Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
B4: 6
Psychostimulants HO2
GP Drug & Alcohol
Supplement No.12
February 2000
Amphetamine Dependence & Withdrawal
Dr. Rebecca McKetin,
Nationl Drug & Alcohol Research Centre
Dr. Sally McKenna,
CMO
Alcohol & Other Drugs Service
Background
Amphetamine belongs to a class of drugs known
as
central
nervous
system
(CNS)
sympathomimetics.
Sympathetic arousal
induced by amphetamine produces rapid and
sometimes irregular heart rate, sweating,
pupillary dilation, hypertension and increased
body temperature. The psychological changes
produced by amphetamine include euphoria or
pleasant effect, alertness, hypervigilance and
decreased appetite.
In the past, amphetamine was used medically to
treat narcolepsy, fatigue, depression, obesity and
attention deficit-hyperactivity disorder (ADHD).
Today, its medical use is restricted to ADHD and
narcolepsy because of the risk of dependence
and adverse effects on mental health. Despite
this, the use of illicit amphetamine continues.
Approximately 9% of the general population,
and one in five young adults (20-29 years),
report having ever used amphetamine (Australian
Institute of Health and Welfare, 1999)i. Aside
from their amphetamine use, most amphetamine
users have tried a variety of other licit and illicit
psychoactive substances, most commonly
cannabis, alcohol, hallucinogens and tobacco.
Patterns of use
Amphetamine is often used in conjunction with
parties and social events. Most first time users
and recreational users snort or swallow the drug.
Many regular amphetamine users make a
transition to injecting the drug within a couple of
years of their first use. Once users make the
transition to injecting, they are unlikely to return
to snorting or swallowing as their preferred
mode of administration.
Amphetamine users report shifting to injecting
because they believe it to be a cleaner, more
economical mode of administration. This belief
is a paradox. Nearly half of the amphetamine
users who start injecting report increased use of
amphetamine, and injection of other drugs that
they had not previously injected. Many injecting
users report daily use patterns, typically using
one to four "hits" of amphetamine per day (hit =
.25 to .50 "street" grams). On the whole,
injection of amphetamine is associated with
more frequent use, higher risk of dependence,
poorer social functioning and psychological
morbidity (Darke et al., 1994)ii.
Constituents of illicit amphetamine
Illicit amphetamine used in Australia almost
exclusively takes the form of white powder. Use
of liquid amphetamine ("ox-blood") or
prescription amphetamine is uncommon. There
are
occasional
reports
of
freebase
methamphetamine crystals (“ice” or “shabu”) in
Australia, usually imported from Asia. Most
illicit
amphetamine
in
Australia
is
methamphetamine, psychotropically the most
potent form of amphetamine,and less
commonly, dextro-amphetamine. Rarely does
“amphetamine” contain only ephedrine or other
amphetamine-related substances. The average
purity of illicit amphetamine in Australia is very
low (7%)(McKetin et al., 1999)iii.
Central Coast Health
GP Drug & Alcohol Supplement No. 12
Pharmacology
Amphetamine is a chemical compound that may
take the form of the methyl-, dextro- or the
inactive laevo- isomers. Amphetamine is easily
modified to produce a range of psychoactive
chemicals, some of which are also commonly
referred to as "amphetamines", although these
derivatives
do
not
necessarily
mimic
amphetamine's effect on the CNS. For example,
methylenedioxymethamphetamine (MDMA or
“ecstasy”) is an amphetamine derivative, but
belongs to a class of drugs called “entactogens”
due to its distinct psychological and
neuropharmacological effect (Nichols, 1994)iv.
After ingestion, amphetamine is rapidly
distributed throughout the CNS, where it
increases catecholamine activity (and serotonin
activity at higher doses), thus producing its
psychological effects. Amphetamine has a halflife of 4 to 15 hours and stays in the user's body
for approximately 12 to 72 hours after use,
where it can be detected in both blood and urine.
Urinary acidification dramatically reduces the
half-life of amphetamine. Although urinary
acidification can be used to speed the excretion
of amphetamine, it increases the risk of renal
failure.
Injection permits much greater
bioavailability than either snorting or swallowing
the drug (Cook et al., 1992)v.
