Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
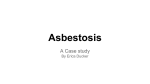
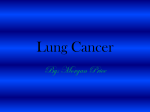
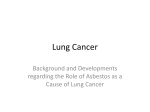
How toTreat www.australiandoctor.com.au PULL-OUT SECTION inside Complete How to Treat quizzes online (www.australiandoctor.com.au/cpd) to earn CPD or PDP points. Asbestos-related lung conditions Other occupational lung diseases Assessment Investigations Management The authors Dr Subash Srikantha respiratory and sleep specialist in private practice, St Leonards, Liverpool and the Woolcock Clinic, Glebe, NSW; and conjoint lecturer, school of medicine, University of NSW. Occupational lung diseases Background IN this industrialised era, workers are exposed to hundreds of potentially hazardous materials, with the associated risk of developing occupational-related health conditions. Increasingly, environmental exposures are being recognised as an important cause of pulmonary disease. Occupational lung disease is one of the leading causes of work-related death and disability in Australia. Causal factors include the inhalation of irritant chemical vapours and gases, organic and inorganic dusts, sensitising agents and toxic fumes, which adversely affect both the upper and lower respiratory tracts. Australia was the world’s largest Table 1: Anatomical location of occupational diseases Anatomical location Examples of occupational diseases Upper airways Rhinitis, laryngitis, nasal ulceration, cancer of the nasopharynx Conducting airways Occupational asthma, bronchitis, bronchiolitis, COPD, bronchial cancer Lung parenchyma Pneumoconiosis (silicosis, asbestosis), lung cancer Pleura Pleural plaques, diffuse pleural thickening, pleural effusions, mesothelioma asbestos user per capita in the world during the 20th century. This resulted in a significant health burden to the workers who were mining, processing or using asbestos products. Due to the long latency from exposure to disease, the number of cases of asbestos-related mesothelioma is increasing despite the fact that asbestos production ended in 1987 and the importation of asbestos products was completely banned in 2003. www.australiandoctor.com.au Recent decades have seen a marked increase in awareness about the adverse health effects of hazardous exposures in the workplace. This has resulted in tighter workplace regulations and industrial legislation to safeguard the health of workers. Each state government now has a WorkCover Authority focused on workplace safety. Among other things, these authorities assist with compensation of workers with occupational lung diseases. Occupational lung diseases can be categorised into groups according to: • Anatomical location (table 1). cont’d next page Dr Michael Hibbert senior respiratory and sleep specialist, department of respiratory and sleep medicine, Royal North Shore Hospital, St Leonards; and lecturer, Northern Clinical School , University of Sydney, NSW. Copyright © 2013 Australian Doctor All rights reserved. No part of this publication may be reproduced, distributed, or transmitted in any form or by any means without the prior written permission of the publisher. For permission requests, email: [email protected] 8 March 2013 | Australian Doctor | 23 How To TREAT Occupational lung diseases from previous page • Inhaled substances (table 2). • Reaction type. • Pathophysiological responses. Occupational lung disease needs to be considered in any current or retired worker, particularly when the worker is involved in an industry with exposure to a known hazardous material. It is important to be aware of the latency between exposure and onset of symptoms, especially in the case of asbestos and silica exposure, where there may be a delay of decades before the onset of symptoms. Similarly in occupational asthma, the onset of symptoms may be delayed for months to years after the initial exposure to the allergen. On the other hand, we should not assume the origins of respiratory symptoms are caused by an occupational exposure without a clear causal relationship. Early cessation of exposure to a toxic agent is of paramount importance. Because respiratory symptoms caused by toxic exposures are nonspecific, recognising their potential relationship to a toxic agent or agents is essential to proper diagnosis. Continued exposure may result in irreversible functional decline and even fatal respiratory disease. Knowledge about and familiarity with these diseases is critically important for the primary care physician, who is often the first healthcare provider to see the affected individuals. Table 2: Agents responsible for occupational lung diseases Agent Industry/occupations Lung condition Asbestos Mining and milling, building and construction, transport equipment manufacturing (shipbuilding, railway locomotive building and maintenance), asbestos product manufacture, power generation, carpenters and joiners, metal fitters, boilermakers Pleural plaques, pleural thickening, pulmonary fibrosis (asbestosis), mesothelioma Beryllium Aerospace, nuclear power, computer, automotive electronics Pulmonary fibrosis (berylliosis), emphysema, lung cancer Barium Petroleum industry Pulmonary fibrosis Coal Coal mining Pulmonary fibrosis Centrilobular emphysema Cadmium Electronics, metal plating and batteries Emphysema, lung cancer Cotton dust Cotton, flax and hemp workers Bronchitis, byssinosis, hypersensitivity pneumonitis Isocyanates Spray painting Asthma, hypersensitivity pneumonitis Irritant gases (ammonia, sulphur dioxide, chlorine) Chemical industry, agriculture, fertilisers Bronchitis, asthma Ionising radiation Radiology, nuclear industry Pneumonitis, pulmonary fibrosis, lung cancer Mouldy hay (thermophilic actinomycetes) Agriculture (farmers) Bronchitis, hypersensitivity pneumonitis Silica Sandblasters, miners, tunnelers, millers, potters, glassmakers, foundry and quarry workers Simple silicosis, silicoproteinosis, progressive massive fibrosis, COPD Talc Paint, ceramics, leather, paper Pulmonary fibrosis Wood dust Milling, construction Hypersensitivity pneumonitis, asthma Asbestos-related lung conditions ASBESTOS is a naturally occurring mineral used since ancient times for its strength and fire-resistant properties. Due to these properties, asbestos has been widely used in building materials, fire resistant products and insulation (lagging). The