Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Nuclear medicine wikipedia , lookup
Medical imaging wikipedia , lookup
Radiation burn wikipedia , lookup
History of radiation therapy wikipedia , lookup
Center for Radiological Research wikipedia , lookup
Radiosurgery wikipedia , lookup
Industrial radiography wikipedia , lookup
Backscatter X-ray wikipedia , lookup
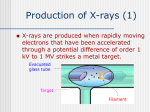
Students’ material Medical Imaging – The Glass Patient X-ray Photography Scientific/Technological fact sheet Introduction In 1895, Wilhelm Conrad Roentgen (1845-1923) discovered that when electrons were accelerated by a high voltage in a vacuum tube and allowed to strike a glass (or metal) surface inside the tube, fluorescent minerals some distance away would glow, and photographic film would become exposed. Roentgen attributed these effects to a new type of radiation (different from the already known cathode rays). They were given the name of X-rays after the algebraic symbol x, meaning an unknown quantity. He soon found that Xrays penetrated through some materials better than through others, and within a few weeks he presented the first X-ray photograph – of his wife’s hand (Figure 2). The production of X-rays today is usually done in a tube similar to Roentgen’s, using voltages of typically 80140 kV (Figure 1). Investigations into the nature of X-rays indicated that they were not charged particles (such as electrons) since they could not be deflected by electric or magnetic fields. It was suggested that they might be a form of invisible light. Today X-rays are indeed recognized as electromagnetic radiation with wavelengths in the range of about 0.01 nm to 10 nm, the range readily produced in an X-ray tube. However, contrary to the case of light, there seems to be no effective material to use as lenses for the very short wavelengths of X-rays. Figure 1 – X-ray tube. Electrons emitted by a heated cathode in a vacuum tube are accelerated by high voltage. When they strike the surface of the anode, the ‘target’, X-rays are emitted. Figure 2 – Roentgen’s first X-ray photograph. For a conventional medical (or dental) X-ray photograph, the X-rays emerging from the tube pass through the body and are detected on photographic film or a fluorescent screen (Figure 3). The rays travel in very nearly straight lines through the body with minimal deviation since at X-ray wavelengths there is little diffraction or refraction. There is absorption (and scattering), however. And the difference in absorption by different structures in the body is what gives rise to the image produced by the transmitted rays. The less the absorption is, the greater the transmission and the darker the film. The image is, in a sense, a ‘shadow’ of what the rays have passed through. In conventional X-ray images, the entire thickness of the body is projected onto the film; structures overlap and in many cases are difficult to distinguish. Within months of Roentgen’s 1895 discovery, X-rays had already become a powerful tool for medical diagnosis, and they have remained so to this day (Figure 4). Although many technical advances have been made over the years, the basic principles for normal X-rays have not changed significantly. Today, detection of X-rays on photographic film is being replaced by electronic detection and digital storage in computer memory. However, in the 1970s a revolutionary new technique called computed tomography (CT) using X-rays was developed (see Scientific/Technological fact sheet – Computed Tomography). Figure 3 – Conventional X-ray imaging, which is essentially shadowing. Figure 4 – X-rays are mainly known for their use at the dentist to check if there are any cavities (left). They are also often used to detect bone fractures and bone tumours (middle). With the help of a special contrast fluid the veins, intestines or other cavities can be made visible (right). In such a case non-toxic atoms with high atomic densities like Iodine (Z = 53) or Barium (Z = 56) are used. Reference – Adapted from Giancoli, Douglas C. (1998), Physics: principles with applications (5th edition, pp. 782, 784). Upper Saddle River, NJ: Prentice Hall. The X-ray tube X-rays for medical diagnostic purposes are produced by having highly accelerated electrons collide with the relatively heavy atoms of a rotating metal disk (the anode, typically made of tungsten, Z = 74) (Figure 1). These collisions cause the electrons to come to a sudden stop or to bend away, which makes them lose all or part of their kinetic energy and produce Bremm Strahlung or braking radiation with a continuous range of frequencies. If the colliding electrons have sufficient energy, they can even knock electrons out of the inner shells of the target metal atoms. Then electrons from higher states fall down to fill the vacancies, emitting X-ray photons with precise energies determined by the electron energy levels. These X-rays with a sharply defined frequency are called characteristic X-rays. The X-ray tube is of high power (20-100 kW), so must be cooled. Such tubes are expensive (10-35 k$), and last only 6-8 months. So they form a substantial financial burden for a radiology department at the hospital. Image formation From the anode the X-ray photons fly in all directions. A diaphragm forms the shape of the beam towards the patient, a process known