Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
A
Synthetic Anticoagulant: A Polysulfuric
Acid Ester of Polyanhydromannuronic
Acid (Paritol)
Experience with Its Use in Man
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
By C. W. SORENSON, M.D. AND IRVING S. WRIGHT, M.D.
The effects of the use of Paritol administered intravenously to 35 individuals are herein reported.
This synthetic anticoagulant produces a prolongation of the clotting time similar to that produced
by heparin but of longer duration, if appropriate dosage is used. As with heparin, at therapeutic
clotting time levels, the prothrombin time is slightly prolonged. Certain untoward effects have
been noted and are described. Further studies with Paritol appear justified in order to evaluate
its usefulnes3 as a rapidly acting anticoagulant.
is concerned with further studies made on the
action of Paritol in man.
T HE AVAILABILITY of a rapidly acting
anticoagulant is extremely important in
the treatment of medical and surgical
thromboembolic conditions. The most serious
handicaps in the use of heparin in this role
has been the difficulty of its preparation and
the resulting high cost which seriously limit
its clinical use. Chemical studiesl-3 on the structure of heparin indicate that it is a polysaccharide esterified with sulfuric acid. Therefore,
considerable work4-7 has been done on the synthesis of various polysaccharide sulfuric acid
esters having anticoagulant activity. Most of
these synthetic compounds have been found to
be toxic when administered to animals and
thus have no clinical value. Seifter and Begany'
reported studies on the pharmacology and
toxicology of a polysulfuric acid ester of
polyanhydromannuronic acid (Paritol) which
suggested its possible clinical use. The anticoagulant activity of this material and its low
-toxicity in animals warranted further investigation. A preliminary report relating to its use
in man appeared in 1949.9 The present report
METHOD
Observations have been made on the administration of Paritol* to 35 individuals. Their
ages ranged from 20 to 70 years. Thirty-one
were males; 4 were females. Four were normal
controls; 31 had a variety of disease conditions,
including pulmonary infarction, thrombophlebitis, thromboangiitis obliterans, axillary vein
thrombosis, carcinoma of the lung, arteriosclerosis obliterans, myocardial infarction, diabetes
mellitus, embolus to a peripheral artery from a
fibrillating rheumatic heart, and postoperative
arterial-venous anastomosis. In 15 patients the
drug was used therapeutically because of some
thromboembolic disease; in the other 16 it was
given to observe its effect. With 2 exceptions,
patients were selected who showed no evidence
of liver or kidney disease, or allergic or hemorrhagic tendencies. One exception was a patient
who had chronic nephritis complicating rheumatic heart disease with a pulmonary infarction. The other had arteriosclerotic heart disease, auricular fibrillation, congestive heart
failure, early cirrhosis of the liver, and multiple
pulmonary emboli.
The effects of the intravenous administration
of Paritol were observed for the following: the
From the Department of Medicine, The New York
Hospital-Cornell University Medical College.
This work was conducted under the auspices of
the Committee on Anticoagulants of the American
Heart Association aided by grants from the Samuel
H. Kress Foundation, the Albert and Mary Lasker
Foundation, the Lillia Babbitt Hyde Foundation and
the Julius W. Hampil Foundation.
* Supplied through the courtesy of Wyeth, Inc.
658
Circulation, Volume II, November, 1950.
659
C. W.SORENSON AND I. S. WRIGHT
response of the blood pressure, pulse, and respirations; delayed reactions as manifested by
temperature rise or allergic manifestations; alterations in the clotting time, the red blood
cell count, the white blood cell count, and the
sedimentation rate; changes in kidney function
as manifested by changes in the urine, the
blood urea nitrogen, and the phenolsulfonthalein test; and alterations in liver function as
indicated by cephalin flocculation, thymol turbidity, total protein, and bromsulfalein excretion.