Acute Intoxication
The visible effects of amphetamine intoxication
include dilated pupils, sweating, and agitation.
Other telltale signs of amphetamine use are low
body weight from anorexia, dehydration, nasal
ulcers or injection sites, lack of appetite, and a
disrupted sleep cycle. An acute toxic reaction to
amphetamine can occur from taking too much of
the drug, and may be characterised by
hypertension, tachycardia, arrhythmias, and
angina pectoris. Delirium is often reported by
amphetamine users during overdose, which may
result in part from hyperthermia and dehydration.
Extreme agitation or panic may also be present.
Most symptoms can be managed with
benzodiazepines, although cardiovascular
symptoms may require a sympathetic antagonist
(e.g., a cardio-selective -blocker) (Kamieniecki
et al., 1998)vi.
Psychosis
February 2000
Heavy amphetamine use can precipitate a
paranoid psychosis in some individuals.
Amphetamine psychosis varies widely in its
symptomatology, although paranoia is by far the
most common symptom followed by delusions
and hallucinations (auditory or visual).
Amphetamine psychosis usually remits rapidly
following an abstinence from the drug (0-10
days), and can be treated with antipsychotic
medication. Sometimes symptoms can be more
prolonged or can recur following use of
stimulant drugs (Sato, 1992)vii.
In addition to amphetamine psychosis,
amphetamine users may experience a range of
other psychiatric symptoms, particularly
depression and anxiety. Symptoms of depression
and anxiety are often present prior to the onset of
amphetamine use, but can be exacerbated by
amphetamine withdrawal. Symptoms of anxiety
and depression typically last 1 to 2 days after
cessation of amphetamine use (Hall et al.,
1996)viii.
Neurotoxicity
High doses of amphetamine (particularly
methamphetamine)
have
neurotoxic
consequences on monoaminergic neurons in a
variety of mammals, including rats, mice,
gerbils, vervet and rhesus monkeys. Most
animal research suggests a neurotoxic action on
dopaminergic nerve terminals, particularly in the
striatum (Ellison et al., 1978)ix.
Nerve
degeneration results in neurochemical depletion.
Neurochemical depletion usually shows partial
recovery over a period of several weeks to
months (Melega et al., 1996) x, but has also been
observed years after amphetamine exposure in
primates, suggesting enduring CNS changes
(Woolverton et al., 1989)xi.
Vascular Pathology
Amphetamine use has been associated with a
variety of cerebral vascular pathology, including
infarctions, vasculitis (inflammation and necrosis
of blood vessels), aneurisms, intracerebral
haemorrhages, haematomas, reduced cerebral
blood flow and fatal subarachnoid and subdural
haemorrhages. The most characteristic vascular
change associated with amphetamine use is a
phenomenon called "beading", a form of
vasculitus which refers to the alternate
narrowing and widening of blood vessels.
Intracerebral haemorrhage is thought to be due to
Central Coast Health
GP Drug & Alcohol Supplement No. 12
either rupture of aneurisms, possibly following
amphetamine-induced hypertension, or the
progressive worsening of vasculitus (beading)
with chronic amphetamine use.
These
complications have been found following both
oral and intravenous use and the mechanism
through which amphetamine produces such
vascular changes is unclear. Vascular pathology
may be a secondary consequence of
amphetamine use or drug impurities, or may be
related to pathology of immune processes
(Margolis et al., 1971; Matick et al., 1983)xiixiii.
Cognitive deficits
It has not been conclusively established whether
cerebral vascular pathology found among
amphetamine users or amphetamine’s neurotoxic
properties
affect
functioning in illicit
amphetamine users.
Nevertheless, several
studies have found evidence of impaired memory
and attention in illicit amphetamine users.
Specific deficits in brain function appear to be
strongly correlated with the current level of
amphetamine dependence (McKetin & Solowij,
1999)xiv.
