Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
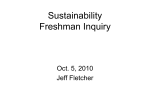
ORIGINAL ARTICLE ARCH SOC ESP OFTALMOL 2006; 81: 383-390 UTILITY OF OPTIC COHERENCE TOMOGRAPHY (OCT) IN THE FOLLOW-UP OF IDIOPATHIC INTRACRANIAL HYPERTENSION IN CHILDHOOD UTILIDAD DEL TOMÓGRAFO DE COHERENCIA ÓPTICA (OCT) EN EL SEGUIMIENTO DE LA HIPERTENSIÓN INTRACRANEAL IDIOPÁTICA EN LA INFANCIA SÁNCHEZ-TOCINO H1, BRINGAS R2, IGLESIAS D1, GONZÁLEZ-PÉREZ A3, DEL VILLAR-GALÁN R3 ABSTRACT RESUMEN Purpose: To show the utility of optic coherence tomography (OCT) in the follow up of the idiopathic intracranial hypertension (IIH) in childhood. Methods: Three girls, aged between 4 and 11 years, were diagnosed and subsequently followed with the help of OCT for an episode of idiopathic intracranial hypertension. All of them had presented with non-specific symptoms such as visual disturbance, headache, stomach ache, and in one case diplopia and torticolis. Brain imaging studies were normal, however lumbar puncture found an elevated intracranial pressure. Visual fields were tested using Octopus automated perimetry and the optic nerve fiber layer (ONF) was measured by OCT at each of the attendances. Results: The visual acuity was normal in all cases, but two girls had evidence of an abducens nerve palsy. Fundus biomicroscopy revealed marked papilledema. The thickness of the ONF was increased 2-3 times over normally expected levels. The Objetivo: Mostrar la utilidad de la tomografía de coherencia óptica (OCT) en el seguimiento de la hipertensión intracraneal idiopática (HII) en la edad pediátrica. Métodos: Se ha realizado el diagnóstico y posterior seguimiento, del episodio agudo de HII en tres niñas con edades entre 4 y 11 años. Todas acudieron con síntomas inespecíficos: Alteraciones visuales, cefalea, abdominalgia, visión doble y tortícolis. Los estudios de neuroimagen fueron normales. Tras la punción lumbar, la presión intracraneal estaba elevada. Se realizó campo visual (CV) mediante perímetro Octopus y medida de la capa de fibras nerviosas (CFN) con OCT en todas las revisiones. Resultados: La agudeza visual fue normal en todas ellas, con paresia de VI par en dos casos. El estudio de fondo de ojo reveló siempre un gran edema de papila. La medida inicial de la CFN con OCT se halló elevada, duplicando o triplicando los valores normales. El seguimiento y tratamiento con predni- Received: 16/12/05. Accepted: 17/7/06. Departamentos de Oftalmología y Pediatría del Hospital Río Hortega. Valladolid. Spain. 1 Ph.D. in Medicine. Ophthalmology specialist. 2 Graduate in Medicine. Ophthalmology specialist. 3 Graduate in Medicine. Pediatrics specialist. Paper presented at the LXXXI Congress of S.E.O. (Zaragoza 2005). Correspondence: Hortensia Sánchez Tocino Servicio de Oftalmología. Hospital Río Hortega Avda. Cardenal Torquemada, s/n 47010 Valladolid Spain E-mail: [email protected] SÁNCHEZ-TOCINO H, et al. follow up and the treatment with prednisone and azetazolamide was monitored by OCT, with a good outcome and return of the ONF levels to normal. In one case, however, a recurrence was detected after three months without treatment. Conclusion: IIH in childhood is an uncommon condition, often with a different presentation from what is seen in teenagers and adults. OCT is a useful technique helping in both the diagnosis and the follow-up of this disorder in children (Arch Soc Esp Oftalmol 2006; 81: 383-390). Key words: Optic coherence tomography in children, idiopathic intracranial hypertension, neuropathy in a child, papilledema, benign childhood intracranial hypertension, pseudotumor cerebri. INTRODUCTION Idiopathic intracranial hypertension or pseudotumor cerebri (HII) is defined as an abnormal elevation of intracranial pressure which is not associated to an expansive process or hydrocephalia and with normal cerebro-spinal liquid (1,2). It expresses as a papilledema frequently associated to small peripapillar hemorrhages, without afferent pupil defect and little involvement of visual acuity, at least initially. By means of three cases, this paper demonstrates the usefulness of Optical Coherence Tomography (OCT) as a diagnostic supplement and, above all, in the follow-up of this paediatric pathology. OCT allows observing an important increase in the thickness of the Nervous Fibre Layer (NFL), considerably greater than that found in previous neuritis conditions. SUBJECTS, MATERIAL AND METHODS This paper describes three cases of women aged 4-11 who attended the urgency ward due to nonspecific visual and systemic symptoms. In all cases, a full ophthalmological study was made with measurement of visual acuity (VA) with the Snellen test, study of eye movement, cover test, far dyplopia test with Worth lights, anterior biomicroscopy, 384 sona y acetazolamida vía oral se realizó de acuerdo a las medidas del OCT. La evolución fue buena con progresiva normalización de los valores de grosor en el OCT. Si bien en un caso, tras 3 meses sin tratamiento, se detectó mediante OCT una recurrencia asintomática. Conclusiones: La HII en edad pediátrica es una entidad poco frecuente y diferente de la afectación típica del adolescente y el adulto. El OCT es una técnica objetiva y reproducible que puede ayudar a completar el diagnóstico y, sobre todo, el posterior seguimiento clínico y terapéutico de estos cuadros en niños. Palabras clave: Tomografía de coherencia óptica en niños, hipertensión intracraneal idiopática, neuropatía en niños, papiledema, hipertensión intracranial benigna en la infancia, pseudotumor cerebri. eye fundus with 90 Dp lens, visual field (VF) with Octopus automatic perimeter (OCTOPUS, HaagStreit AG, Koeniz-Berne, Switzerland) and study of NFL with OCT. The thickness of the retina nervous fiber layer was measured with Optic Coherence Tomograph (OCT3, Carl Zeiss, Meditec, Dublin, CA, USA). OCT is a non-invasive image diagnostic method which carries out objective and direct quantitative measurements of the papilla and the NFL. It is based on an optical principle known as low coherence interferometry and utilizes an 820-nm wavelength light beam. A part of the light beam goes to the retina and the other to a reference mirror placed at a determined distance. The echoes obtained after reflecting off the retina are compared with those coming from the reference mirror, thus producing an interference which is captured and measured by a detector. In this way, two-dimension images are obtained which are compatible with histological images with an axial cross section of approximately 10 µm and a depth of 2 mm by means of scans which oscillate between 128 and 768 nm (3). Although the perfect condition for carrying out the scan is in midriasis, good images can be obtained without dilating the pupil. For studying the NFL structure, the OCT detects the anterior surface of the NFL and the pigmentary epithelium of the retina (RPE). As the said structures are highly reflective, they appear in red. In the NFL study, the parapapillar ARCH SOC ESP OFTALMOL 2006; 81: 383-390 Usefulness of OCT in idiopathic intracranial hypertension in childhood thickness parameters are automatically calculated and assessed in the vertical and horizontal axis along a circular scan. For making the measurements we utilized the Fast RNFL Thickness (3.4) mode under midriasis obtained with 1% cyclopentholate eye drops (Colircusi cyclopegic 1% Alcon Cusí, El Masnou, Barcelona, Spain). The measurements were analyzed with the RFNL Thickness Average Analysis protocol which is able to quantify the mean thickness in total microns (µ), in 4 peripapillar sectors: inferior, superior, nasal and temporal and in nine clock times; while the RNFL Thickness Serial Analysis Report was utilized for studying the differences in the thickness of the scans. In all cases, the pediatrics service of our hospital carried out a general analysis which included: hemogram, reactive protein C, rheumatoid factor, protein gram, ANA, antiDNA, thyroid hor-mones, cortisole, ASLO, serology against herpes virus, zoster, citomegalovirus, toxoplasmosis, legionella, coxiella, chlamydia, mycoplasma, borre-lia, syphilis, brucella, salmonella, rickerttsia and hidati-dosis; imaging studies: Computerized Axial Tomography (CAT), Magnetic Nuclear resonance (MNR) and angioresonance; electrical-physiological tests; electroencephalography and a lumbar punction, assessing the presence of proteins, glucose, cells and measuring intracranial pressure. In all three cases, the studies gave normal results excepting the intracranial pressure which was high. This pressure was taken in the subarachnoid space by means of a hydraulic system (liquid-filled column) in cm of water. FINDINGS Case 1 A ten-year old girl who attended our services due to abdominalgia. The ophthalmological exploration showed a VA of 1 in both eyes (BO), slight paresia of the VI cranial pair which caused dyplopia in extreme positions. The eye fundus evidenced a bilateral papillar edema (fig. 1). The CV showed an increase of the blind spot. OCT evidenced a diffuse thickening of the NFL Fig. 1: Case #1: A. Bilateral papilledema and OCT image with initial NFL thickening in RE. B. Papilla and OCT image one month later in RE. Normalization of NFL after treatment. ARCH SOC ESP OFTALMOL 2006; 81: 383-390 385 SÁNCHEZ-TOCINO