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
The anticoagulant action was measured by a modification of the Lee-White procedure. After careful
venepuncture and release of the tourniquet, approximately 2 ml. of blood were drawn through
the needle. This blood and syringe were discarded,
leaving the needle in place. Approximately 5 ml. of
blood were then drawn carefully into a silicone
coated syringe, with a stop-watch being started at
this time. One ml. of blood was immediately placed
in each of three dry Pyrex tubes, 10 mm. in diameter.
Each tube was tipped gently at one minute intervals
and the end point taken as the time when the blood
held a vertical surface with the tube in a horizontal
position. The three tubes were measured simultaneously and the clotting time reported was the average
of the three tubes. By this method the average clotting time of 47 control determinations was 9 minutes, with a range from 6 to 12 minutes. Careful
adherence to this technic was maintained; all blood
specimens were drawn by the same individual and
all the end points were determined by one of two
individuals in order to obtain the maximum accuracy
possible with this method.
Prothrombin times were done by the Link-Shapiro
modification of the Quick one-stage method, using
dried rabbit lung thromboplastin.
The anticoagulant action of Paritol was compared with that of heparin by observations of
the clotting time following the intravenous administration of the sodium salt of heparin (Li-
quaemin, Roche).
The Paritol was obtained as a sterile solution
of the water soluble sodium salt which is stable
at room temperature. It was given intravenously in 1, 5, and 10 per cent solutions, allowing 5 to 10 minutes for slow administration of
the given amount. The 10 per cent solution was
found to be the most convenient dilution to use.
RESULTS
Clotting Times
Single Doses. The averages of the results obtained by following the clotting times after
single doses of 2 mg. per Kg. and 5 mg. per
Kg. of 10 per cent Paritol solutions (Lot Nos.
L-81B and 286) are shown in table 1.
TABLE 1.-Average Clotting Times Obtained After.
Single I.V. Dose Of Paritol (10% Solution)
Clotting Time in Minutes
Time After
Administration of Paritol
2 mg./Kg.
5 mg./Kg.
Average-2 curves Average-21 Curves
9
55
38
26
20
16
11
12
8
39
Control
30 min.
2 hours
4 hours
6 hours
8 hours
10 hours
12 hours
14
18
12
TABLE 2.-Average Clotting Times Obtained After
Single I.V. Dose of Heparin (10% Solution)
Time After
Administration of
Hepari
Control
30 min.
2 hours
4 hours
6 hours
Clotting Time in Minutes
0.8 mg/Kg. 1.0 mg./Kg.
Average-4 Average-3 Average-3
.-
0.5 mg./Kg.
curves
curves
curves
10
37
13
10
10
47
23
10
10
74
45
14
9
For comparison, the averages of the clotting
times obtained after the administration of heparin in single intravenous doses of 0.5, 0.8, and
1.0 mg. per Kg. are shown in table 2.
Repeated Doses. Ten patients with thromboembolic conditions have been treated with repeated doses of Paritol for periods over 48
hours. The longest period of therapy has been
eight days in each of 2 cases. The total amount
of the drug given ranged from 250 mg. in a
48 hour period to 3440 mg. in a 5 day period
as shown in table 3. Average clotting times
obtained during these periods of the repeated
administration of Paritol in amounts of 2 mg.,
3 mg., and 5 mg. per Kg. are shown in table 4.
C.IC c
Ci
I
m
.
l
cq cq
,
'-
)
oocj
c
oC
_ ___
_-
dq
-
cq
LO
bC
N
°o
m°5
CD
CD
Ip
,iCl)
_
cq~~~~~cc
cq
4
° I
O0
mI
CO
1OCe- o
'-4 CO
°0
t_
00
0
CmO
CO
0
0I
0
0
0
qmIuu0q
c
O0
OD
c
c
oo
t
o
<
oo
pp
I
I)
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
-s
-
CO
~-
,
t
-{
Cl
C-
CO
_Il
0a
-s _I -
O'
- ~
l'
-
B~~~~~~~~~~~~~~~~~~~~~~~P P bo o pp w
C-CO
0
Q4
bo
C
CO)-CO
t>C10
bo
0
bi) ho_bOh
0
0I
o
P
*C)
4)
.
n
.