most common types of asbestos fibres are serpentine fibres (chrysotile or ‘white asbestos’) and amphiboles (amosite ‘brown asbestos’ and crocidolite ‘blue asbestos’). Asbestos exposure can result in a number of lung conditions particularly in the occupational setting (see the box below). Exposure to amphibole fibres (crocidolite) confers a greater risk of developing lung disease than the serpentine fibres of chrysotile. This relates to the persistence of amphiboles in the lung for many years after the exposure has stopped, in comparison with chrysotile fibres, which generally disappear within 10 years. Asbestos was mined and processed in Australia for more than 100 years. Until 2003, there was extensive local use and subsequent exposure in many industries. The occupations with high incidence of asbestos exposure are summarised in table 2. As in other industrialised countries, the ill-effects from past exposure are expected to peak later this decade in Australia, due to the long lag time between exposure and disease presentation, particularly in the case of mesothelioma. Exposure to asbestos is quantified in terms of the concentration of inhaled fibres (fibres/mL) with the highest exposure seen in people who worked in asbestos mining (up to 100 f/mL) and background community exposure generally measured at less than 0.01f/mL. The recommended exposure standards for asbestos in air in Australia are 0.1f/mL. Cumulative exposure is expressed in fibre/mL/years, similar to the packyear measurement for smoking. Asbestiform fibres also occur naturally in areas where other minerals, 24 | Australian Doctor | 8 March 2013 Figure 1: Pleural plaques as seen on chest X-ray. Pleural plaques Figure 2: Rounded atelectasis. Benign pleural plaques All radiology images courtesy of Dr Greg Briggs and Dr Anne Miller. Lung conditions related to asbestos exposure • Pleural plaques • Benign pleural effusion • Rounded atelectasis • Diffuse pleural thickening • Asbestosis • Mesothelioma • Lung cancer such as gold and iron ore, have been exploited, with a consequent risk of significant lung disease to miners. Currently, the main sources of exposure to asbestos fibres are old buildings undergoing renovation or demolition where building maintenance and demolition workers are employed. Home owners renovating their own homes are also at risk of exposure to asbestos fibres. Plaques are deposits of hyalinised collagen fibres on the parietal pleura. They are usually found on the parietal pleura adjacent to the 6th-9th ribs and along the diaphragm. Plaques are rarely seen in the lung apices or costophrenic angles. It usually takes about 20 years after exposure to asbestos for plaques to be evident, and they are often calcified. Up to half of those exposed to asbestos develop plaques. They rarely occur bilaterally without asbestos exposure (figure 1). Benign pleural plaques are merely the markers of asbestos exposure and in isolation do not cause any symptoms. They have no effect on lung volumes and do not impair exercise tolerance or gas exchange. Regular follow-up of pleural plaques with imaging is not required due to their lack of disease potential and such follow-up has not been shown to impact on the survival from mesothelioma or lung cancer. Benign pleural disease Benign asbestos-related pleural effusion (BAPE) Exposure to asbestos can cause benign pleural plaques, benign pleural effusions, diffuse pleural thickening or rounded atelectasis in the sub-pleural lung parenchyma. Benign asbestos-related pleural effusion (BAPE) is usually an exudative unilateral effusion with occasionally eosinophilic predominance on cell counts. The interval between www.australiandoctor.com.au the exposure and the presentation of effusion may vary from 5-30 years and early onset is correlated with higher exposures. It usually resolves spontaneously or may be followed by diffuse pleural thickening (see below). Rounded atelectasis Pleural adhesions caused by asbestos-related pleural inflammation result in atelectasis of a part of the sub-pleural lung parenchyma and appear as a rounded lung mass on imaging (figure 2). In many instances when they are large or not classical in radiological appearance, biopsy is required to exclude malignancy. Diffuse pleural thickening This generally begins as fibrosis of the visceral pleura with secondary thickening of the parietal pleura. Both visceral and parietal pleura become inseparable, leading to obliteration of the costophrenic sulci (figures 3 and 4). Although commonly a precursor to diffuse plural thickening, pleural effusion is not a prerequisite for diffuse thickening. Diffuse plural thickening may result in dyspnoea as a result of a reduction in lung volumes and diffusion capacity. Asbestosis Diffuse interstitial pulmonary fibrosis caused by asbestos exposure is called asbestosis. It is indistinguishable from idiopathic pulmonary fibrosis except for the presence of other radiological features of asbestos exposure such as calcified pleural plaques or identification of asbestos fibres or ferruginous bodies (asbestos fibres coated by iron) in the lung tissue. Although the term ‘asbestosis’ is often used to describe any asbestos-related disease affecting the lung and the pleura, it should be confined to pulmonary fibrosis caused by asbestos exposure. The development of asbestosis follows high-level asbestos exposure usually seen only in those with occupational exposure. Many patients who develop asbestosis are asymptomatic for at least 20-30 years after the initial exposure and a high level of exposure results in a shorter latency period. Patients present with an insidious onset of exertional dyspnoea. Productive cough and wheeze are rare and, if present, are usually caused by concomitant smoking-related lung disease. Bilateral fine-end inspiratory crackles and clubbing are seen in about 40-60% cases. Pulmonary function testing demonstrates restricted lung volumes with reduced gas transfer. Laboratory tests such as sputum and basic blood tests are unhelpful. High-resolution CT scanning is much more sensitive than X-ray for assessment, with interstitial changes seen in the lower zones early in the course and progression to honeycombing and upper lobe involvement as the disease advances. Concurrent smoking accelerates the progression of fibrosis. Asbestosis is in general a slowly progressive