H, et al. which maintains the typical double hunch pattern, mean NFL thickness 206 µm and 108 µm right eye (RE) and left eye (LE) respectively (fig. 1). The neuroimaging techniques, the analyses and the biochemical study of the cerebro-spinal liquid (CSL) gave normal results. Intracranial pressure was of 31 cm of H20. The Body Mass Index (BMI) was of 17,6 (percentage 50-75). Case 2 A four-year old girl who attended due to dyplopia, torticollis and Myodesopsia. Ophthalmological exploration revealed a VA of 1 in both eyes. Paresia in the VI pair of the left eye, torticollis with face on right side. Pathological Worth lights test. The eye fundus study revealed bilateral papilledema with small wedge-shaped hemorrhage in the inferior pole of the left eye. Considering the short age of the girl, the visual fields could not be taken as reliable. OCT showed a large increase of the NFL, with an average thickness of 200 µm and 245 µm in RE and LE respectively (fig. 2). CSL; analytical study and neuroimaging gave normal results. The intracranial pressure was 45 cm H20. IMC: 18.6 (percentage 90-95). Case 3 Eleven year-old patient previously diagnosed with pigmentous retinitis who attended the checkup practice referring blurred vision, dizziness and episodes of amaurosis fugax in the past few days. The exploration revealed a VA of 0.7 in both eyes, without changes from previous controls. No alterations in eye movements or dyplopia. The eye fundus revealed bilateral papilledema, retro-equatorial espicular pigment dispersion in the four quadrants and normal-looking maculae (fig. 3). They showed a peripheral restriction typical of pigmentous retinitis. OCT evidenced a large increase in NFL mean thickness from 546 µm in the RE and 442 µm in the LE (fig. 3). The analytical and neuroimage gave normal results. A lumbar punction revealed normal biochemistry and a pressure of 30 cm H20. BMI: 29,19, overweight (percentage 97). In all cases treatment was established with oral prednisone at a dosage of 1.5 mg/kg/day, Acethazolamide at 250 mg/8 hours, a potasium supplement and gastric protector supplied by the Pediatric Service at our Hospital. Both Papilledema and paresia of the VI pair improved in both cases during the first week. Other OCT tests were performed a week later, after 15 days, one month, and subsequently on a monthly basis. Figure 2 shows OCT evolution in case 2, consisting of a progressive decrease in NFL thickness. In case 3, the papilledema remained constant for eight weeks. Maximum follow-up time was 9 months (fig. 3). Corticoids were gradually withdrawn as soon as lab tests improved and there was significant reduction in NFL thickness on the OCT and Acethazolamide when NFL measurements were checked with OTC at around 110 µm. In the first two cases, this was achieved approximately in the third month; in case 3 treatment was prolonged for 6 months. In case 1, after 3 months untreated, a small transitional increase of NFL was detected by means of an OCT, although in the absence of symptoms, no treatment was prescribed. Nevertheless, in case 3, two months after treatment was completed there was a decrease in NFL thickness, down to 75 µm on the right eye and 67 µm on the left (fig. 4) which reflect an evolution towards a certain degree of atrophy. During the long-term 1-year follow-up, OCTs did not reveal in neither case 1 nor 2 any significant recurrence requiring new treatment. DISCUSSION Fig. 2: Case #2: Evolution of NFL: Initial, at 2 weeks, 3 months and 6 months. 386 HII is defined as an entity leading to an elevation of the intracranial pressure without apparent cause ARCH SOC ESP OFTALMOL 2006; 81: 383-390 Usefulness of OCT in idiopathic intracranial hypertension in childhood Fig. 3: Case number 3: A. Bilateral Papilledema. B. OCT image with initial NFL thickening in A.O. C. OCT with NFL during the 6th month in A.O. and with a normal image study of the central nervous system. The illness is well described in adults who characteristically show a female predominance and a link with obesity. In children, these characteristics may differ. The same gender distribution is present; the series published by Orssaud describe how 47 percent of the 30 patients surveyed were girls under 13, whereas 75% of those aged over 13 were women (4.5). Among adolescents, as in adults, this illness is linked to obesity and is primarily present among females. In prepuberal children, HII appears generally associated with cephalea, diplopia, strabismus and in certain cases also nape rigidity. Other general symptoms have been described as well, such as irri- tation, agressivity, behaviour alterations or