QOOo
a
Wy~~C
<;
C.@0o
-
-
____
-
C) C)C)
I.
.
.
.
.
DCD0C
to 0
m-
0
0
nO
lt
-
C)CO
- --
ClC
-
m000000
CDOCl,-440
0 cO
C)
C)
cr
cr
Cl '- -
l
0
000
0
DC
c
0
-
O
O
.
C
CD1 -DC'
C
0r
0bC
-
00
00:0c
00 0
MS~
1.e
H
C
t00
0D
0
0
GoI
~~~~~~~~~~~~~~~~~~~~+
.
.b .
.~C~~.~
-
44~~DCD
CI
W-
c- -
I~
-
00
000
'
CO C
-)C
CmC)
C)C
CO
o
0
e"
FI
Ii
Cl
Iq
cd
Pi
I.
12
nu
m.Ie
u
I
0 XCO
O
oo
Oc _mto
co
m
CD "0
C
~~C
0 e II
_
-
I 110'
C-. ~~~~~~~~~~~
o
C.)
CoC
cdCO
COIO ~~~~~
CO4|'C
41
O10C-
C
10
~4
QQQ
18
12
12
1z~4
12 1G'
0o
Io
1t- 0 1
~
COO
Q0b)
u1
CN
660
c-
C
-I1~~0
C 1H__0
C H t-..I ^H
-~~~~~~~~~~-
Q 18
S 12
1
° |N)
N o
eq
mO
CV
co
e
N
es
0
O
0
0
oc4
_
oo
N -e
'0
0
00
t-.
0003
CO
t-
_I
X
eCOC
m
OO0o00
_:
eq
0
eq
-
X00
N
eq
O
t
CCO
eqeq
0O
t-
CID
cc
CO
+ eq
O0 0
CO
C
0
-
0
'0
4
C
'0
It
eq ;
eq
' u4
cmO
C
'0
0
_e ee a:t>t
tt
CD
C
e
C
s
s
t
+
'
e
0
CD
+
+~~~~~~~~~ce
+
CO
e
0
0
0
e
CO
c
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
0~~~~~~~~~
0
C0
e)
CO
oo
o
Co
I
u
sI)
aC)
e
)
eq
00
0
0
t
-4
_l
0 |~_N C|O
4
_
_,
0
0
-z
'-4-oo-.0
00
0
0
0
0
0
CO 00 '-4
-
'-i
-
0
C0
0c
0C0
0
000
'4
_
_ _
'0N
_
_
_
P-
I
!q-
CO
eq
6611
0
_ S
-o0U0
-
eq
l~t
_
0
q
'0!4eq
2 !eq'0
Y)
0
CO
'0
_J
I04
0
~
)Q)C
0
4
P4
e'0
e
0
0
~
0
_1i
O
OC o-0~
~'0COCO
O
-
0
~
004
0
0
C )
A
~
0
-0
&
CO 00q|
00
00
CD toC) C
C ,C)
C)
'0
0
0
_
O~~~~~~~~~00
O
q~ 00
-
0c
H
'
.
CD
CO
q
0
0
0o
0'0
0
0 eq
COb 'CO
10
-
*
*
'
N
est
._
'i
._
Io
U,
CO
CO
.
-
e
,qjn,IUxgqj, |q
N
+
| 'O
*oj:Iq oO
I-b
-n
0
q~n~ui~cqj~
q
0
t
r_
|'cD
q
CO
oO
cO
0
I
C
rm
C5
4c]f10
4 .:
p
110
~~
o
1
0~~c
0
1
550
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
i
C) 00 00
e
s
0
~~~~~~~~CO
N
CO
U,~~~~~~~~~~~~~~~-
1)
___q
eq
o
oo
.0$
r.
z
0
Pt~~.
c
k
z
CO CD _
_
cq cq
cq
00-koCC~
N CDC
c]
Z
CcD tCYD
z
1 s0
occo
0
CO
-Q
___
-
m_ ~~~
m
CO
CO
-z
O+
t
to
~.O
~
~
I °
-
0"
I0,"
.P
&
I~
-
10
O
.