disease but occasionally follows a more accelerated course, leading to respiratory failure. Malignant mesothelioma Malignant mesothelioma is an insidious, aggressive and fatal cancer of the parietal pleura with a median survival of 12 months from diagnosis. Occasionally it may involve the mesothelial surfaces of the peritoneal cavity, pericardium and tunica vaginalis. Eighty-five per cent of cases are caused by asbestos exposure in an occupational setting. It may also occur with very lowlevel asbestos exposure occasioned by activities such as washing the clothes of someone working in an asbestos-related work environment. The lifetime risk of mesothelioma in a population exposed to asbestos is in the range of 5-10%. Crocidolite fibre exposure causes the greatest risk for the development of malignant mesothelioma. The latency between first exposure and the development of malignant mesothelioma varies from 15-60 years, with patients most commonly presenting in their 50s, 60s or 70s. The most frequent presenting symptoms of pleural mesothelioma are dyspnoea, often related to a pleural effusion, and non-pleuritic chest pain. Occasionally it may present as an asymptomatic unilateral pleural effusion on routine imaging. The initial chest X-ray findings often show the presence of a pleural effusion or pleural thickening. Figure 3: Chest X-ray of the thorax demonstrating asbestos-related diffuse pleural thickening. Note the overall reduction in right lung volume. Figure 5: Imaging findings in pleural mesothelioma. A: Chest X-ray demonstrating the four classic findings: pleural thickening, pleural effusion, decreased thoracic volume, and no shift of the mediastinum to the affected side. B and C: CT scans demonstrating pleural thickening, loculated pleural effusion, and pleural nodularity. Pleural thickening othelioma. Soluble mesothelinThe most common CT findings Figure 4: CT thorax of the same patient, demonstrating encasement of the right hemithorax by the diffuse pleural thickening with overall reduction in lung volume. Pleural thickening A are pleural thickening (92%), pleural effusion (74%) (figure 5) and contraction of a hemithorax. Only one-fifth of patients will have radiological evidence of asbestosis. It is also rare for there to be bilateral involvement with malignancy. A PET scan may help to differentiate malignant mesothelioma from diffuse pleural thickening. A definitive histological diagnosis is essential, given the medicolegal consequences of the diagnosis and prognostic implications of particular histological subtypes. Epithelioid and mixed-type malignant mesothelioma denote a better prognosis than sarcomatoid mesothelioma. Closed pleural biopsy or thoracocentesis may produce false-negative results. Surgical intervention in the form of open thoracotomy or video-assisted thoracoscopic surgery has a higher diagnostic yield and is recommended for the tissue sampling. After the pleural biopsy via thoracoscopy or thoracotomy, the surgeons may, if indicated, perform a pleurodesis procedure by mechanically irritating the parietal pleura to cause adhesion of parietal and visceral pleura to prevent any recurrent pleural effusions Although no clear diagnostic role has been established for serum tumour markers, both mesothelin and osteopontin have been used in the research setting to aid in the non-invasive diagnosis of mesothelioma. Mesothelin is a glycoprotein that is expressed on the surface of the normal mesothelial cells and is over-expressed in malignant mes- related peptides are measured in serum and pleural fluid and their sensitivity in detecting malignancy varies from 16-68% and is limited to epithelioid types. Osteopontin is overexpressed in mesothelioma but has a lower diagnostic yield than mesothelin. Currently, there is no serum, pleural fluid or urine marker that can be used in isolation to diagnose or exclude mesothelioma. Asbestos-related lung cancer Lung cancer can occur as a result of asbestos exposure even in the absence of pulmonary fibrosis. The risk is related to the degree of exposure and the presence of asbestosis. However, it is worth noting that not everyone who develops lung cancer in the asbestos exposure setting has asbestosis. While smoking remains the most important causative agent for lung cancer, the combined effect of asbestos and smoking appears to be more than additive and approaches a multiplicative effect. The relative risk of cancer is increased by up to 60-fold in smokers with asbestos exposure. There is a dose–response relationship between asbestos exposure and risk of lung cancer. The quantitative risk of lung cancer varies according to fibre type and cumulative exposure. Crocidolite fibres are three times more likely than chrysolite fibres to cause lung cancer with the same level of exposure. Estimates for excess deaths from lung cancer (ie, compared with the background rate of deaths from lung cancer) at very heavy exposures of 100 f/mL years are of the order www.australiandoctor.com.au B Pleural effusions Pleural thickening with nodularity C of 5-100 per 100,000 for chrysotile and 150-350 for crocidolite. Overall, it appears that asbestos-related lung cancer is under-diagnosed and under-compensated mainly because of doctors attributing lung cancer to smoking without considering the contribution of asbestos in patients, most of whom are heavy smokers. cont’d page 26 8 March 2013 | Australian Doctor | 25 How To TREAT Occupational lung diseases Other occupational lung diseases Silicosis SILICOSIS is a fibrotic lung disease caused by inhalation of free crystalline silica. Given that silica is the most abundant mineral in the world, occupational exposure to respirable crystalline silica dust particles occurs in a vast number of industries including mining, quarrying, stone cutting, polishing and sandblasting. Phagocytosis of crystalline silica in the lung triggers an inflammatory cascade with subsequent fibrosis. Impairment of lung function increases with disease progression, even after the patient is no longer being exposed. The cumulative dose of silica is the most important factor that predicts the development of silicosis. On X-ray in simple silicosis, there are small round opacities, often symmetrically distributed with upper-zone predominance and associated calcification of lymph nodes. Lung function abnormalities are uncommon in early