified or treated. Asymptomatic Contacts In most circumstances, identification and treatment of asymptomatic household contacts are not indicated. However, in households with a rheumatic individual, or special epidemiological circumstances, it is advisable to obtain cultures and treat those with positive cultures. Selected References Books Shulman ST (ed): Pharyngitis: Management in an Era of Declining Rheumatic Fever. Philadelphia, Praeger Pubs, 1984 Breese BB, Hall C: Beta Hemolytic Streptococcal Diseases. Boston, Houghton Mifflin, 1980 Stollerman GH: Rheumatic Fever and Streptococcal Infection. New York, Grune & Stratton Inc, 1975 Markowitz M, Gordis L: Rheumatic Fever, ed 2. Philadelphia, WB Saunders Co, 1972 Book Chapters and Articles Krause RM: Streptococcal diseases, in Wyngaarden JB, Smith LH (eds): Cecil's Textbook of Medicine, ed 18. Philadelphia, WB Saunders Co, 1988, pp 1572-1580 Bisno AL: Rheumatic fever, in Wyngaarden JB, Smith LH (eds): Cecil's Textbook of Medicine, ed 18. Philadelphia, WB Saunders Co, 1988, pp 1580-1586 Markowitz M: Rheumatic fever, in Behrman RE, Vaughn VC III (eds): Nelson Textbook of Pediatrics, ed 13. Philadelphia, WB Saunders Co, 1987, pp 539-543 Wannamaker LW, Kaplan EL: Acute rheumatic fever, in Adams FH, Emmanouilides GC (eds): Moss' Heart Disease in Infants, Children, and Adolescents, ed 3. Baltimore, Williams and Wilkins Co, 1983, pp 534-552 Veasy GL, Wiedmeier SE, Orsmond GS, Ruttenburg HD, Boucek MM, Roth SJ, Tait VF, Thompson JA, Daly JA, Kaplan EL, Hill HR: Resurgence of acute rheumatic fever in the intermountain area of the United States. N EngI J Med 1987 ;3 16:421-427 American Heart Association Publications Prevention of bacterial endocarditis. A statement for health professionals by the Committee on Rheumatic Fever and Infective Endocarditis of the Council on Cardiovascular Disease in the Young: Shulman ST, Amren DP, Bisno AL, Dajani AS, Durack DT, Gerber MA, Kaplan EL, Millard HD, Sanders WE, Schwartz RH, Watanakunakorn C. Special report. Circulation 1984;70:1123A-1 127A Ad hoc committee to revise the Jones Criteria (modified) of the Council on Rheumatic Fever and Congenital Heart Disease of the American Heart Association: Jones criteria (revised) for guidance in the diagnosis of rheumatic fever. Circulation 1984;69:203A-208A Wannamaker LW: A method for culturing beta hemolytic streptococci from the throat. Circulation 1965;32:1054-1058 Prevention of rheumatic fever. A statement for health professionals by the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association. A S Danjani, A L Bisno, K J Chung, D T Durack, M A Gerber, E L Kaplan, H D Millard, M F Randolph, S T Shulman and C Watanakunakorn Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Circulation. 1988;78:1082-1086 doi: 10.1161/01.CIR.78.4.1082 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1988 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/78/4/1082.citation Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/