drowsiness (6). Baker reported a loss of visual acuity (between 13 and 38 percent) in children with HII (7). Cinciripini found visual field defects in 85% of eyes, the most frequent being an increase of blind spots (6). No loss of VA was found in any of the cases presented herein. There was an initial CV defect in case 1 which subsided fully. In case 3, damage the visual field was linked to the pigmentary retinitis already present. No drusas were detected in the optical nerve either through tomography or OCT. Although most published series describe a full recovery of visual acuity, strabismus and CV ARCH SOC ESP OFTALMOL 2006; 81: 383-390 387 SÁNCHEZ-TOCINO H, et al. Fig. 4: Case number 3. Evolution of NFL over a 9 month period. defects, there are cases of permanent loss of VA(4) or visual field (6); diagnosis and early treatment are very important for fully tackling this diagnosis. In our series, only case number 3 showed a permanent loss of NFL which can be interpreted as a consequence of an acute HII without VA alteration. Nevertheless, based on the patient’s previous pathology and without prior OCT, we could not reject the possibility that the result obtained from measuring NFL existed from the very beginning. Other authors already described the impossibility of knowing via OCT whether the reduction in fiber thickness of the optical nerve is due to decrease of the edema or to fiber atrophy (8). Nonetheless, when linking OCT and other findings such as visual field, it proves to be very useful for the follow-up of patients with papilledema (8). The papilla normalizes usually at around 4 months if treatment was undertaken promptly enough. But in some cases evolution can lead to optical nerve atrophy (6). Nevertheless, there is no correlation between the papilla edema and the increase in pressure, or between the latter and the risk of an alteration in visual functions. On the other hand, CV alterations are not characteristic of this diagnosis (4). Although OCT does not help to clearly identify a papilledema, especially if it is a light, pseudopapilledema, a congenital elevation of the optical nerve, as proven by other authors (9), since it only detects 388 an increased thickness in the fiber layer around the optical nerve. Even in those cases where we detect in the optic fundus a papilledema together with a more or less evident migraine or without decrease in vision, OCT will not prevent the performance of neuroimaging tests; nonetheless, it will allow us to do the follow-up until achieving stabilization of the diagnosis (8). Kar-ma et al. (9) also point out the likelihood that the thickness of nerve fibers in patients suffering from a more severe case of papille-dema could be greater with significant statistical differences in eyes affected by pseudopapilledema. The present review shows that OCTs are very useful tests for HII, since they are objective, noninvasive and reproducible, they can be performed on children and allow supporting diagnoses in face of unspecified symptoms and, above all, they have proved to be very useful during follow-up and assessment of therapeutic efficacy on papilledema as illustrated by the normalization of NFL. Similarly, they have allowed for the detec-tion of recurrences and the discovery of chronic sequels after an acute episode of HII. REFERENCES 1. Biousse V, Bousser MG. L’hypertension intracrânienne bénigne. Rev Neurol (Paris) 2001; 157: 21-34. 2. Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain 1991; 114: 155180. 3. Chauhan DS, Marshall J. The interpretation of optical coherence tomography images of the retina. Invest Ophthalmol Vis Sci 1999; 40: 2332-2342. 4. Orssaud C, Dureau P, Zerah M, Cinalli G, Sainte Rose C, Kahn AP, et al. Benign childhood intracranial hypertension. J Fr Ophtalmol 2001; 24: 54-59. 5. Wall M. Idiopathic intracranial hypertension. Neurol Clin 1991; 9: 73-95. 6. Cinciripini GS, Donahue S, Borchert MS. Idiopathic intracranial hypertension in prepubertal pediatric patients: characteristics, treatment, and outcome. Am J Ophthalmol 1999; 127: 178-182. 7. Baker RS, Carter D, Hendrick EB, Buncic JR. Visual loss in pseudotumor cerebri of chidhood. A follow-up study. Arch Ophthalmol 1985; 103: 1681-1686. 8. Hedges TR. Optical coherence tomography in neuro-ophthalmology. In: Schuman JS, Puliafito CA, Fujimoto JG. Optical Coherence tomography of ocular diseases. 2nd ed. Thorofare: SLACK Incorporated; 2004; 13: 611-630. 9. Karam EZ, Hedges TR. Optical coherence tomography of the retinal nerve fibre layer in mild papilloedema and pseudopapilloedema. Br J Ophthalmol 2005; 89: 294-298. ARCH SOC ESP OFTALMOL 2006; 81: 383-390