Tolerance and Dependence
The development of tolerance and dependence to
the psychological and physiological effects of
amphetamine is less pronounced than for opiates,
but it is still well established. Five to 10 mg of
d-amphetamine is sufficient to yield a
psychological effect in a non-tolerant user,
whereas a tolerant user could engage in daily use
of several hundred milligrams (Ellinwood,
1971)xv. Cessation of amphetamine use in a
tolerant user is associated with both physical and
psychological withdrawal symptoms. Although
physical withdrawal symptoms exist, they are
less severe than those associated with opiate
withdrawal and occur only in severely dependent
users.
Psychological symptoms appear to
dominate
the
amphetamine
withdrawal
syndrome.
Amphetamine withdrawal symptoms include
psychological distress (mainly irritability,
depression and anxiety), circadian disturbances
(mainly reduced appetite and insomnia), somatic
symptoms (runny eyes/nose, diarrhea and
nausea), fatigue, and psychological disturbance
(mental confusion, difficulty concentrating, and
hallucinations) (Topp & Mattick, 1997)xvi. The
February 2000
temporal pattern of amphetamine withdrawal
symptoms can be seen in Table 1).
Table 1. Common Symptoms in Amphetamine
Withdrawal (Pead et al., 1996)xvii
Time from
Signs and Symptoms:
Last Use:
Days 1 to 3
exhaustion
“the crash”
increased sleep
depression
Days 4 to 7
strong urges to use
amphetamines
mood swings, alternating
between irritability,
restlessness & anxiety to
feeling tired, lacking energy
& generally run down
poor sleep & concentration
headaches, generalised aches
& pains
increased appetite
increased feelings of paranoia
such as people are ‘out to get
you’, misunderstanding things
around you, such as seeing
things that are not there
Days 7 to 28
most symptoms start to settle
down, although common
symptoms can include:
mood swings, alternating
between feeling anxious,
irritable or agitated, to feeling
flat and run down
poor sleep
cravings
1 to 3 months
return of normal sleep and
activity
major improvements in health
and mood
Treatment
The majority of amphetamine users have not had
contact with treatment services, possibly
reflecting the lack of amphetamine-specific
treatment options available in Australia.
However, it may also be because many users
claim that they can manage amphetamine-related
problems on their own. Three quarters of
amphetamine users surveyed by Hando et al.
(1997) had tried to reduce their amphetamine use
without professional assistance. Of these, 93%
successfully reduced their amphetamine use and
83% were satisfied with the outcome. Below are
Central Coast Health
GP Drug & Alcohol Supplement No. 12
some strategies to assist amphetamine users who
would like to reduce their use (Hando et al.,
1997)xviii.
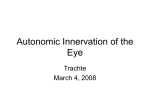
Strategies for reducing/ceasing use
A key issue in assessing what strategy is used for
patients who are amphetamine dependent is their
readiness to quit. A useful model in assessing a
patient’s motivation is the ‘Stages of Change
Model’ (figure 1 adapted from Prochaska and Di
Clementexv1v).
Figure 1
Non user
Relapse
Unsure
30%
Maintenence
Ready
10%
Ask “where does this leave you now?”
Get the patient to make a list of the things they
like about their amphetamine use and the things
that they dislike. This list can provide impetus
for reducing use, and can be referred to at later
stages of the withdrawal process to assist with
maintaining abstinence.
Mood Diary
Lapses
This model provides a simple method of
questioning to determine the ‘stage of change’ of
the patient. The model involves four stages and
indicates whether the patient:
Summarise your understanding of the patient’s
pros and cons.
Get the patient to construct a mood diary, in
which they note the time/place/mood/company
where they feel like using amphetamine. Use
this diary to identify triggers for amphetamine
use, and work with the patient to identify
alternative activities that they can substitute for
amphetamine use.
Ex user
Not ready
60%
February 2000
is not ready ( pre-contemplation stage)
is unsure (contemplation stage)
is ready ( action stage )
has quit, but is at risk of relapse (maintenance
stage ).
This process is active, in that the patient can be
assisted through each of the stages in order to
achieve the patient’s desired goal.
Comparing the pros and cons of amphetamine
use
Motivational interviewing is a useful style of
counselling for these ambivalent patients. The
aim is to elicit the patient’s own thoughts about
the pros and cons or the “good” and “not so
good” things about amphetamine use. The doctor
then summarises these and encourages the
patient to think about them. This helps the
patient to take responsibility for the decision to
change their behaviour.