0
.
Cd
Cd
On I ce ee
02~~~~~~
I >o~~~~~~~~~~~~~~~~~~c
<
o
(4~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~-.
t_ |
-I §
||410
CdI
10
10
P-(
uz~ ~
1
10
CO
_el
-10
4)
CO
662
0
~
~
~
-
10
10 _
0
bl10
C. W. SORENSON AND I. S. WRIGHT
Prothrombin Times. The effect of the administration of Paritol on the prothrombin time
as determined by the Link-Shapiro modification of the Quick one-stage test is shown in
table 5.
TABLE 4.-Average Clotting Times Obtained During
Maintenance Treatment With Repeated Doses of
Paritol I.V. (10% Solution)
Clotting Time in Minutes
Time After
Administration of
Paritol
2 mj g./Kg.
Aver age-22
3 mg./Kg.
Average-7
Cuirves
Curves
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
Before any Paritol
administered.....
Before next dose of
Paritol ...........
30 min........
8 hours......
10 hours......
12 hours......
5 mg./Kg.
Average-19
Cut
lies
9
8
9
114
t
50
15
13
55
12
69
k
18
15
16
TABLE 5.-Prothrombin Time Determinations after
5 mg./Kg. of Paritol I.V. (10% Solution)
Prothrombin Time in Sec.
Time After Paritol Clotting Time
in Minutes
Administration
UndilutedPlasma
Diluted-12.5%
16
23
22
17
38
47
41
39
100%
Control
30 min.
2 hours
4 hours
6 hours
7
57
32
15
14
Plasma
6.-Prothroinbin Time Determinations after
Heparin 1 mg./Kg. I.V. (10% Solution)
TABLE
Time
After
Tieparter
Administration
Clotting
C
Time
Clotting Time
in Minutes
Prothrombin
Undiluted100% Plasma
Time
in
Sec.
Diluted-12.5%
Plasma
Control
10
15
37
30 min.
2 hours
74
45
14
10
24
19
16
42
39
39
4 hours
6 hours
For comparison, the prothrombin times obtained following the administration of heparin
are shown in table 6.
The Effect of Paritol
on
Other Laboratory Deter-
minations
Table 3 summarizes the laboratory determinations done on the 10 patients given re-
663
peated doses of Paritol for periods over 48
hours.
Hemoglobin, Red Blood Cell Count, and White
Blood Cell Count. No change in these values has
been observed that could be attributed to Paritol.
Platelets. No change in the platelets was observed as determined by the estimation of the
number of platelets in relation to red blood
cells on stained smears.
Kidney Function. There was no change noted
in the urine with the administration of Paritol.
Case 21, a patient with no recognized renal
disease prior to administration of the drug,
showed a rise in the blood urea nitrogen from
11 mg. to 26 mg. per 100 cc. after receiving
1680 mg. of Paritol over a period of four days.
During this same time he was receiving Thiomerin 2 ml. daily. The Paritol was discontinued
and the blood urea nitrogen continued to rise
to 30 mg. per 100 cc. Three days later, Thiomerin was stopped and the blood urea nitrogen
promptly fell to within normal range. The data
indicated that the urea retention was due more
probably to the action of the Thiomerin than
of the Paritol.
Case 28, a patient with pulmonary infarction,
rheumatic heart disease, congestive heart failure, and chronic nephritis with a consistently
elevated blood urea nitrogen of about 30 mg.
per 100 cc. was given 380 mg. of Paritol in
two days. There was a rise in the blood urea
nitrogen to 54 mg. per 100 cc., following which
the Paritol was discontinued. The blood urea,
nitrogen then fell to the pretreatment level of
around 30 mg. per 100 cc. Four hundred eighty
mg. of Paritol was then administered during
three days and the blood urea nitrogen rose to
60 mg. per 100 cc. After the Paritol was discontinued the blood urea nitrogen gradually
returned to the former level (30 mg. per 100
cc.). The Paritol was considered to be responsible for the increased urea retention occurring
in the presence of decreased kidney function.
