Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
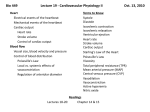
Europace (2005) 7, S118eS127 New developments in a strongly coupled cardiac electromechanical model David Nickerson, Nicolas Smith, Peter Hunter* Bioengineering Institute, University of Auckland, Level 6, 70 Symonds Street, Auckland, New Zealand Submitted 12 January 2005, and accepted after revision 3 May 2005 KEYWORDS cardiac electromechanics; computational model; finite element Abstract Aim The aim of this study is to develop a coupled three-dimensional computational model of cardiac electromechanics to investigate fibre length transients and the role of electrical heterogeneity in determining left ventricular function. Methods A mathematical model of cellular electromechanics was embedded in a simple geometric model of the cardiac left ventricle. Electrical and mechanical boundary conditions were applied based on Purkinje fibre activation times and ventricular volumes through the heart cycle. The mono-domain reaction diffusion equations and finite deformation elasticity equations were solved simultaneously through the full pump cycle. Simulations were run to assess the importance of cellular electrical heterogeneity on myocardial mechanics. Results Following electrical activation, mechanical contraction moves out through the wall to the circumferentially oriented mid-wall fibres, producing a progressively longitudinal and twisting deformation. This is followed by a more spherical deformation as the inclined epicardial fibres are activated. Mid-way between base and apex peak tensions and fibre shortening of 40 kPa and 5%, respectively, are generated at the endocardial surface with values of 18 kPa and 12% at the epicardial surface. Embedding an electrically homogeneous cell model for the same simulations produced equivalent values of 36.5 kPa, 4% at the endocardium and 14 kPa, 13.5% at the epicardium. Conclusion The substantial redistribution of fibre lengths during the early preejection phase of systole may play a significant role in preparing the mid-wall fibres to contract. The inclusion of transmural heterogeneity of action potential duration has a marked effect on reducing sarcomere length transmural dispersion during repolarization. ª 2005 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: C64 9 373 7599; fax: C64 9 367 7157. E-mail address: [email protected] (P. Hunter). 1099-5129/$30 ª 2005 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.eupc.2005.04.009 New developments in coupled cardiac electromechanical model Introduction The integration of cardiac electrical and mechanical experimental data and hypothesizes across multiple spatial scales and functions via mathematical modelling is arguably the most advanced example of a ‘Physiome’ [1] style framework. Detailed electrophysiological models of myocyte cellular [2,3] and subcellular processes incorporating genetic mutations [4] are now being linked to a large body of existing research for modelling the spread of electrical excitation throughout cardiac tissue and the whole heart (for reviews see [5e7]). Numerous methods have been developed to model the spread of electrical excitation varying from discrete models in which individual cells are electrically coupled to their neighbours via variable resistive elements (gap junctions) through to continuum based models. Similarly, detailed finite element continuum models incorporating anatomy, structure and passive mechanics have been coupled to cellular active tension (see [5,7] for reviews). The development of models of these two physical processes has occurred largely independently. However, coupled models of cardiac electromechanics which trigger mechanical contraction based on the calculated activation sequence have recently been developed to investigate the relationship between activation and contraction in the normal [8,9] and paced heart [10,11]. It is indicative of both the computational load and modelling complexities that in each of these studies the activation sequence has been calculated independently and then later used as the excitation wavefront to initiate contraction. Such an approach negates the possibility of incorporating the effects of electro-mechanical coupling due to, for example, length-dependent calcium binding or stretchdependent conductance changes that are characterized in some of the more recently developed myocyte models [2,12] and have also been shown to be important in tissue models [13,14]. While we can expect computational performance to continue to improve, in order to incorporate these coupling processes, or indeed new advances such as signal transduction models [15], gene regulation models [4] or metabolic models [16], a method is required which strongly couples tissue stretch and activation to cellular tension and membrane potential. The method we have developed uses cellular models of electromechanics to drive