as collimation. This prevents unnecessary exposure to radiation: the patient is only radiated where it is needed, and the personnel is protected. After passing the diaphragm, the X-ray photons enter the human body. Different tissues have various attenuation properties because they interact differently with the photons. Three different types of interaction can be distinguished (Figure 5): • Transmission – The photon does not Figure 5 – Interaction of X-ray photons with matter. interact: it passes the tissue without meeting any atom. The probabilities of interacting and not interacting depend on the electron densities of the different tissues. The lower the electron density of the tissue, the higher the probability of not interacting is. • Absorption – The photon interacts and transfers all its energy to the tissue’s atoms. In this case the photon ejects an electron from its atom, a process known as the photoelectric effect. As al of the photon’s energy is transferred, the photon completely disappears. • Scattering – The photon interacts and is diverted into a new direction, with or without loss of energy. Low energy photons just change their direction without loss of energy. Higher energy photons not only change their direction, but also lose part of their energy in the process of ejecting an electron from its atom. After the interaction the photon’s energy has become less, a process known as the Compton effect. Bone mainly consists of calcium with a large atomic mass (Z = 20) and thus has a high electron density. It therefore absorbs a lot of radiation. Soft tissues like liver, fat, muscles etc. are less dense and therefore a photon has a higher probability to pass these tissues. The attenuated radiation falls on a photon detecting film behind the patient, resulting in a 2D shadow image. A beam passing bone gives a low number of photons on the detector, with leaves the detector film white. The bigger number of transmitted photons that passed through soft tissues makes the film dark-coloured (just like the photons that go only through air). The attenuated intensity I of the X-ray beams at the detector depends on the intensity I0 at the source, the attenuation coefficient µ of the tissue and the path length d through the tissue: I = I0⋅e–µ⋅d This expression reflects an exponential fall in the intensity with distance, depending on the attenuation coefficient µ. The larger the µ-value (bone as compared to soft tissue), the faster the attenuated intensity I falls with distance. It is useful in radiology to define the mass attenuation coefficient µm, which refers to the attenuation per unit mass of material traversed: µm = µ/ρ, where ρ is the density of the material. The photons that reach the film in a straight line from the tube are called primary photons. Scattered or secondary photons can also reach the detector, but they cause the detector to have some background signal: haze. This can partly be avoided by using an anti-scatter grid (Figure 6), also known as a collimator. Figure 6 – The components of the X-ray imaging system and the formation of the radiographic image. B and E represent photons that have passed through the patient without interacting. C and D are scattered photons. The antiscatter grid has stopped D. Photon A has been absorbed. Figure 7 – Phosphor screen and film detector. X-rays are electromagnetic waves. The energy E of a photon is related to the frequency f and the wavelength λ of such a wave: E = h⋅f = h⋅c/λ. In this expression h is Planck’s constant (6.626⋅10–34 Js) and c is the velocity of electromagnetic waves (3.00⋅108 m/s). So, the energy of a photon is inversely proportional to the wavelength of the radiation. X-rays with short wavelength photons (with relatively high energy, called hard radiation) penetrate easier and are used when there are bones in the image. X-rays with long wavelength photons (with relatively low energy, called soft radiation) easily interact with the atoms of low atomic mass such as in soft tissues, and are therefore used for making breast images (mammography). Conventional screens – The conventional method for obtaining X-ray images is to use a cassette containing the film and an intensifying screen (Figure 7). All X-ray photons easily go through the film without interaction, but they are caught by the high-Z phosphor screen. This screen absorbs the X-rays and gives out fluorescent light exposing the film. The film is subsequently processed to form a final image. Digital screens – Nowadays digital screens replace these conventional screens almost everywhere. These digital screens typically consist of Europium-doted barium fluorohalide material. The amazing physical effect is that in this material the electrons in the Europium ions can be excited by the incoming photons to higher meta-stable energy levels, which have a very long lifetime of several weeks. The number of excited electrons depends on the dose at different locations of the imaging plate. So, a latent image is formed by these excited electrons. The cassette is then inserted into a read-out scanner where an infrared laser beam rapidly scans the imaging plate, pixel by pixel. This infrared radiation from the laser raises the energy of the electrons in the meta-stable level a little bit. This causes them to fall back to their original level under emission of a light