There was no evidence that the drug had cause(1
a further permanent decrease in the renal function.
Liver Function. One patient (case 23) had
arteriosclerotic heart disease, auricular fibrillation, congestive heart failure, multiple
664
A SYNTHETIC ANTICOAGULANT
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
pulmonary infarctions, and evidence of early
cirrhosis of the liver. Before Paritol was administered, the cephalin flocculation was elevated to
12 units (normal, below 5) and the thymol
turbidity was 6 units (normal, below 5). During the period he received the drug the cephalin
flocculation rose to 18 units and the thymol
turbidity to 9 units. Twenty-five days after
the treatment, the cephalin flocculation was 7
units and the thymol turbidity was 7 units.
This patient was extremely ill during the first
two weeks of hospitalization and it was impossible to determine with certainty whether the
drug was responsible for the evidence of increased liver damage. On a clinical basis, however, the impairment of liver function might
well have been due to his serious illness and
not to a toxic effect of the drug.
No other patients developed any evidence of
liver damage following the administration of
Paritol.
Effect of Paritot on the Blood Pressure, Pulse,
and Respirations
The pulse, respiratory rate, and blood pressure determinations during and after the administration of Paritol to 13 patients are shown
in table 7.
The systolic blood pressure of patient 7 decreased 20 mm. Hg during the administration
of 350 mg. (6 mg. per Kg.) of the drug without a corresponding decrease in the diastolic
pressure (120/75 to 100/70). Two days later
his pressure was found to be at the reduced
level (100/65). A second dose of 400 mg. (7
mg. per Kg.) of the drug produced no change
in the pressure. Patient 9 showed no change
in blood pressure with the first administration
of 400 mg. (4.2 mg. per Kg.) of Paritol. Two
days later he was given 325 mg. (3.5 mg. per
Kg.) and with this there was a transient fall
in the systolic and diastolic pressures (126/66
to 106/54) associated with flushing of the
face and a feeling of fullness in the epigastrium.
These minor manifestations disappeared spontaneously within fifteen minutes after the injection was completed.
Reactions to Paritol
Of the 35 patients to whom Paritol has been
given, 3 have shown immediate reactions: one
of these was severe, two were mild. The severe
reaction occurred in a 40 year old woman (patient 2) with rheumatic heart disease, auricular fibrillation, mitral stenosis, and an embolus
to the left popliteal artery. She had received
three injections of Paritol in amounts of 125
mg. (2 mg. per Kg.), 185 mg. (3 mg. per Kg.),
and 185 mg. on successive days without reaction, although she later stated that with two
of these she had felt "uneasy." The fourth
dose, administered the next day, was 315 mg.
of a 1 per cent solution (5 mg. per Kg.). About
five minutes after the completion of the injection the patient developed nausea, vomiting,
abdominal cramps, defecation, oppression in
the precordial area, pallor, sweating, bradycardia and a fall in the blood pressure to imperceptible levels. These manifestations subsided rapidly following the administration of
of 0.3 mg. of epinephrine subcutaneously
and within 30 minutes the blood pressure had
returned to normal levels and the patient was
feeling much improved. It is noteworthy that
this patient developed similar, but less severe
reactions to the intravenous administration of
papaverine and had a somewhat similar reaction to magnesium sulfate used in determining the circulation time.
Two patients (cases 7 and 24) developed
a reaction following Paritol administration
which the authors have not previously encountered with any drug. This consisted of the
development within 15 minutes of "pins and
needles" sensations in the hands and feet followed by a moderate swelling of the hands,
and to a lesser degree of the feet. This was
associated with stiffness of the finger joints
and inability to close the fingers completely.
In one patient this swelling subsided spontaneously in about eight hours. In the second,
the administration of 0.3 mg. of epinephrine
subcutaneously was followed by a decrease in
the symptoms of tingling in the hands and feet
and stiffness of the fingers within 20 minutes.