the dynamic active material properties of a continuum organ model while the cellular models themselves get S119 feedback from both the electrical excitation and the deforming mechanical model. The mechanical deformation of the geometric models also feeds into the excitation model affecting the propagation of electrical activation and cellular electrophysiology. In this study we use the developed framework to examine explicitly the effect of adding transmural electrical heterogeneity in the embedded cell models on global myocardial mechanics. Methods A computationally efficient cellular model was developed by coupling the Fenton and Karma [17] simplified activation model to the cardiac mechanics of Hunter et al. [18] which characterizes the length and calcium dependence of tension generation. This coupled model is termed below as FKHMT. For the purposes of coupling, a calcium transient (not explicitly included in the Fenton and Karma formulation) was calculated from the slow inward current based on the original intracellular calcium formulation in the Luo and Rudy [19] model on which the Fenton and Karma is based. Following the method described by Nickerson et al. [12], the activation model was then used to provide the calcium transient input required to drive the active and dynamic development of cellular tension. Three different parameter sets were used in this formulation to characterize the heterogeneous behaviour of myocardium produced by midmyocardial or M cells, located in the middle of the ventricular wall [20]. Parameter values of trZ150 ms for midmyocardial cells, 144 ms for epicardial and 142 ms for endocardial cells resulted in calculated single cell action potential durations (APD) of 437 ms, 352 ms and 329 ms, respectively, matching values found in human ventricular tissue [21]. This cellular model was then embedded in a simplified geometric model of the left ventricle (shown in Fig. 1a) based on a prolate geometry with 50 mm outer radius (at the base) and 60 mm longitudinal base apex dimensions represented using 128 tricubic Hermite finite elements in rectangular Cartesian coordinates. Wall thickness was set at 10 mm at the base tapering at the apex. The simple distribution of the epicardial, midmyocardial, and endocardial cell types prescribed transmurally in the model is illustrated in Fig. 1b. The microstructure of the models was defined such that the fibre angle varied sigmoidally over 120 between the endocardium and the epicardium. S120 D. Nickerson et al. Table 1 Tissue conductivities for the mono-domain activation model based on the values of Hooks et al. [27] Figure 1 (a) Simplified geometric model of the left ventricle and the reference rectangular Cartesian axes. The red arrows indicate the material fibre axis, the green arrows are aligned with the sheet axis, and the blue matches the sheet-normal axis. The mid-septum region of the left ventricle is indicated by the green endocardial surface. (b) Distribution of the three cell types described by the cell model as used in the heterogeneous left ventricle model. The epicardial cells are yellow, the midmyocardial cells blue, and the endocardial cells are drawn in red. The material properties for the electromechanical stimulations are referred to in this local embedded microstructure. Recent studies have shown that conclusive evidence for the use of fully orthotropic conductivities in tissue level models is not yet available [22]. Thus, the myocardial model was treated as transversely isotropic using a ratio of 10:1 [23], longitudinal:transverse to the fibre direction; parameters for the mono-domain activation model are shown in Table 1. The mechanical constitutive properties were also referenced to the microstructure using the non-linear pole-zero law [18] with the parameter values listed in Table 2 taken from Remme et al. [24]. This parameter set was applied to the regions of the model shown in Fig. 2 to characterize increased stiffness at the apex and base due to higher collagen and valve ring effects, respectively. Following the work of Tomlinson et al. [25] the initial activation times at points on the left Table 2 Material axis Value (mS mmÿ1) Fibre conductivity Sheet conductivity Normal conductivity 0.263 0.0263 0.0263 ventricular endocardial surface are specified to simulate Purkinje fibre activation. A stimulus current is then applied at these points following the specified activation profile. The applied stimulus distribution is shown in Fig. 3 where the stimulus times are derived from the initial activation times from the canine ventricular model of Tomlinson et al. [25]. As shown in Fig. 3, the earliest activation occurs in the lower mid-septal wall and the latest activation is toward the base of the free wall. The boundary conditions for simulating the four phases of the cardiac mechanical cycle were applied based on the temporal relationship between global contraction