Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
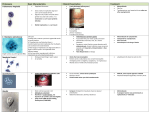
“Ensuring quality and access for malaria diagnosis: how can it be achieved?” Nat Rev Microbiol. 2006 Sep;4(9 Suppl):S7-20. Amy Storfa 3/23/2007 Background • Symptoms (fever, rigors, headache) overlap with presentations of other febrile illnesses • P. falciparum can often lead to coma and death; other Plasmodium spp. cause acute severe illness but rarely fatal • Despite microscopy, most diagnoses with subsequent treatment made based on symptoms • Estimates of malaria deaths estimated at ~1-2 million/y – 350-500 million cases of malaria occur annually • Programs developed for treatment but accurate diagnosis not emphasized Background • Some countries maintain microscopy-based diagnosis programs (e.g. India) • BUT, microscopy largely unavailable to providers of most patients with tropical febrile illness • Requires organized health system, supplies, reagents, good microscopes, maintenance, competence, ability to make blood films • Antigen-detecting rapid diagnostic tests (RDTs) first introduced in early 1990s and used sparingly in malaria endemic areas Background • More recently, drug resistance is increasing, necessitating switch to artemisinin-based combination therapy (ACT), more $ • Shift has led to upsurge in use of RDTs • But many areas (particularly sub-Saharan Africa) still rely on symptom-based diagnosis Early diagnosis • Differential diagnosis of febrile tropical illness: respiratory tract infxn, typhus, viral illness, meningitis • Early detection/treatment likely to occur if microscopy services are offered within 15-20 minutes of residence • ACT ~$1.60 per course • RDT ~$0.55 to $1.00 each • Overall funding for research and development – Diagnosis receives <1%, vs 37% for drug development Advantages: -Improved management of non-malarial disease -Savings in drug costs -Improved adherence to therapy Implications on health care system • • • • Preparation and interpretation can be poor Requires adequate level of training, supervision Appropriate instructions developed Requires temperature controlled distribution and storage facilities • Need to be stable, simple to use, able to detect clinically significant disease (100 parasites/uL) • Need quality assurance and control Bell et al. Nature Reviews Microbiology 4, S7–S20 (September 2006) | doi:10.1038/nrmicro1525 Bell et al. Nature Reviews Microbiology 4, S7–S20 (September 2006) | doi:10.1038/nrmicro1525 1. HRP2 2. pLDH 3. aldolase P. falciparum HRP-2 pLDH Further development/study needed • Field trials needed to see how tests perform in field • WHO initiative to test accuracy and stability of RDTs • Previous studies based on various RDT types in different clinical and epidemiological settings are difficult to compare • Difficult to generate conclusive comparisons of RDT performance • Timing of treatment and effectiveness of therapy also complicates comparative studies – pLDH is rapidly cleared but HRP2 persists for weeks Malaria Review Malaria review • Plasmodium: four species – – – – P. falciparum (~45%) P. vivax (~45%) P. ovale (rare, <5%, limited to W. Africa) P. malariae (<5%) • Acquired via anopheles mosquito Malaria review: multiple forms • Trophozoites (=ring forms): most numerous form to see in peripheral blood, ring like structure (<1/2 diameter of cell), progressively enlarge and mature to… • Schizont: multinuclear structure, appear as intraerythrocytic collection of merozoites (each with its own nucleus) • Gametocyte: mononuclear structure occupying >1/2 the red cell, usually amoeboid in shape and nearly fills entire RBC Life cycle • Mosquitoes inject sporozoites, divide in liver into schizonts (containing merozoites) • Merozoites infect RBC and then become trophozoites • Again divide into merozoites – Can infect more RBCs or become gametocytes (ingested by mosquitoes) Malaria review • Infects RBCs; causes intermittent hemolysis with paroxysmal fevers • Fever q48 h (tertian fever): P. falciparum, P. ovale; P. vivax • Fever q72 h (quartan fever): P. malariae • Examine thick (for screening) and thin (for species identification) films Malaria review • Signs/symptoms – Splenomegaly – Periodic shaking chills (rupture of RBCs) followed by spiking fevers (merozoites penetrating other RBCs) – Sweats – Anorexia – Joint pain P. falciparum • Malignant tertian fever because potentially lethal • Must be identified • Usually only early ring forms and gametocytes seen – Ring forms: may have double chromatin dots, may be multiply infected; accole or applique forms present; less than 1/5 size of RBC – Gametocytes: banana shaped • Infected red cells NOT enlarged, infects RBCs of all stages of maturation P. falciparum • Acute intravascular hemolysis with hemoglobinuria (“blackwater fever”) • Infected RBCs have “sticky knobs” leading to sludging, infarcts of brain, kidneys • With no treatment, patients either die or spontaneously resolve within one year P. falciparum P. vivax and P. ovale • Benign tertian fever • Morphologically very similar • P. ovale very rare, confined to Western Africa • Both infect young RBCs and appear enlarged and pale • All stages seen (early and developing rings, schizonts, gametocytes) P. vivax and P. ovale • Schuffner’s dots may be present • Gametocytes are amoeboid shaped, not banana • Schizonts have 12-14 merozoites P. malariae • Associated with nephrotic syndrome • Infects older erythrocytes, normal to small sized RBCs • No Schuffner’s dots • All stages seen • Schizonts have 6-12 merozoites, rosette pattern • Coarse pigment may be present • Occasional band forms (trophozoite form) seen • Low grade cryptic infections can occur up to 40 y P. malariae Malaria and RBC associations • Hemoglobin S trait (HbSA) protective against P. falciparum • Duffy antigens mediate attachment of P. vivax (Duffy negative patients protected from P. vivax) • Glucose-6-phosphate dehydrogenase deficiency protects against ALL Plasmodium spp. References • • • Bell D et al. “Ensuring quality and access for malaria diagnosis: how can it be achieved?” Nat Rev Microbiol. 2006 Sep;4(9 Suppl):S7-20. Jones SL. Clinical Laboratory Pearls. Lippincott Williams and Wilkins, 2001. Mais DD. Quick Compendium of Clinical Pathology. ASCP Press, 2005.