The swelling gradually disappeared within
about six hours. Neither patient showed any
evidence of urticaria elsewhere nor did they
develop respiratory signs or symptoms. Neither
gave personal or family histories of allergic
manifestations.
One patient with an acute pulmonary in-
TABLE 7.-Blood Pressure, Pulse, and Respiration Changes during Paritol Administration in 13 Cases
#3 2mg./Kg.
# 4 Smg./Kg.
#5 6mg/Kg.
Time
ls
B.P.
110/72
Control
Start injection
4 min.
6 min.
8 min.
10 min.
End Injection
2 min.
5 min.
10 min.
15 min.
20 min.
116/80
112/78
120/84
118/80
118/80
P
R
B.P.
P
R
116/66
120/70
122/74
76
72
76
18
20
20
110/88
120/80
118/84
122/88
50
74
60
58
16
16
20
16
128/74
118/68
88
80
28
22
125/68
80
20
118/68
64
20
118/80
124/80
120/84
118/82
118/86
56
60
64
58
54
16
16
16
16
16
p
R
B.P.
P
R
B.P.
84
16
130/70
72
20
20
20
16
16
16
80
80
78
78
80
130/75
130/70
132/75
140/80
130/70
68
68
72
80
76
20
16
20
20
20
# 6 8mg/Kg.
# 7 6mg/Kg.
# 7 7mg./Kg.
#8 6mg./Kg.
#9 Smg./Kg.
Time
P
R
BRP.
P
R
B.P.
P
R
B.P.
P
R
120/75
120/78
118/74
115/75
100/70
104/68
60
60
60
78
96
92
16
16
16
16
12
16
96/64
100/65
98/65
98/65
98/62
100/68
68
68
64
68
68
68
20
20
20
24
20
20
134/86
150/86
120/80
115/78
132/90
130/90
92
94
96
88
100
96
24
28
20
20
16
20
120/78
126/70
120/76
120/76
122/76
118/68
76
76
80
76
82
80
16
16
16
16
96/68
106/72
104/74
104/72
100/72
68
64
64
64
68
16
16
20
20
16
98/64
98/64
96/62
72
72
72
20
20
20
138/90
100
20
118/70
82
16
130/86
92
20
122/74
84
16
68
20
132/88
92
20
B.P.
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
Control
Start Injection
4 min.
6 min.
8 min.
10 min.
End Injection
2 min.
5 min.
10 min.
15 min.
20 min.
96/62
#9b 5mg./Kg.
# 11 5 mg/Kg.
# 10 Smg./Kg.
Time
B.P.
126/66
Control
Start Injection
4 min.
6 min.
8 min.
10 min.
End Injection
2 min.
5 min.
10 min.
15 min.
20 min.
l~
P
100
# 125 mg./Kg.
P
R
B.P.
P
R
88
16
150/90
18
18
18
18
18
18
134/100
100 I 24
160/80
160/80
150/100
150/100
92
92
88
92
92
92
134/100
130/94
112
100
24
24
155/78
92
18
132/98
96
24
155/70
150/95
148/100
150/100
B.P.
135/100
R
B.P.
P
R
24
148/72
148/76
68
70
68
68
64
18
16
16
16
68
68
68
16
16
16
68
16
118/64
118/70
106/54
104
16
16
16
106/60
110/70
88
88
20
16
150/100
114/74
118/74
118/74
92
92
16
16
150/100
92
18
126/94
100 I 20
168/78
156/70
88
16
150/100
92
18
128/94
100
142/66
84
100
20
#1'[4 5mg/Kg.
# 13 Smg./Kg.
Time
16
16
18
# 15 Smg./Kg.
B.P.
p
R
B.P.
P
R
124/70
124/72
130/70
126/70
128/70
126/70
60
60
64
64
64
64
16
16
16
16
16
16
155/80
160/86
165/80
158/78
98
96
104
104
18
18
20
20
156/78
100
20
128/70
124/64
120/68
68
68
68
16
16
16
144/76
104
20
120/66
68
16
150/78
-1
B.P.