and electrical transients as described by a classical Wigger’s diagram [26]. At all time points throughout the cycle spatially constant pressures were applied over the entire endocardial surface. Prior to the initiation of activation the model was inflated to a cavity of pressure of 1.0 kPa. The isovolumic phase was implemented by adding a finite element mesh which represented the volume of blood in the left ventricle and was constrained such that these elements had a constant total volume. This cavity region was then coupled to the ventricular wall to act as feedback mechanisms to constrain weakly the deformation of the ventricular wall. Once pressure exceeded 10 kPa the ejection phase was initiated by allowing a central node in the cavity mesh to displace in the baseeapex axis of the model, thereby reducing cavity volume. Displacement Summary of the pole-zero material parameters used in the model [24] Type Parameter Apex Sub-apex Normal Base Coefficient k11, k22, k33 k12, k21, k13, k31, k32, k23 a11 a22 a33 a12, a21, a13, a31, a23, a32 b11, b22 b33 b12, b21, b13, b31, b23, b32 2.22 kPa 2.0 kPa 0.136 0.136 0.136 0.3 2.22 2.22 1.5 2.22 kPa 2.0 kPa 0.227 0.227 0.227 0.4 1.67 1.67 1.0 2.22 kPa 1.0 kPa 0.475 0.619 0.943 0.8 1.5 0.442 1.2 2.22 kPa 2.0 kPa 0.423 0.555 0.845 0.4 1.5 0.442 1.0 Pole Curvature New developments in coupled cardiac electromechanical model S121 1. Cellular fields from activation model 2. Interpolate cellular fields from influential GBFE nodes to Gauss points Figure 2 The apex nodes are shown as red spheres, the sub-apex as silver spheres, the normal nodes are gold spheres, and base nodes are green. The material parameters in Table 3 are specified at these nodes and linearly interpolated as required at intermediate spatial locations. 3. Solve cellular model at Gauss point 5. Solve FE model of the cavity node was controlled to match the left ventricular cavity volume transient described by the Wigger’s diagram, scaled to give a peak ejection fraction of 50%. The separate solution algorithms of the grid based finite element method (GBFE) for the monodomain equations (activation) and finite element method (FEM) of the finite deformations equations (mechanics), have previously been described elsewhere [27,28]. The solution process for coupling these two solution techniques together is summarized in Fig. 4. From the activation solutions solved using a time step of 0.01 ms and an average grid point spacing 200 mm the cellular fields were locally interpolated at the lower resolution gauss Figure 3 Illustration of the Purkinje-like stimulus used to approximate sinus rhythm in the left ventricle model; the left panel shows the septal wall and the right is the left ventricular free wall. The coloured endocardial surface shows the time of electrical stimulation of the endocardial surface, with red being the earliest activation at time 0 ms and blue the latest site of stimulation at 16 ms (the contour bands are in 2-ms intervals). The non-coloured regions of the endocardial surface have no stimulus current applied. A stimulus current of 150 mA mmÿ3 is applied to the coloured regions of the endocardial surface with duration of 1 ms. Converged? No Yes Figure 4 Schematic diagram of the algorithm developed for the calculation of active tension for a given Gauss point from the cellular values at the influential grid points. FE, finite element; GBFE, grid-based finite element. points in the mechanics mesh. Using these interpolated values the cell model was solved at the gauss point to determine regional active tension, which was then incorporated into the finite deformation mechanics model. The local strain was calculated at each activation grid point from the deformation and used to update the model cellular lengths. The relatively slower temporal dynamics of myocardial deformation means that this coupling update process could be implemented at a significantly larger time step, 1 ms, than the activation solution process. Results The membrane potential and myocardial deformation of the finite element mesh are shown in Fig. 5aeh at specific time points marked on Fig. 6 through the cardiac cycle to illustrate stages of activation and contraction. S122 D. Nickerson et al. Figure 5 Results from simulations of contraction and ejection in the heterogeneous left ventricular model. The green lines show the undeformed geometry and the element faces are coloured by the membrane potential spectrum shown above. 