disease. In progressive massive fibrosis (figure 6), opacities larger than 1cm develop due to coalescing of small nodules with development of fibrosis and worsening lung function. Mycobacterial diseases, COPD, Kaplan’s syndrome (silica nodules with fibrosis in rheumatoid arthritis patients) and lung cancer are associated with silica dust exposure. Meta-analyses of cancer risk in silicosis sufferers show a significant increase, but the effect of silica exposure on lung cancer is weak and variable in workers who do not have silicosis. Silicosis is becoming less common in industrialised nations through aggressive measures to control airborne dust in the workplace, but is still a major problem in many developing nations. Coal workers’ pneumoconiosis An occupational lung disease caused by exposure to coal dust, coal workers’ pneumoconiosis is also known as ‘black lung disease’ with deposition of coal in the lung parenchyma. Simple coal workers’ pneumoconiosis is characterised by the presence of upper lobe nodular opacities that can develop into progressive massive fibrosis with restrictive impairment of lung func- Figure 6: Progressive massive fibrosis in silicosis. High-resolution CT showing bilateral upper lobe predominant large irregular rounded opacities, interlobular septal thickening with fibrous parenchymal bands and ground glass pattern. It also shows mediastinal and hilar lymphadenopathy with associated ‘eggshell’ calcification. tion. The onset of disease is related to the length and severity of exposure. Silica contamination increases the pneumoconiosis risk and consequently in some coalminers, pneumoconiosis may represent a mixed picture of coal pneumoconiosis and silicosis. Coal workers’ pneumoconiosis can also result in airway obstruction with focal emphysema due to small airway inflammation. The prevalence and mortality rates from coal workers’ pneumoconiosis are declining in most industrialised countries including Australia as a result of tightened industrial regulations. Hypersensitivity pneumonitis Hypersensitivity pneumonitis (extrinsic allergic alveolitis) is a granulomatous disease of the lungs caused by an immunological response to chronic inhalation of organic dusts or chemicals, with more than 300 aetiological agents reported to date. Only a small proportion of those exposed develop clinically significant hypersensitivity pneumonitis, although it may progress to disabling or even fatal end-stage lung disease. While oral corticosteroids can improve the symptoms and radiological appearance in the short term, the definitive treatment is early recognition and control of exposure. Farmer’s lung is one of the most common forms of hypersensitivity pneumonitis. Cattle farming, bird and poultry handling (bird fancier’s lung), grain and flour processing and lumber milling are some of the occupations that are associated with a risk of developing hypersensitivity pneumonitis. While many causative agents have been recognised in occupational dusts, most current new cases arise from residential exposure to pet birds (pigeons and parakeets), contaminated humidifiers, and indoor moulds. Occupational lung cancer At least 12 substances found in the workplace are classified as human lung carcinogens. These include asbestos, radon, diesel exhaust fumes and certain metals such as arsenic, cadmium, chromium, beryllium and nickel (table 2, page 24). Occupational exposure is estimated to account for about 5% of lung cancer in Australia, with most of them being caused by asbestos. Occupations and industries that tend to be associated with an increased risk of lung cancer include mining and quarrying, asbestos production, metal industries, shipbuilding, railroad equipment manufacturing, gas production and Assessment History A THOROUGH occupational and environmental history is the key in the assessment of potential occupational lung disease. The occupational history should be documented in detail in chronological order for every job the patient has ever held, irrespective of duration. The history for each job should include • Job title. • Tasks undertaken/job processes. • Exposures — type (chemical, gas, fumes, dust) and level (mild, moderate, high), duration of exposure (per day, per year). • Availability and use of respiratory protection and ventilation methods used. Any environmental and domestic exposures associated with demolition or renovation should also be inquired about along with the smoking history. A thorough history is not only essential for an accurate diagnosis but also plays an important role in the possible subsequent litigation process. Occupational hygienists can help with accurate assessment of the degree 26 | Australian Doctor | 8 March 2013 of exposure (see Online resources, page 28). A history of progressive shortness of breath, chronic cough and other constitutional symptoms usually accompanies the clinical presentation of occupational lung disease. The transient presence of symptoms in relation to the work environment is typical in occupational asthma. Examination The physical signs related to occupational disease are minimal and generally unrevealing about specific causes. The clinical findings include clubbing, inspiratory crackles and wheeze at times. Occasionally pleural effusion is detected clinically. A comprehensive general physical examination, particularly involving the cardiac system, remains important, looking for evidence of advanced signs such as pulmonary hypertension and related cor pulmonale as well as evidence of alternative differential diagnoses and assessment of impairment (see Investigations, page 28). cont’d page 28 www.australiandoctor.com.au some areas of construction. Occupational asthma Occupational asthma is defined as asthma caused by exposure to agents encountered in the working environment in those without pre-existing asthma. In developed countries, occupational asthma is the leading form of occupational lung disease, having supplanted lung disease related to dust. An estimated 15% of newly diagnosed cases of asthma in working adults are the consequence of occupational exposures. Occupational asthma can occur as a new onset of asthma caused by repeated low-level sensitising exposure (asthma with latency, sensitiser-induced asthma) or asthma that results from a single heavy exposure to a potent respiratory irritant such as chlorine