P
R
170/90
180/94
170/90
120
112
120
24
22
24
164/88,
116
24
166/88
120
24
176/90
120
24
210/111
124
24
I-
Control
Start Injection
4 min.
6 min.
8 min.
10 min.
End Injection
2 min.
5 min.
10 min.
15 min.
20 min.
665
100
20
6A SYNTHETIC ANTICOAGULANX1
i66`
farction and alcoholism was nauseated on admission. The administration of Paritol appeared
to increase the nausea and vomiting. However,
after his nausea had subsided, repeated doses
of the same amount of Paritol were given without causing any symptoms.
In 2 patients, small extravasations of Paritol
outside the veins produced a moderate amount
of pain, swelling, increased heat, and redness
in a localized area which lasted about 24 hours.
No slough occurred.
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
DIscussION
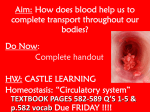
Paritol is a polysulfuric acid ester of polyanhydromannuronic acid. The structural formula compared with that of heparin is shown
in figure 1. Seifter and Begany (8) have reHEPARIN
H
HH
H
OH
H
CH2OH
O-SO H
-0
°I
0--
H
0
COOH
Glucuronic
HHSO OH
H
Glucosomine
Acid(v
n
PARI TOL
H
COOH
H
O
H
OH
HSO-O
0
H
0-SO
H
COOH
Mannuronic Acid
H
OH
H3
0
H
o
H
H
Mannuronic
H
Acid
n
FIG. 1. Formula of hepariii compared with
that of Paritol.
ported that in animals its toxicity was no
greater than that of heparin and much less
than that of other synthetic polysaccharide
sulfuric acid esters that were tested. The halflethal dose in mice determined as mg. per Kg.
were: heparin, 1500-2000; Paritol 1898; cellulose sulfuric ester, 100; and oxycellulose sulfuric ester, 200. They found the anticoagulant
activity of Paritol to be about one-seventh
that of heparin.
Preliminary studies on the action of Paritol9
(formerly known as Heparinoid), demonstrated
that it had definite anticoagulant activity when
administered intravenously to humans. These
preliminary observations with the preparations
then available (Lots 137 and 289) indicated
that it was about one-thirteenth as active as
the sodium salt of heparin (Liquaemin, Roche)
in prolonging the clotting times. Extension of
the previously reported studies with more recent preparations of Paritol (Lots 286 and
L-81-B) indicate that in man the present potency is about one-seventh that of heparin.
More important, however, is the fact that
prolongation of the clotting time continues for
8 to 12 hours after Paritol administration,
while with crystalline heparin the action is
demonstrable for only 4 to 5 hours after intravenous administration. It has therefore been
possible to treat patients with thromboembolic diseases with intravenous doses of Paritol
administered at intervals of 8 to 12 hours and
with improvement in their clinical conditions.
This represents an advantage over the use of
heparin for intermittent intravenous therapy
where the dose must be repeated about every
4 hours. The local reactions produced by Paritol when extravasation occurred outside the
veins have precluded its use by the intramuscular or subcutaneous route.
The data on case 28 appears to demonstrate
that in the presence of decreased kidney function and an elevated blood urea nitrogen, Paritol caused further urea retention. Seifter and
Begany8 found that in animals about 25 per
cent of the administered dose of Paritol is excreted in the urine. The remainder appears to
be inactivated in the blood and the inactivated
product picked up by the reticuloendothelial
system. The manner in which this polysaccharide may interfere with urea excretion in a
damaged kidney requires more study. Until
further experience is obtained, however, Paritol
should be used with caution in the presence of
decreased kidney function.
The mechanism of the other reactions to
Paritol here noted are also at present obscure.
The explanation of the severe reaction in case
2 is complicated by the fact that the patient
developed reactions to other drugs given intravenously. However, the reaction has some
of the toxic manifestations of other of the sul-
C. W. SORENSON AND I. S. WRIGHT
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
furic acid esters of polysaccharides. Also in
case 9 there was a transient moderate fall in
the blood pressure during the administration
of Paritol associated with mild flushing of the
face. Therefore, the toxicity of Paritol must
be evaluated with a larger series of carefully
studied patients before its general use can be
advocated. Such a study is now in progress by
the Committee on Ant icoagulants of the American Heart Association.