55 20 15 45 10 Cavity pressure Cavity volume 5 0 0 35 25 100 200 300 400 500 600 700 800 900 1000 Cavity volume (ml) Cavity pressure (kPa) At the eight locations in the finite element mesh shown in Fig. 7a the calculated strain, active tension and membrane potentials are illustrated through the cardiac cycle in Fig. 7bed. Using the Purkinje-like stimulus the smooth transmural progression of electrical activation is clear, with full ventricular activation occurring after 70 ms. The repolarization wave begins at the apical epicardium approximately at 270 ms and progresses toward the endocardial surface and basal plane. The mid-wall at the base of the ventricle is the last tissue to repolarize approximately at 490 ms. With the simple transmural fibre variation illustrated in Fig. 1a and the sequence of contraction solutions given in Fig. 7, we show that Time (ms) Figure 6 The imposed cavity volume and calculated ventricular pressure and through the cardiac cycle (see text). the left ventricle initially deforms into a more spherical shape with just the endocardial region actively contracting. Then as the mechanical activation moves out through the wall to the circumferentially oriented mid-wall fibres, the deformation becomes more longitudinal and the twisting motion begins. This is followed once more by a move toward more spherical deformation as the inclined epicardial fibres are activated and the twisting increases. An important feature of this heterogeneous model is the reversal of the direction in which the repolarization wave travels through the wall. During the repolarization phase of the cycle the model maintains a higher cavity pressure due to the prolonged action potentials of the midmyocardial cells, giving rise to increased active tension at the cellular level. The peak pressure achieved by the model during ejection is consistent with values reported in similar models [9]. To interpret the sequence of electrical and mechanical events taking place during the pre-ejection phase of systole, the results shown in Fig. 7 are reproduced on an expanded 200 ms time scale in Fig. 8. The electrical activation sequence is endocardium to epicardium with the free wall endocardial point shown in yellow (B) on the left of the ventricular model in Fig. 7a being activated 50 ms New developments in coupled cardiac electromechanical model S123 1.15 Extension ratio () 1.1 1.05 1 0.95 0.9 0.85 0 200 400 600 800 1000 Time (ms) (a) (b) 20 Membrane potential (mV) Active tension (kPa) 40 30 20 10 0 0 200 400 600 800 1000 0 -20 -40 -60 -80 0 200 400 600 Time (ms) Time (ms) (c) (d) 800 1000 Figure 7 The temporal variation in cellular signals from locations within the finite element model. The colour of each trace in (b)e(d) matches the corresponding sphere in (a) which indicates the spatial location of the cell from which the signal is calculated. Locations in the mid-wall are labelled AeF. after the septal wall endocardial point shown in grey (A) on the right. The septal transmural points (endocardial to epicardial) shown as grey (A), orange (C) and black (E) are separated by 100 ms intervals (easiest to see in Fig. 8b) as are the (slightly later) transmural sequence of free wall points shown as green (B), light blue (D) and purple (F). The earliest mechanical response is seen in Fig. 8a is fibre shortening at A, 15 ms after the electrical stimulus at A. The mechanical consequence of the active septal endocardial shortening is stretching of the still passive adjacent mid-wall fibres at C. The next point to activate is the free wall endocardial point B which begins contracting 15 ms later and similarly causes substantial lengthening of mid-wall fibres at point D. The third point to activate is the mid(septal)-wall point C at about 22 ms and 15 ms later its active response d which follows the ‘pre-stretch’ d can be seen in Fig. 8a as fibre shortening. The mid-wall fibres at C and D next begin to shorten (at 35 ms and 45 ms, respectively) and contribute to the very substantial lengthening of epicardial fibres at E and F which, following their passive pre-stretch, begin their contraction about 15 ms after excitation such that by 60 ms all points are activated. Note, however, that the fibre shortening at points A and B is temporarily reversed as the contracting mid-wall and then epicardial fibres exert their influence. This substantial redistribution of fibre lengths during the early pre-ejection phase of systole may play a significant role in preparing the mid-wall fibres to contract. By 80 ms ventricular pressure has risen sufficiently to begin ejection. To assess the potential influence of cellular heterogeneity on myocardial deformation, specifically during repolarization, the above simulation was repeated using a homogeneous distribution of cellular models (trZ144 ms and APDZ352 ms). Figs. 9 and 10 contrast the model extension ratios and active tension transients in the heterogeneous and homogeneous models and Table 3 provides data on the transmural APD dispersion in the septum and free wall of the model. In the heterogeneous model the sequence of repolarization, as specified by the APD assigned to different regions through the left ventricular wall, is epicardial first (points E, F in Fig. 7a), then endocardial (points S124 D. Nickerson et al. 1.15 1 D Extension ratio () F Extension ratio () C 1.1 1.05 B 1 E A 0.95 A 0.95 B C 