photon, which is detected by a sensitive light detector (a photomultiplier tube). The image is converted into digital data before it is sent to the workstation for post-processing. The advantages of these digital screens include improvement in contrast ratio (1-105). Moreover, they can endlessly be reused. The digital images are easily sent to other departments in a hospital, and if needed all around the world. Storage of digital images is easier too. The digital modality with highest spatial resolution has 2500x2500 pixels/image, 12 bits/pixel. Clinical use The most well-known clinical use of X-ray imaging is, of course, diagnosing bone fractures. There are, however, quite a lot of other applications, including mammography, fluoroscopy and angiography. Mammography – Nowadays many countries have a national screening program to detect breast cancer in early stages: all women between the age of 50 and 65 are imaged once every two years. For imaging breast tissue, soft radiation is needed. These large wavelength photons are produced by a 25-37 kV X-ray tube with a Molybdenum anode. Because breast tissue absorbs 99 percent of this radiation, more radiation is needed to get a suitable transmitted dose for making an image with good contrast. Compression of the breast is necessary to reduce the tissue path length and thus the absorption. Fluoroscopy – Fluoroscopy is real-time interactive X-ray imaging. Instead of a short pulse of current through the Xray tube a small continuous current (1-3 mA) is applied. The detector is a special detection system for very low intensity X-ray radiation, a so-called image intensifier. In Figure 8 – Example of a mammogram with malignant fluoroscopy a live video image from the image intensifier tissue. on the TV monitor enables the radiologist to see a moving X-ray picture of the inside of the human body. It is mostly used during interventions. Radiological interventions are all activities on a radiology department that can be done in the body through a small hole with a catheter. Examples are blood vessel catheterisations (injecting contrast medium directly at the right place), ballooning or dottering (removing cholesterol etc. on the vessel wall by blowing up a small balloon on a catheter) or placing new vessel wall reinforcements (stents). Angiography – Digital Subtraction Angiography (DSA) is a powerful technique for the visualisation of blood vessels in the human body. In DSA a sequence of X-ray projection images is taken to show the passage of a bolus of injected contrast material through one or more blood vessels. The images below show, respectively, an image taken prior to injection (the mask image) and an image containing contrasted vessels (the live or contrast image) (Figure 9). The background structures are largely removed by subtracting the mask image from the live image, thus making the blood vessels clearly visible (Figure 10). The subtraction technique is based on the assumption that during exposure, tissues do not change in position or density. As can be observed from the DSA image shown, this is not always the case. In practice patient motion occurs, but infrequently. Figure 9 – DSA contraction images of a head. Left: mask image. Right: live image. Figure 10 – DSA image constructed out of Figure 9 with help of contrast enhancement. Radiation safety The softer the radiation, the higher the absorption of X-rays in the tissues is. And thus, the more energy remains behind in the patient and does not reach the film or the detector. This represents an unnecessary radiation dose, which should be avoided. Some safety measures have been taken to make X-rays less damaging to patients. First, the diaphragm at the tube prevents overexposure to radiation. The glass wall of the X-ray tube itself also acts as a soft-photon filter. In addition, an aluminium or copper safety filter absorbs a lot of the harmful soft radiation that leaves the tube. What is the nature of the damaging property of X-rays in tissues? The X-ray photons easily eject electrons from atoms, thus turning these atoms into ions. Those ions cause the production of free radicals such as OH– from water (H2O), which are very aggressive molecules. They cause molecular damage, like broken DNA-molecules, reduction of proteins, membrane damage etc. Cells can become totally disorganised and disorders in growing factors can cause diseases like cancer. So, too much or too soft radiation is rather damaging. Today, the typical radiation dose given is rather low, in the order of the natural background radiation. The dose of a chest X-ray is 0.1 mSv – the same dose as one gets from background radiation in a period of ten days. But one has always to be careful. Radiologists know: make the dose ALARA – As Low As Readily Achievable. This, of course, also holds for hospital personnel. Therefore, the people working the X-ray machines go behind a lead screen or wear a lead apron whenever the machine is in operation. Lead is a very good radiation absorber due to its high electron density. Physics principles involved • Electric field: accelerating charged particles, particle energy in eV • X-rays: transmission, absorption and scattering • Bohr model of the atom: electron energy levels, photon energy, radiation frequency and wavelength, fluorescence Additional links http://science.howstuffworks.com/x-ray.htm