The swellings limited to the hands and feet
of 2 patients (cases 7 and 24) would appear
to be vascular in nature. The exact mechanism
responsible for these changes which appeared
to be limited too the peripheral vessels is obscure.
CoN CLUSIoNS
1. The polysulfuric acid ester of polyanhydromannuronic acid (Paritol) produces a significant prolongation of the clotting time when
administered intravenously to humans.
2. The duration of anticoagulant effect of
Paritol is from two to three times as long as
that of heparin.
3. When compared mg. per Kg. with reference to the maximum clotting time obtained
the effect of Paritol as presently prepared is
approximately one-seventh that of heparin.
4. This may be compensated by administering Paritol in doses sufficient to produce clotting times comparable to those obtained with
heparin.
5. Repeated doses of Paritol at 8 to 12 hour
intervals have been given for periods up to
eight days with evidence of satisfactory maintenance of anticoagulant therapy.
6. Paritol produces a slight prolongation of
the prothrombin time similar to that produced
by heparin. This is proportional to the effect
on the clotting time.
CW-0
7. Paritol appeared to cause a further rise
in the blood urea nitrogen in a patient with an
elevated blood urea nitrogen due to kidney
disease. The drug should therefore be used
with caution in patients with serious kidney
damage.
8. Of 35 patients to whom Paritol has been
given, 3 others have developed reactions. One
was severe, with generalized symptoms including vascular collapse. Two have had mild reactions characterized by swelling of the hands
and feet, which are suggestive of some vascular
change in the peripheral vessels. The mechanism of these reactions is not clear.
9. Further studies with Paritol are justified
in order to evaluate more completely its usefulness as a rapidly acting anticoagulant for
the treatment of thromboembolic diseases.
REFERENCES
1 JORPES, E.: The chemistry of heparin. Biochem. J.
29: 1816, 1935.
On heparin, its chemical nature and properties. Acta med. Scandinav. 88: 427, 1936.
3~ , AND BERGSTROM, S.: Heparin: A mucoitin
polysulfuric acid. J. Biol. Chem. 118: 447, 1937.
4BERGSTROM, S.: Uber Polysaccharidester-schwefelsauren mit Heparinwirkung. Ztschr. Physiol.
Chem. 238: 163, 1936.
5 ASTRUP, T., GALSMAR, I. AND VOLKERT, M.: Polysaccharide sulfuric acids as anticoagulants. Acta
physiol. Scandinav,. 8: 215, 1944.
6
, AND PIPER, J.: Cellulose sulfuric acids as
anticoagulants. Acta physiol. Scandinav. 9: 351,
1945.
7CHARGAFF, E., BANCROFT, F. I., AND STANLEYBROWN, Al.: Studies on the chemistry of blood
coagulation. II. On the inhibition of blood clotting by substances of high molecular weight. J.
Biol. Chem. 115: 155, 1936.
8 SEIFTER, J., AND BEGANY, A. J.: Studies on the
action of a synthetic heparinoid. Am. J. M. Sc.
216:,234, 1948.
9 SORENSON, C. W., SEIFTER, JOSEPH, AND WRIGHT,
I. S.: A new synthetic anticoagulant (heparinoid). Preliminary report of its action in humans.
Bull. New York Acad. AMed. 25: 448, 1949.
2
A Synthetic Anticoagulant: A Polysulfuric Acid Ester of Polyanhydromannuronic Acid
(Paritol): Experience with Its Use in Man
C. W. SORENSON and IRVING S. WRIGHT
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
Circulation. 1950;2:658-667
doi: 10.1161/01.CIR.2.5.658
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1950 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/2/5/658
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not
the Editorial Office. Once the online version of the published article for which permission is being
requested is located, click Request Permissions in the middle column of the Web page under Services.
Further information about this process is available in the Permissions and Rights Question and Answer
document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/