0.9 D E 0.9 0.85 F 0 50 100 150 0.85 200 200 300 350 400 450 Time (ms) (a) Extension ratio of the first 200ms of the cardiac cycle (a) Calculated extension ratios for the heterogeneous model during repolarisation 20 1 0 A Extension ratio () Membrane potential (mV) 250 Time (ms) -20 A B C D E F -40 -60 0.95 B C D 0.9 E -80 0 50 100 150 200 Time (ms) (b) Membrane potential for the first 200ms of the cardiac cycle Figure 8 An enlargement of the results in Fig. 7bed showing the temporal variation in extension ratio (a) and membrane potential (b) from the locations labelled AeF in Fig. 7a for the first 200 ms of the cycle. A, B), and then mid-wall (points C, D). The initial epicardial repolarization is reflected in the rapid early sarcomere length increase from 300 ms on in the sub-epicardium in Fig. 7b (and in expanded form in Fig. 9 for both homogeneous and heterogeneous models). The sarcomere lengths at the mid-wall points C, D begin increasing at about 360 ms for both the homogeneous and heterogeneous models. The major consequence of assuming homogeneous APDs (Fig. 9b) is a substantially more dispersed transmural sarcomere length variation. For example, at 400 ms fibre extension ratio distribution in the homogeneous model is 0.9 to 0.98, whereas in the heterogeneous model it is reduced to 0.91 to 0.96. Within the sub-epicardium and mid-wall region the range is only 0.91 to 0.92. Discussion The simulation results presented above demonstrate that the modelling and simulation framework developed and implemented works well for coupled electromechanical models using a three-dimensional geometry representative of the cardiac left 0.85 200 250 F 300 350 400 450 Time (ms) (b) Calculated extension ratios for the homogeneous model during repolarisation Figure 9 An enlargement of extension ratios from 200 to 450 ms (during repolarization) in: (a) the heterogeneous model accounting for the transmural variation in action potential durations; (b) the homogeneous model. ventricle. Two specific insights have been provided by this study. The first is the important role that electrical heterogeneity may play in reducing the transmural sarcomere length variation during repolarization. The implications for this effect, including distribution of mechanical work and the metabolic efficiency of the whole heart, provide interesting avenues for future investigation via an electromechanical model. The second insight provided by the model is into the detailed relationship between activation times, shortening and spatial location within the myocardium. In particular, the possibility of endocardial stretch during late isovolumic contraction has not previously been reported. The results in Fig. 8a show a significant heterogeneity of strain at end isovolumic contraction which is consistent with the model results of Kerckhoffs et al. [8]. However, this result is inconsistent with experimental data that report a relatively homogeneous distribution of strain and work throughout the myocardium [29]. Thus, possible influences such as geometry, complex fibre angle variation and a spatial distribution of delay New developments in coupled cardiac electromechanical model Active tension (kPa) 40 A B 30 C 20 E D F 10 0 200 250 300 350 400 450 Time (ms) (a) Calculated active tension in the heterogeneous model during repolarisation. Active tension (kPa) 40 B 30 A C 20 10 E D F 0 200 250 300 350 400 450 Time (ms) (b) Calculated active tension in the homogeneous model during repolarisation. Figure 10 An enlargement of calculated active tension from 200 to 450 ms (during repolarization) in: (a) the heterogeneous model accounting for the transmural variation in action potential durations; (b) the homogeneous model. between excitation and activation may ultimately need to be included in the model. It is also important to note that the single beat simulated in this study is effectively modelling a very slow steady-state heart rate where the cells prior to stimulation are always at, or close to, the initial condition set in this model. This may explain the differences between model and experimental results. However, to characterize more effectively, these memory effects where ionic concentrations Table 3 Comparison of the transmural APD dispersion in the homogeneous and heterogeneous models Spatial location Homogeneous model (ms) Heterogeneous model (ms) A B C D E F 362 360 351 350 344 339 437 434 418 417 367 367 The spatial locations of points AeF are illustrated in Fig. 7a. S125 and gating variables at stimulation are dependent on heart rate, a more biophysical basis to the cell model is required. The most significant drawback in the framework highlighted by these simulations is the sheer amount of time taken to obtain these results, the coupled electromechanics simulations shown in Figs. 6 and 7 took in the order of three weeks to achieve 1000 ms of simulation time using an IBM Regatta P690 high-performance