or ammonia (asthma without latency, irritant asthma, or the reactive airways dysfunction syndrome). Spray painters (diisocyanatebased paints), bakers (flour), lumber industry workers (red cedar dust) and cleaners work in some of the highest risk occupations for developing occupational asthma. Most occupational asthma is associated with a latency period of hours to months. Occupational asthma should be considered in every case of adult-onset asthma. Occupational asthma symptoms are identical to patients with asthma without an occupational exposure. Another type of work-related asthma is aggravation of pre-existing asthma by the work environment (work-aggravated asthma). In this situation, an individual with pre-existing asthma who is exposed to factors in the workplace such as non-specific gases or fumes, smoke or cold dry air may have an asthmatic attack precipitated by these factors. The detailed work history should include all types of prior occupations and the specific duties that were performed, the relationship between the symptoms and the workplace and any improvement in symptoms when away from work, particularly for extended periods of time. The confirmation of occupational asthma should begin with spirometry and peak expiratory flow recordings to assess airflow obstruction, its reversibility and variability. Reversible airflow obstruction is a key feature in establishing the diagnosis of asthma, but many asthmatic patients may have normal or near-normal pulmonary function, especially during non-exacerbation periods or due to treatment. In this instance, a methacholine challenge test or comparable measure of nonspecific airway hyper-responsiveness (such as a Mannitol challenge test) during a period of work exposure may help to establish the diagnosis of asthma. The relationship of exposure to work is usually confirmed by serial peak flow measurements performed at least four times a day for a period of at least three weeks at work and three weeks away from work. Other tests that can be performed in the assessment of sensitiser-induced occupational asthma include allergen skin-prick testing and serum-specific IgE testing. Specific challenge testing with the suspected agent is not usually performed in Australia but remains the gold standard of diagnosis. The patients should not be asked to leave work or change their work practices until assessed by a specialist respiratory physician and the diagnosis of occupational asthma is confirmed, as the outcome has important medical, public health, legal and financial implications. Workers with occupational asthma should avoid all future exposure to the sensitising agent. This usually requires a change of job, ideally within the same organisation to minimise hardship to the worker. While occupational asthma can resolve after these measures in about 50% of cases, this is more likely with earlier diagnosis and removal from exposure. Workers with irritant-induced asthma caused by a single heavy exposure, who are not sensitised, can continue working with the agent at low-level exposure. Treatment of occupational asthma is similar to that for usual asthma with inhaled steroids and bronchodilators but significant improvement can result with mere avoidance of the respiratory irritant. Investigations Serum TAKING an FBC and biochemistry to exclude non-respiratory causes of presenting symptoms should form an early part of the investigative process. Allergen-specific IgE can be useful in some forms of occupational asthma (eg, animal house workers). Precipitants to avian proteins, fungus and thermophilic actinomycetes may be present in patients exposed to organic dusts (eg, mouldy hay exposure leading to hypersensitivity pneumonitis) and should be requested in the pathology. The diagnostic value of soluble mesothelin-related peptide is debatable. Currently it is more useful as a marker for monitoring disease progression in mesothelioma at specialised clinical centres. Radiology Chest X-ray is a good screening test, but provides insufficient detail for Online resources complete assessment. High-resolution CT scan of the chest provides excellent identification of fibrosis, nodules and ground glass opacities associated with various occupational lung diseases. Images taken in the prone position are important to exclude innocent dependent changes at the lung bases, which may masquerade as pulmonary fibrosis. A CT scan of the chest is also important in identifying pleural plaques — one of the markers of asbestos exposure, even when they are not calcified. Pulmonary function tests Spirometry is useful as a screening test, particularly for the diagnosis of early airway obstruction when FEV1/ forced vital capacity (FVC) is less than 70%. Serial measurements may be a simple method for monitoring progression in fibrotic lung disease generally with normal or increased FEV1/FVC ratio. Reduced lung volume measurements, both residual volume and total lung capacity, in association with a lowered carbon monoxide diffusing capacity (DLCO) strongly suggest a restrictive defect such as the pulmonary fibrosis seen in asbestosis. Serial peak flow measurements provide evidence for variability in airflow measurements as seen in occupational asthma, particularly when performed at home and at work. Bronchial provocation testing with mannitol or methacholine may be helpful in diagnosing occupational asthma. It is important that this is performed while the patient is exposed to the irritant. Other tests TB screening with Mantoux skin testing in patients with silicosis is recommended as there is strong evidence for an association between silicosis and mycobacterial infection. Cardiopulmonary exercise testing provides an objective measure of the overall degree of functional impairment. An assessment of cardiac function including pulmonary pressures with an echocardiogram may be useful in advanced interstitial lung diseases (asbestosis or silicosis). Bronchoscopy with bronchioalveloar lavage is rarely useful in occupational lung diseases other than in situations where an alternative diagnosis such as infection needs to be excluded. Histopathological confirmation of the clinical diagnosis may occasionally be necessary in some cases of occupational interstitial lung disease. In general, fine-needle aspiration biopsy or transbronchial lung biopsy is insufficient for definitive