Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
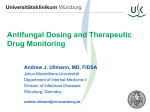
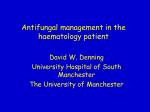
ANSWER TO THE PHOTO QUIZ Anthony Amoroso, Section Editor A Patient With Ulcerated Nodules on His Face (See page 839 for the Photo Quiz.) Figure 2. Histologic section from right mandibular region skin biopsy (hematoxylin-eosin stain, ×100 magnification), demonstrating squamous cell carcinoma. The image shows a dermal proliferation with nuclear atypia and numerous mitotic figures (small arrow). The cells have abundant eosinophilic cytoplasm with intracellular bridging confirming the squamous lineage (large arrow). Figure 1. Skin lesions on the right side of the face; diffuse nontender, hard, ulcerated nodules with necrosis that oozed serous fluid. Diagnosis: Cutaneous squamous cell carcinoma (SCC) likely due to the long-term use of voriconazole. In some clinical settings, ulcerated nodular skin lesions can be concerning for a cutaneous nontuberculosis mycobacterial or fungal infection (Figure 1). However, in our patient, the histological sections of skin from the right mandibular region demonstrated dermal proliferation with nuclear atypia and numerous mitotic figures typical of SCC (Figure 2). In addition, the cells had abundant eosinophilic cytoplasm with intracellular bridging confirming the squamous lineage. The overlying surface epithelium was relatively unremarkable and all fungal and nontuberculosis mycobacterial specific stains and cultures were negative. A computed tomographic (CT) scan of the head and neck revealed periauricular skin thickening compatible with SCC with focal dermal lesions along the face in addition to necrotic lymphadenopathy with apparent invasion into the floor of the mouth. Based on the biopsy and CT findings, the patient was diagnosed with stage IV cutaneous SCC (T4N1M0, with various bilateral cervical lymph nodes). He underwent his initial treatment with local radiotherapy (40 Gy in 16 fractions), which was complicated by hemoptysis. His chronic fungal infection, decreased pulmonary function, and overall poor performance status prohibited the use of systemic myelosuppressive chemotherapy; therefore, a palliative course of cetuximab (epidermal growth factor receptor inhibitor) was administered. Unfortunately, despite these interventions, his SCC progressed over a period of several months and eventually led to airway compromise and death. Voriconazole is a broad-spectrum second-generation azole that exerts its antifungal activity by inhibiting ergosterol synthesis [1]. It has activity against all Candida species, most Aspergillus species, Fusarium species, the endemic mycoses, and Scedosporium apiospermum [1]. Voriconazole is generally well tolerated, but side effects can include self-limiting visual disturbances ( photophobia, altered ANSWER TO THE PHOTO QUIZ • CID 2014:58 (15 March) • 901 color discrimination, and blurred vision) and elevations in hepatic enzymes [1]. Of note, this antifungal agent can also cause a generalized rash in up to 8% of patients, and more specifically, voriconazole has been associated with a phototoxicity-related rash that manifests as a sunburn-like erythema in 2% of patients [2, 3]. The mechanism of action for voriconazole-associated phototoxicity is largely unknown. One theory is that voriconazole inhibits all-trans retinol metabolism and leads to the accumulation of phototoxic retinoid compounds [3]. Another explanation is that the principal metabolite of voriconazole, voriconazole N-oxide, absorbs the ultraviolet A wavelength (the action spectrum for most phototoxic reactions) and induces this phenomenon [4]. It is hypothesized that voriconazole-induced phototoxicity may account for the recent reports linking the long-term use of this antifungal agent to the development of cutaneous SCC and melanoma [5–12]. In the largest case series, Clancy et al reported 36 patients with skin cancer following the long-term use of voriconazole [5]. All patients reported were white, the majority were men, the median length of voriconazole use ranged from 2 to 60 months, and 3 died as a result of their skin cancer [5]. The use of immunosuppressive therapies, underlying human immunodeficiency virus (HIV) infection, and residing in regions of the United States with high sun exposure appear to be risk factors for the development of voriconazole-associated SCC [6–8, 10]. Our patient was not infected with HIV or on immunosuppressive medications. However, we suspect that his residence in Virginia (a region of the United States with higher levels of sun exposure and ultraviolet index compared to northwestern states such as Washington and Oregon) in addition to his severely decreased pulmonary function and chronic fungal infection may have been put him at risk for this malignancy [13]. Although further studies are needed to define the causal relationship between voriconazole use and SCC, when prescribing this antifungal agent, physicians should advise patients to limit sunlight exposure and have new skin lesions evaluated promptly. Notes Acknowledgments. In fond memory of J. A. M., who reminded us that medicine is still an art, and that every day is a blessing. Disclaimer. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of the Army, Uniformed Services University, Department of Defense, or the US government. This work was prepared as part of D. C. D., J. D. M., E. H., J. M., and T. J. W. official duties. Title 17 U.S.C. 101 defines a US government work as a work prepared by a military service member or employee of the US government as part of that person’s official duties. Reviewed by the WRNNMC public affairs office in September 2013. Potential conflicts of interest. All authors: No reported conflicts. 902 • CID 2014:58 (15 March) • ANSWER TO THE PHOTO QUIZ All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed. Dennis C. Drinkwater,1 Jan Davidson-Moncada,2 Emily Heckendorn,3 Janet Myers,4 and Timothy J. Whitman5 1 Department of Internal Medicine, Walter Reed National Military Medical Center (WRNMMC), 2Department of Hematology/Oncology, National Institutes of Health, and 3Department of Pathology, WRNMMC, Bethesda, Maryland; 4Department of Pulmonary Medicine, United States Naval Hospital Okinawa, Japan; and 5 Department of Infectious Diseases, WRNMMC, Bethesda, Maryland References 1. Johnson LB, Kauffman CA. Voriconazole: a new triazole antifungal agent. Clin Infect Dis 2003; 36:630–7. 2. Rubenstein M, Levy ML, Metry D. Voriconazole-induced retinoid-like photosensitivity in children. Pediatr Dermatol 2004; 21:675–8. 3. Denning DW, Griffiths CM. Muco-cutaneous retinoid-effects and facial erythema related to the novel triazole antifungal agent voriconazole. Clin Exp Dermatol 2001; 26:648–53. 4. Murayama N, Imai N, Nakane T, et al. Roles of CYP3A4 and CYP2C19 in methyl hydroxylated and N-oxidized metabolite formation from voriconazole, a new anti-fungal agent, in human liver microsomes. Biochem Pharmacol 2007; 73:2020–6. 5. Clancy CJ, Nguyen MH. Long-term voriconazole and skin cancer: is there cause for concern? Curr Infect Dis Rep 2011; 13:536–43. 6. Vadnerkar A, Nguyen MH, Mitsani D, et al. Voriconazole exposure and geographic location are independent risk factors for squamous cell carcinoma of the skin among lung transplant recipients. J Heart Lung Transplant 2010; 29:1240–4. 7. Ibrahim SF, Singer JP, Arron ST. Catastrophic squamous cell carcinoma in lung transplant patients treated with voriconazole. Dermatol Surg 2010; 36:1752–5. 8. Epaulard O, Saint-Raymond C, Villier C, et al. Multiple aggressive squamous cell carcinomas associated with prolonged voriconazole therapy in four immunocompromised patients. Clin Microbiol Infect 2010; 16:1362–4. 9. Cowen EW, Nguyen JC, Miller DD, et al. Chronic phototoxicity and aggressive squamous cell carcinoma of the skin in children and adults during treatment with voriconazole. J Am Acad Dermatol 2010; 62:31–7. 10. Brunel AS, Fraisse T, Lechiche C, et al. Multifocal squamous cell carcinomas in an HIV-infected patient with a long-term voriconazole therapy. AIDS 2008; 22:905–6. 11. Vanacker A, Fabre G, Van Dorpe J, et al. Aggressive cutaneous squamous cell carcinoma associated with prolonged voriconazole therapy in a renal transplant patient. Am J Transplant 2008; 8:877–80. 12. McCarthy KL, Playford EG, Looke DF, et al. Severe photosensitivity causing multifocal squamous cell carcinomas secondary to prolonged voriconazole therapy. Clin Infect Dis 2007; 44:e55–6. 13. National Oceanic and Atmospheric Administration. National Weather Service Climate Prediction Center. Available at: http://www.cpc.ncep. noaa.gov/products/stratosphere/uv_index/uv_current_map.shtml. Accessed 27 September 2013. Correspondence: Timothy J. Whitman, DO, Department of Infectious Diseases, Walter Reed National Military Medical Center, 8901 Wisconsin Ave, Bethesda, MD 20889 (timothy.j. [email protected]). Clinical Infectious Diseases 2014;58(6):901–2 Published by Oxford University Press on behalf of the Infectious Diseases Society of America 2014. This work is written by (a) US Government employee(s) and is in the public domain in the US. DOI: 10.1093/cid/cit713