computer implemented in parallel on eight processors. Furthermore, despite the large computational load imposed by high spatial resolution grids, numerical artefacts remain. A small error associated with grid discretization is shown in the brief hyperpolarization prior to upstroke. Also, the sensitivity of the lengtheactive tension coupling produces rapid oscillations in calculated active tension during contraction induced by finite time stepping in the numerical method. However, on the time scale of myocardial mechanics these variations have little effect on ventricular deformation although ultimately physiological based viscous damping will need to be added completely to eliminate the oscillations. It is this computational limitation which currently also precludes the inclusion of a more detailed cellular model. Such a model could potentially account for mechano-electric feedback and stretch dependence, which can now be explicitly linked to the tissue simulations via the strong coupling solution procedure outlined in Fig. 4. It is this coupling between cellular contraction and activation that Kerckoffs et al. [8] propose as a possible mechanism to produce a heterogeneous electromechanical delay that is required simultaneously to produce both physiological activation and contraction spatio-temporal sequences. The framework is sufficiently general, such that new cell models can be accommodated without changing the existing software tools. Thus, as computational resources continue to increase rapidly, we anticipate that in the near future we will be using this framework with more detailed biophyisically based cell models. This generality has been implemented using the CellML language [30,31] to embed the cellular models in the continuum simulations. A general application programme interface (API) has been developed (freely available at http://cellml.sourceforge.net) to provide a layer of abstraction between an application and the implementation of a CellML processing library. Using the API a list of the cellular equations was generated for the model and a specific maths writer was developed to create a S126 Fortran subroutine from the cellular equations which could then be compiled and linked with our CMISS simulation environment (freely available for academic use at http://www.cmiss.org). The CellML model repository (http://www.cellml.org/ examples/repository/index.html) provides an extensive database of cellular models of cardiac electrophysiology and mechanics. Thus, it is largely only computational resources that prevent repeating the above study with a detailed biophysically based cellular model. To assess the computational requirements of a more detailed cellular model we have run electromechanics simulations using a 4!4!4 mm cube of cardiac tissue using a 200 mm grid point spacing. With a reduced number of grid points it was possible to compare the computational performance with the simplified model FK-HMT model used above with a biophysically based coupled LRd-HMT model [4,18]. Profiling of these simulations showed the additional biophysical detail produced a threefold increase in memory usage and a tenfold increase in computational time. Thus, applying the often quoted Moore’s Law, a strongly coupled cardiac electromechanics simulation using a detailed cell model will be likely to be feasible within the next three years. Future developments within that timeframe also include solving electromechanical models using more realistic anatomical and microstructural models [32,33] and coupling three-dimensional ventricular fluid dynamics solutions to determine the endocardial boundary conditions. Within the wider scope of the Physiome Project we aim to enhance further the modelling framework with the use of markup languages such as CellML (as discussed above) and other ontologies under development. For example, a markup language to represent the spatial variation of fields used in the models (FIELDML: http://www. physiome.org.nz) is also being developed. In doing so we aim to improve the accessibility of models across spatial scales and accelerate the development, validation and application of mathematical models of the heart and other organs. Acknowledgements P.J.H. and D.P.N. acknowledge the support of the Centre for Molecular Biodiscovery. N.P.S. acknowledges support from the Marsden Fund and New Zealand Institute of Mathematics and its Applications. All authors gratefully acknowledge contributions by colleagues in the Auckland Bioengineering Institute. D. Nickerson et al. References [1] Hunter PJ, Borg TK. Integration from proteins to organs: the Physiome Project. Nat Rev Mol Cell Biol 2003;4:237e43. [2] Noble D, Varghese A, Kohl P, Noble P. Improved guinea-pig ventricular cell model incorporating a diadic space, IKr and IKs, and length- and tension-dependent processes. Can J Cardiol 1998;14(1):123e34. [3] Hund TJ, Kucera JP, Otani NF, Rudy Y. Ionic