diagnosis and a larger tissue sample, which can be achieved thoracoscopically, is required. Management THERE is no specific management currently available for most of the occupational lung diseases. Steroid therapy for occupational asthma and hypersensitivity pneumonitis; and surgical intervention in early occupational lung cancer are some of the specific therapies available. Supportive care with the emphasis on primary and secondary prevention is the current treatment goal. Informing the patient of the likely work-related nature of the illness and the options for compensation will form part of the initial management with formal assessment of functional impairment. For current workers, further avoidance of the exposure is paramount. Patients with benign asbestosrelated conditions such as pleural plaques can be reassured that no regular follow-up required. The management of patients with asbestosis and other pneumoco- nioses should focus on secondary preventive measures including: • Smoking cessation. • Withdrawal from further exposure. • Immunisation with pneumococcal and influenza vaccines. • Optimal management of concurrent respiratory and other diseases. • Supplemental oxygen when resting hypoxaemia or exerciseinduced oxygen desaturations occurs. Regular monitoring with respiratory function tests and imaging every 2-3 years or earlier is recommended with development of a patient-specific management plan for symptomatic patients. Management of malignant mesothelioma is controversial, with no standard approach currently available. The treatment may vary from symptom control with pleurodesis for recurrent malignant pleural effusion and pain relief to radical surgery or combined approaches. No randomised control trials have demonstrated a survival benefit with surgical resection. A recent pilot study in the UK (the MARS trial), showed no survival benefits but increased morbidity with surgery compared with non-surgical approach.1 A palliative approach with drainage of pleural effusions and systemic chemotherapy with a cisplatin–pemetrexate combination could be considered. Molecularly targeted agents have been trialled in mesothelioma although additional clinical trials are required to establish whether these approaches will have a role in patient management. Management of lung cancer and asthma related to occupational exposure is identical to the management in general population. Medicolegal aspects of occupational lung disease The medicolegal aspects of occupational lung diseases are complex. Workers compensation is available through the state-based WorkCover authorities, as in all occupational diseases. Diagnosis is usually based on physician assessment, and income support and retraining are usually available to patients. NSW has a specific scheme for asbestos- and silica-related diseases administered by the Workers’ Compensation Dust Diseases Board. Common law claims can also be pursued, especially with asbestos-related conditions, and require referral to an appropriate legal representative. The fact that an employer may no longer exist does not preclude compensation, as insurers can usually be located. Author’s case studies Case study 1: Mesothelioma Mr MH was an 89-year-old retired man, living with his wife. He presented with a three-month history of increasing shortness of breath, rightsided pleuritic chest pain and a 10kg weight loss. A CT chest showed a small right-sided pleural effusion with pleural plaques. He was a lifelong non-smoker. Mr MH had had a variety of occupations in the past but spent over 30 years working in a power station and had at least moderate asbestos exposure. Given the clinical symptoms and the latency of asbestos exposure, his presentation was very suspicious for a malignant mesothelioma. Pleural aspiration revealed an exudate with no evidence of infection or malignant cells. While other diagnoses such as primary lung cancer, metastatic malignancy, infective or an inflammatory effusion were possibilities, the most likely diagnosis remained mesothelioma due to the clinical presentation and radiology. The possibility of a tho- 28 | Australian Doctor | 8 March 2013 racoscopic procedure (eg, videoassisted thoracoscopic surgery) with a pleural biopsy to obtain tissue for definitive diagnosis and to perform a pleurodesis to prevent recurrent pleural effusions was discussed at length with the patient. Given the small amount of the fluid and the marked frailty of the patient, it was decided that he should be managed conservatively, with symptom control, with a presumptive diagnosis of malignant mesothelioma. He was started on regular paracetamol and an opiate for pain relief and was also started on a small dose of prednisolone to improve his appetite and wellbeing. He was referred to community palliative care services for pain management and regular follow-up. Mr MH’s family also sought legal representation with the view to seeking compensation. He continued to deteriorate with weight loss and generalised weakness accompanied by increasing right-sided chest pain and worsening short of breath. A few months later, he was admitted to hospital because of significant clinical deterioration. He was managed palliatively and died five days later. A post-mortem, requested by his family and performed for the purposes of compensation, confirmed the diagnosis of mesothelioma. Discussion points • A unilateral pleural effusion with pleuritic pain and constitutional symptoms in a patient with previous asbestos exposure is highly suspicious of mesothelioma, even with negative cytology. • Since surgical and other multimodality therapy in mesothelioma has no clear survival advantage with an overall median survival of only 12 months, the pros and cons of aggressive therapy vs comfort care should be discussed with the patient and next of kin at diagnosis. • Adequate analgesia with good symptom control, early palliative care referral and a claim for compensation are some of the key facwww.australiandoctor.com.au US National Institute of Occupational Safety and Health Occupational Respiratory Disease and Surveillance (information on various occupational lung diseases, its spread and its impact) www.cdc.gov/niosh/topics/ surveillance/ords/ Workers’ Compensation Dust Diseases Board of NSW Provides a system of no-fault compensation to people (and their dependants) who have developed