Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
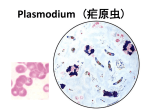
HUWEL LIFESCIENCES PVT. LTD. Thriving on Science MALARIAL PARASITE DETECTION- PLASMODIUM SPS (P. VIVAX AND P. FALCIPARUM) Disease overview: Plasmodium is commonly known as the malaria parasite which is a large genus of parasitic protozoa. Malaria, a deadly disease, is the infection caused by plasmodia infection. The most common forms of human malaria are caused by Plasmodium falciparum, P. vivax, P. knowlesi, and P. malariae. P. falciparum, common in sub-Saharan Africa, and P. knowlesi, common in Southeast Asia, are especially dangerous. Mosquitoes of the genera Culex, Anopheles, Culiseta, Mansonia and Aedes may act as vectors. The known vectors for human malaria (more than 100 species) belong to the genus Anopheles. Only the female mosquitoes bite. The presence of the parasite in human populations caused selection in the human genome in a multitude of ways, as humans have been forced to develop resistance to the disease. Some scientist suggest that sickle-cell disease and thalassaemia could offer protection from malaria. Of the six malarial parasites, P. falciparum causes the most fatal and medically severe form. Malaria is prevalent in tropical countries with an incidence of 300 million per year and a mortality of 1 to 2 million per year. Roughly 50% of all malarial infections are caused by P. falciparum. P. falciparum : Plasmodium falciparum is a protozoan parasite, one of the species of Plasmodium that cause malaria in humans. It is transmitted by the female Anopheles mosquito. Malaria caused by this species (also called malignant malaria) is the most dangerous form of malaria, with the highest rates of complications and mortality. Almost every malarial death is caused by P. falciparum. Artemisinin-based combination therapies (ACTs) are the recommended first line antimalarial treatments for uncomplicated malaria caused by P. falciparum. As second-line anti-malarial treatment, when initial treatment does not work or stops working, an alternative ACT known to be effective in the region is recommended, such as: Artesunate plus tetracycline or doxycycline or clindamycin / Quinine plus tetracycline or doxycycline or clindamycin. Any of these combinations are to be given for 7 days. P. vivax: Plasmodium vivax is a protozoal parasite and a human pathogen. The most frequent and widely distributed cause of recurring (Benign tertian) malaria, P. vivax is one of the five species of malaria parasites that commonly infect humans. It is less virulent than Plasmodium falciparum, but vivax malaria can lead to severe disease and death due to splenomegaly (a pathologically enlarged spleen). P. vivax is carried by the female Anopheles mosquito, since it is only the female of the species that bite. Treatment is different from that for p. falciparum. Chloroquine remains the treatment of choice for vivax malaria, except in Indonesia's Irian Jaya (Western New Guinea) region and the geographically contiguous Papua New Guinea, where chloroquine resistance is common (up to 20% resistance). Chloroquine resistance is an increasing problem in other parts of the world including India. Symptoms The symptoms of uncomplicated malaria can be rather non-specific and the diagnosis can be missed if health providers are not alert to the possibility of this disease. Since untreated malaria can progress to severe forms that may be rapidly (<24 hours) fatal, malaria should always be considered in patients who have a history of exposure (mostly: past travel or residence in disease-endemic areas). The most frequent symptoms include fever and chills, which can be accompanied by headache, myalgias, arthralgias, weakness, vomiting, and diarrhea. Other clinical features include splenomegaly, anemia, thrombocytopenia, hypoglycemia, pulmonary or renal dysfunction, and neurologic changes. The clinical presentation can vary substantially depending on the infecting species, the level of parasitemia, and the immune status of the patient. Infections caused by P. falciparum are the most likely to progress to severe, potentially fatal forms with central nervous system involvement (cerebral malaria), acute renal failure, severe anemia, or acute respiratory distress syndrome. Other species can also have severe manifestations. Complications of P. vivax malaria include splenomegaly (with, rarely, splenic rupture), and those of P. malariae include nephrotic syndrome. HUWEL LIFESCIENCES PVT. LTD. Thriving on Science Preferred sample: Specimens Whole Blood: 3-5 ml collected in an EDTA tube. Transport: To be transported at 4 degrees Methodology: Qualitative DNA PCR for the detection of Malaria is performed using genomic DNA extracted from whole blood sample. This assay detects and discriminates all four malaria-causing Plasmodium species (P. falciparum, P. vivax, P. ovale and P. malariae). Sensitivity: 5-10 copies Interpretive DATA: A negative result does not rule out the presence of PCR inhibitors in the patient specimen or Plasmodium sps DNA concentrations below the level of detection by the assay. Note: Although all precautions are taken and results cross checked during Nucleic acid tests, the currently available data indicates the technical error rate for all such analysis is ~1-2%. The results assume that all the information regarding the patient and the sample are correct and should be interpreted and acted upon in the light of the information noted above. References: ARUP Laboratories: www.aruplab.com CDC: www.cdc.gov NIH: www.nih.gov Mayo clinic: www.mayoclinic.org Other journals, articles and websites