charge conservation and long-term steady state in the Luo-Rudy dynamic cell model. Biophys J 2001;81(6):3324e31. [4] Clancy CE, Rudy Y. Na(C) channel mutation that causes both Brugada and long-QT syndrome phenotypes: a simulation study of mechanism. Circulation 2002;105:1208e13. [5] Smith NP, Nickerson D, Crampin EJ, Hunter PJ. Computational modelling of the heart. Acta Numer 2004;13: 371e431. [6] Kleber AG, Rudy Y. Basic mechanisms of cardiac impulse propagation and associated arrhythmias. Physiol Rev 2004; 84:431e88. [7] Hunter PJ, Pullan AJ, Smaill BH. Modelling total heart function. Annu Rev Biomed Eng 2003;5:147e77. [8] Kerckhoffs RC, Bovendeerd PH, Kotte JC, Prinzen FW, Smits K, Arts T. Homogeneity of cardiac contraction despite physiological asynchrony of depolarization: a model study. Ann Biomed Eng 2003;31(5):536e47. [9] Usyk TP, Le Grice IJ, McCulloch A. Computational model of three-dimensional cardiac eletromechanics. Comput Visual Sci 2002;4:249e57. [10] Kerckhoffs RC, et al. Timing of depolarization and contraction in the paced canine left ventricle: model and experiment. J Cardiovasc Electrophysiol 2003;14:S188e95. [11] Usyk TP, McCulloch A. Electromechanical model of cardiac resynchronization in the dilated failing heart with left bundle branch block. J Electrocardiol 2003;36:57e61. [12] Nickerson D, Smith NP, Hunter PJ. A model of cardiac cellular electromechanics. Phil Trans R Soc Lond A 2001; 359:1159e72. [13] Smith NP, Buist ML, Pullan AJ. Altered T wave dynamics in a contracting cardiac model. J Cardiovasc Electrophysiol 2003;14:S203e9. [14] Li W, Kohl P, Trayanova N. Induction of ventricular arrhythmias following mechanical impact: a simulation study in 3D. J Mol Histol 2004;35:679e86. [15] Saucerman JJ, McCulloch AD. Mechanistic systems models of cell signaling networks: a case study of myocyte adrenergic regulation. Prog Biophys Mol Biol 2004;85:261e78. [16] Smith NP, Crampin EJ. Development of models of active ion transport for whole-cell modelling: cardiac sodiumpotassium pump as a case study. Prog Biophys Mol Biol 2004;85:387e405. [17] Fenton F, Karma A. Vortex dynamics in three-dimensional continuous myocardium with fiber rotation: filament instability and fibrillation. Chaos 1998;8:20e47. [18] Hunter PJ, McCulloch AD, ter Keurs HE. Modelling the mechanical properties of cardiac muscle. Prog Biophys Mol Biol 1998;69:289e331. [19] Luo CH, Rudy Y. A model of the ventricular cardiac action potential. Depolarization, repolarization, and their interaction. Circ Res 1991;68:1501e26. [20] Antzelevitch C, Sicouri S, Litovsky SH, Lukas A, Krishnan SC. Heterogeneity within the ventricular wall. Electrophysiology and pharmacology of epicardial, endocardial, and M cells. Circ Res 1991;69(9):1427e49. [21] Drouin E, Charpentier F, Gauthier C, Laurent K, Le Marec H. Electrophysiologic characteristics of cells spanning the left New developments in coupled cardiac electromechanical model [22] [23] [24] [25] [26] ventricular wall of human heart: evidence for presence of M cells. J Am Coll Cardiol 1995;26(1):185e92. Colli-Franzone P, Guerri L, Taccardi B. Modeling ventricular excitation: axial and orthotropic anisotropy effects on wavefronts and potentials. Math Biosci 2004;188: 191e205. Roth BJ. Electrical conductivity values used with the bidomain model of cardiac tissue. IEEE Trans Biomed Eng 2003;44:326e8. Remme E, Nash MP, Hunter PJ. Distributions of sacromere stretch, stress and work in a model of the beating ventricles. In: Kohl P, Franz M, Sachs F, editors. Cardiac mechanoelectric feedback and arrhythmias: from pipette to patient. Philadelphia: Saunders; 2004. p. 381e91. Tomlinson KA, Pullan AJ, Hunter PJ. A finite element method for an eikonal equation model of myocardial excitation wavefront propagation. SIAM J Appl Math 2002; 63:324e50. Katz A. Physiology of the heart. 2nd ed. New York: Raven Press; 1992. p. 361e64. S127 [27] Hooks DA, et al. Cardiac microstructure: implications for electrical propagation and defibrillation in the heart. Circ Res 2002;91:331e8. [28] Nash MP, Hunter PJ. Computational mechanics of the heart. J Elasticity 2001;61:113e41. [29] Prinzen FW, Hunter WC, Wyman BT, McVeigh ER. Mapping of regional myocardial strain and work during ventricular pacing: experimental study using magnetic resonance imaging tagging. J Am Coll Cardiol 1997;33:1735e42. [30] Lloyd C, Halstead M, Nielsen P. Cell ML: its future, present and past. Prog Biophys Mol Biol 2004;85:433e50. [31] Cuellar AA, Lloyd CM, Nielsen PF, Bullivant DP, Nickerson D, Hunter PJ. An overview of CellML 1.1 a biological model description language. Simulation 2003;79(12):740e7. [32] Nielsen PM, Le Grice IJ, Smaill BH, Hunter PJ. Mathematical model of geometry and fibrous structure of the heart. Am J Physiol 1991;260:H1365e78. [33] Stevens C, Hunter PJ. Sarcomere length changes in a 3D mathematical model of the pig ventricles. Prog Biophys Mol Biol 2003;82:229e41.