a dust disease from occupational exposure to dust as a worker in NSW www.ddb.nsw.gov.au Asbestos Diseases Research Institute Aims to improve the prevention, the diagnosis and treatment of asbestos-related diseases www.adri.org.au Asbestos Diseases Society of SA Provides counselling, support and information to asbestos disease victims in SA www.adssa-inc.com.au Australian Mesothelioma Registry Monitors all new cases of mesothelioma diagnosed from 1 July 2010 in Australia www.mesothelioma-australia.com Asbestos Awareness Describes why asbestos is dangerous, where it can be found in the home, how to remove it safely, how to deal with it and how to dispose of it www.asbestosawareness.com.au Safework Australia Provides national codes of practice and guidance notes and reports by the Australian Safety and Compensation Council on mesothelioma www.safeworkaustralia.gov.au Australian Institute of Occupational Hygienists Information about occupational hygiene and the profession of occupational hygienist www.aioh.org.au tors in mesothelioma management. Case study 2: Occupational asthma A 30-year-old male with no past history of asthma began working several years ago as a glazier in a firm manufacturing windows and doors. His work took place in a single shared open-plan factory. Wood machining, wood joinery and glazing were carried out in adjoining areas. His job involved cutting glass and placing glass in windows and doors. Almost all the wood used in the factory was Western red cedar. Within 12 months of starting work he developed rhinitis and dermatitis. Eight years later, he noticed the gradual onset of cough and chest tightness. His GP diagnosed asthma and started him on beclomethasone and salbutamol. He left his job as he felt his asthma was work-related and worked as a courier for a few years. During this time, he was able to stop all asthma medications owing to a lack of asthma symptoms. cont’d page 30 Reference 1. Treasure T, et al. Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: clinical outcomes of the Mesothelioma and Radical Surgery (MARS) randomised feasibility study. Lancet Oncology 2011; 12:763-72. Further reading Available on request from [email protected] How To TREAT Occupational lung diseases Figure 7: Serial peak flow readings of 30-year-old male working in a window and door factory. SERIAL PEFR 700.0 Maximum Mean Minimum Working 650.0 600.0 550.0 PEFR from page 28 Some years later, he recommenced work as a glazier in the same factory as before. Within one month it became necessary for him to start taking his asthma medications again because of symptom recurrence. His asthma has persisted since and has become worse in the past year. He has had two exacerbations of asthma in the past 12 months requiring courses of prednisolone. There have been no spills or accidents at work to suggest irritant asthma. He is an exsmoker with five pack-year history. His examination was unremarkable and his baseline spirometry was normal. He had evidence of nonspecific bronchial hyper-responsiveness with a positive methacholine challenge. He monitored his serial peak flows and the results are shown in figure 7. There was a significant deterioration in his peak flows at the start of the working week, with an improvement on weekends. A diagnosis of occupational asthma due to Western red cedar was made. He was moved to another 500.0 450.0 400.0 350.0 08 08 08 08 08 08 08 08 08 /20 /20 /20 /20 /20 /20 /20 /20 /20 /01 /01 /01 /02 /01 /02 /02 /03 /02 4 7 1 1 8 4 8 1 5 1 0 2 1 2 1 2 Date part of the factory with no exposure to Western red cedar and now has no asthma symptoms, is on no medications and has a normal methacholine challenge. Discussion points • New asthma in a working person requires documentation of a careful occupational history. • Occupational exposure to a known How to Treat Quiz Occupational lung diseases — 8 March 2013 1. Which THREE statements are correct regarding occupational lung disease? a) It is important to consider occupational lung disease in any current or retired worker with respiratory symptoms b) The upper airways are never affected by occupational exposure to inhaled irritants c) Awareness of the latency between exposure and onset of symptoms is extremely important in consideration of occupational lung disease d) A clear causal relationship needs to be established before attributing the cause of a patient’s respiratory symptoms to occupational exposure 2. Which TWO statements are correct regarding asbestos fibres? a) Asbestos is a man-made fibre that has been in use only since the early 1950s b) Asbestos production ended in Australia in 1987 and the importation of asbestos products was completely banned in 2003 c) Serpentine fibres are known as chrysotile or ‘white asbestos’, while amosite (‘brown asbestos’) and crocidolite (‘blue asbestos’), are both amphiboles d) Blue asbestos, or crocidolite, is a benign form of asbestos fibre, in contrast to white asbestos, or chrysotile 3. Which THREE statements regarding asbestos exposure are correct? a) Occupational exposure to asbestos is limited to those involved in asbestos product manufacture b) Exposure to asbestos is quantified in terms of the concentration of inhaled fibres (fibres/mL). Cumulative exposure is expressed in fibre/mL/ years, similar to the pack-year measurement for smoking c) Asbestiform fibres also occur naturally in cause of occupational asthma, such as Western red cedar, increases the likelihood of the diagnosis of occupational asthma. • Work-related symptoms including rhinitis and dermatitis followed by asthma symptoms are suggestive of occupational sensitisation. It may take months to several years before the onset of asthma symptoms. •E vidence of a relationship between lung function and attendance at work, with documentation of peak flow measurements, confirms the diagnosis of occupational asthma and should be performed before advising a worker to stop exposure. •E vidence of reversible airway obstruction on spirometry is very specific for a diagnosis of occupational asthma while nonspecific bronchial hyper-responsiveness may be helpful when spirometry is normal with high clinical suspicion. •F urther exposure to the sensitising agent needs to be avoided. Summary Occupation-related lung diseases are common despite workplace regulations and increased awareness A thorough occupational history