Ask “what do you like about your drug use?”
Ask “what are the things you don’t like so
much about your drug use?”
It is important not to treat lapses as failures.
Identify situational triggers that preceded the
lapse, and develop strategies for avoiding lapses
in similar situations in the future.
Getting through withdrawal Non-pharmacological treatment
The most severe part of the withdrawal phase is
the first few days to a week. During this time the
patient should plan a safe supportive
environment, and a support person. Make sure
the patient will have little contact with other
amphetamine users or dealers, and remove drug
paraphernalia from their surrounds. The support
person(s), should not be using drugs or in a
position to tempt the patient to use drugs, or
supply drugs to the patient. Get the patient to
make a list of potential support people to assist
them throughout the withdrawal process, and a
list of people who they should avoid contact with
during this time.
Somatic symptoms are common during
withdrawal and can be managed with warm
baths, massages or light exercise. Relaxation
techniques (muscle relaxation and breathing
exercises) can be used to reduce anxiety and
insomnia.
Coping with cravings
Provide strategies for coping with the cravings.
One strategy – delay, distract, decide – is
described below.
Central Coast Health
GP Drug & Alcohol Supplement No. 12
Delay
Get the patient to delay the decision to use for a
designated period of time (e.g., one hour).
Distract
During this time, get the patient to engage in an
activity that interests them, to distract them from
their craving.
Decide
Once the craving has subsided get the patient to
review their list of pros and cons of
amphetamine use, reinforce their own reasons
for wanting to reduce use. Then get them to
make a decision about whether they will
continue to use the drug.
Explain to the patient that cravings will occur,
but will also subside and can be coped with.
Pharmacological treatment
Most patients do not require medication,
however when necessary pharmacologic
interventions can be used to reduce the severity
of withdrawal symptoms.
Somatic symptoms
Mild analgesics (e.g. paracetamol) may be used
as necessary.
Anxiety and insomnia
Benzodiazepines may be used to address these
symptoms, yet they should only be used during
the acute withdrawal phase and for no longer
than one weeks duration.
Craving and dysphoria
Chronic psychostimulant use is believed to act
on a large number of neurotransmitter systems
including dopaminergic, noradrenerigc and
serotonergic, resulting in neurotransmitter
depletion and receptor super-sensitivity. During
withdrawal this depletion can impact by
increasing cravings and lowering mood.
Medications that may be considered to target
such symptoms and include;
February 2000
A tricyclic antidepressant, may reduce cravings
by reducing receptor super-sensitivity in both
dopaminergic and noradrenergic systems. Initial
dose 25-30mg nocte then increase by 50-150mg
per week, as tolerated, until reaching a maximum
of 150-300mg nocte.
b) Bromocriptine
A dopamine receptor agonist, may also reduce
cravings, but non-compliance due to drug side
effects limits its use. Commence dosing at 0.625
mg tds then gradually increase to 7.5-12.5 mg
tds, as tolerated over 14 days.
c) Amantadine
An indirect dopamine agonist, may be as
effective as bromocriptine in reducing cravings.
Further
information
on
treatment
of
amphetamine
dependence
and
self-help
resources for amphetamine users:
A Users’ Guide to Speed – available from the
National Drug and Alcohol Research Centre, Ph.
(02) 9385 0333, Fax (02) 9385 0222
Getting Through Withdrawal – available from
Turning Point Alcohol and Drug Centre Inc. Ph.
(03) 8413 8413, Fax. (03) 9416 3420
Models of intervention and care for
psychostimulant users, by G. Kamieniecki, N.
Vincent, S. Allsop & N. Lintzeris. National
Centre for Education and Training on Addiction,
Monograph Series No. 32. Commonwealth of
Department of Health and Family Services,
1998.
General Practitioners who require further
information or assistance regarding patients
who are using or wish to withdraw from
amphetamines can contact the GP Drug &
Alcohol Local Consultancy Service on
0413 276 177.
This service is for General Practitioners only.