is crucial in identifying any workrelated lung conditions Finding a clear temporal relationship between symptoms and exposure is useful, but be aware that current exposures do not always lead to immediate symptoms An occupational agent is a common culprit in adult-onset asthma and is under-diagnosed as a result of the failure to associate symptoms and work. Early referral to a respiratory physician is recommended if there are ongoing respiratory symptoms in a patient with occupational exposure. Avoidance of exposure to the causative agent is the main management strategy to reduce further lung impairment. Instructions Complete this quiz online and fill in the GP evaluation form to earn 2 CPD or PDP points. We no longer accept quizzes by post or fax. The mark required to obtain points is 80%. Please note that some questions have more than one correct answer. GO ONLINE TO COMPLETE THE QUIZ www.australiandoctor.com.au/education/how-to-treat areas where other minerals, such as gold and iron ore, have been exploited, with a consequent risk of significant lung disease to miners d) Currently, the main sources of exposure to asbestos fibres are old buildings undergoing renovation or demolition 4. Which THREE statements regarding benign pleural disease are correct? a) Benign plural plaques are deposits of hyalinised collagen fibres on the parietal pleura b) Benign pleural plaques require regular followup with imaging c) Pleural adhesions due to asbestos-related pleural inflammation appear as a rounded lung mass on imaging and often require a biopsy to exclude malignancy d) Diffuse pleural thickening generally begins as fibrosis of the visceral pleura with secondary thickening of the parietal pleura 5. Which TWO statements regarding asbestosis are correct? a) Asbestosis is the correct term to describe all asbestos-related disease affecting the lung and pleura b) Many patients who develop asbestosis are asymptomatic for at least 20-30 years after the initial exposure c) Productive cough and wheeze are rare in patients suffering from asbestosis d) Chest X-ray is the gold standard for detection of asbestosis 6. Which TWO statements are correct regarding mesothelioma? a) Malignant mesothelioma has a median survival of three years from diagnosis b) Mesothelioma may occur with very-low- level asbestos exposure occasioned by activities such as washing the clothes of someone working in an asbestos-related work environment c) The most common CT findings are pleural thickening (92%), pleural effusion (74%) and contraction of a hemithorax d) Diagnosis of mesothelioma can be definitively established using the serum tumour markers mesothelin and osteopontin 7. Which THREE statements regarding silicosis and hypersensitivity pneumonitis are correct? a) The mechanism causing silicosis from inhalation of free crystalline silica is phagocytosis of the crystalline silica in the lung, which triggers an inflammatory cascade, with subsequent fibrosis b) Short-term occupational exposure to silica can cause silicosis c) Hypersensitivity pneumonitis (extrinsic allergic alveoli) is a granulomatous disease of the lungs caused by an immunological response to chronic inhalation of organic dusts or chemicals d) Cattle farming, bird and poultry handling (bird fancier’s lung), grain and flour processing and lumber milling are some of the occupations that are associated with a risk of developing hypersensitivity pneumonitis 8. Which TWO statements are correct regarding occupational asthma? a) Occupational asthma is defined as asthma caused by exposure to agents encountered in the working environment in workers without pre-existing asthma b) An estimated 2% of newly diagnosed cases of asthma in working adults are the consequence of occupational exposures c) The relationship of exposure at work is usually confirmed by serial peak flow measurements performed at least four times a day for a period of at least three weeks at work and three weeks away from work d) Frequent doses of oral corticosteroids is the standard treatment for occupational asthma 9. Which TWO statements regarding assessment of patients with occupational lung disease are correct? a) Identification of the multitude of clinical signs that develop as a result of occupational lung disease is essential to diagnosis b) Industrial hygienists can help with accurate assessment of the degree of exposure c) Soluble mesothelin-related peptide is currently useful as a marker for monitoring disease progression in mesothelioma at specialised clinical centres d) Bronchoscopy with bronchioalveloar lavage is an important investigation in the diagnosis of occupational lung disease 10. Which TWO statements regarding treatment and compensation of occupational lung disease are correct? a) Secondary preventive measures for patients with asbestosis and pneumoconiosis include smoking cessation, withdrawal from exposure, and immunisation with pneumococcal and influenza vaccines b) Surgical treatment of mesothelioma has demonstrated survival benefits c) NSW has a specific compensation scheme for asbestos- and silica-related diseases administered by the Workers’ Compensation Dust Diseases Board d) Compensation for occupational lung disease is impossible to obtain if the employer no longer exists CPD QUIZ UPDATE The RACGP requires that a brief GP evaluation form be completed with every quiz to obtain category 2 CPD or PDP points for the 2011-13 triennium. You can complete this online along with the quiz at www.australiandoctor.com.au. Because this is a requirement, we are no longer able to accept the quiz by post or fax. However, we have included the quiz questions here for those who like to prepare the answers before completing the quiz online. how to treat Editor: Dr Barbara Tink Email: [email protected] Next week Non-alcoholic fatty liver disease is emerging as the most common cause of liver disease worldwide, despite its being hard to diagnose and having only an estimated true incidence. It is physiologically linked to insulin resistance and is the hepatic manifestation of the metabolic syndrome. The next How to Treat aims to build awareness of this condition, focusing on its pathogenesis, diagnosis and management. The author is Dr Leah Gellert, consultant gastroenterologist and hepatologist, Bondi Junction, NSW. 30 | Australian Doctor | 8 March 2013 www.australiandoctor.com.au