Patients can contact the Central Coast Health
Alcohol and Other Drugs Service on 4393 4880.
a) Desipramine
References
i
Australian Institute of Health and Welfare (1999). The 1998 National Drug Strategy Household Survey.
Central Coast Health
GP Drug & Alcohol Supplement No. 12
ii
February 2000
Darke, S., Cohen, J., Ross, J., & Hando, J. (1994). Transitions between routes of administration of regular amphetamine users.
Addiction, 89, 1077-1083.
iii McKetin, R., Darke, S., Hayes, A. & Rumbold, G. (1999). Drug Trends 1998: A comparison of drug use and drug trends in
three Australian states. Findings from the Illicit Drug Reporting System (IDRS). NDARC Monograph No. 42. Sydney, UNSW.
iv Nichols, D. E. (1994). Medicinal chemistry and structure-activity relationships. In A. K. Cho & D. S. Segal (Eds.), Amphetamine
and its analogs (pp. 3-41). San Diego, CA: Academic Press.
v Cook, C. E., Jeffcoat, A. R., Sadler, B. M., Hill, J. M., Voyksner, R. D., Pugh, D. E., White, W. R., & Perez-Reyes, M. (1992).
Pharmacokinetics of oral methamphetamine and effects of repeated daily dosing in humans. Drug Metabolism and Disposition, 20,
856-862.
vi Kamieniecki, G., Vincent, N., Allsop, S. & Lintzeris, N. (1998). Models of intervention and care for psychostimulant users.
National Centre for Education and Training on Addiction, Monograph Series No. 32. Canberra, Commonwealth of Department of
Health and Family Services.
vii Sato, M. (1992). A lasting vulnerability to psychosis in patients with previous methamphetamine psychosis. Annals of the New
York Academy of Sciences, 654, 160-170.
viii Hall, W. Hando, J., Darke, S. & Ross, J. (1996). Psychological morbidity and route of administration among amphetamine users
in Sydney, Australia. Addiction, 91, 81-87.
ix Ellison, G., Eison, M. S., Huberman, H. S., & Daniel, F. (1978). Long-term changes in dopaminergic innervation of caudate
nucleus after continuous amphetamine administration. Science, 201, 276-278.
x Melega, W. P., Quintana, J., Raleigh, M. J., Stout, D. B., Yu, D.-C., Lin, K.-P., Huang, S.-C., & Phelps, M. E. (1996). 6[18F}Fluoro-L- DOPA-PET studies show partial reversibility of long-term effects of chronic amphetamine in monkeys. Synapse,
22, 63-69.
xi Woolverton, W. L., Ricaurte, G. A., Forno, L. S., & Seiden, L. S. (1989). Long-term effects of chronic methamphetamine
administration in rhesus monkeys. Brain Research, 486, 73-78.
xii Margolis, M. T., & Newton, T. H. (1971). Methamphetamine ("speed") arteritis. Neuroradiology, 2, 179-182.
xiii Matick, H., Anderson, D., & Brumlik, J. (1983). Cerebral vasculitis associated with oral amphetamine overdose. Archives of
Neurology, 40, 253-254.
xiv McKetin, R., & Solowij, N. (1999). Event-related potential indices of selective attention in dependent amphetamine users.
Biological Psychiatry, 45, 1488-1497.
xv Ellinwood, E. H. (1971). Assault and homicide associated with amphetamine abuse. American Journal of Psychiatry, 127,
1170-1175.
xvi Topp, L., & Mattick, R. P. (1997a). Validation of the amphetamine dependence syndrome and the SamDQ. Addiction, 92, 157167.
xvii Pead J., Lintzeris, N., & Churchill, A. (1996). From Go to Whoa. Amphetamines and analogues. Canberra: Australian
Government Publishing Service.
xv1v Prochaska, J.O. & DiClemente, C.C. 1986. Toward a comprehensive model of change. In W.R. Miller & N. Heather (Eds),
Treating addictive behaviors: processes of change. Plenum Press: New York.
xviii Hando, J., Topp, L., & Hall, W. (1997). Amphetamine-related harms and treatment preferences of regular amphetamine users
in Sydney, Australia. Drug and Alcohol Dependence, 46, 105-113.
.
Central Coast Health