Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
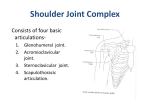
Glenoid Version Measurement when the Medial Scapula Is Not in the Cross-Sectional Imaging Field of View +1,2Robertson, D D; 1,3Sharma, G B; 4Kang, M D; 5Stone, D A; 1,5McMahon, P J University of Pittsburgh, Bioengineering, USA; +2Emory Spine and Orthopaedic Center, USA; 3University of Calgary, Mechanical and Materials Engineering, Canada; 4University of Pittsburgh Medical Center, Radiology, USA; University of Pittsburgh Medical Center, Orthopaedic Surgery, USA [email protected] 1 Introduction: Glenoid version, glenoid surface orientation in the axial plane, has an important role in the passive stabilization of the articular components of the glenohumeral joint1. Glenoid shape and version has been associated with glenohumeral instability2, arthritis3, and rotator cuff tears4. Cross-sectional computed tomography (CT) and magnetic resonance (MR) imaging have been demonstrated to be more accurate than radiography for measuring glenoid version5. Glenoid version calculation requires a transverse scapular axis, often defined as a line connecting the glenoid fossa midpoint with the scapular spine medial endpoint6. Other transverse axis definitions include a line perpendicular to the glenoid surface midpoint or a line tangent to either the posterior or anterior glenoid rim7. Prior studies require identification of scapula's medial border to measure glenoid version. Clinical shoulder joint crosssectional imaging frequently uses a reduced field of view (FOV) without visualizing scapula's medial border. Thus preventing replication of the published methods. No method is currently available to measure glenoid version in routine shoulder cross-sectional imaging studies where the medial scapular border is not in the FOV. The purpose of this study was to design and validate a method to accurately measure glenoid version on cross sectional clinical CT shoulder images, where the FOV does not include the entire scapula. Materials and Methods: Forty unembalmed, fresh scapulae cadavers (20 pairs, 10 male, 10 female, mean age: 52±18 years, mean height: 171±12 cm). Exclusion criteria were moderate or severe arthritis, or bony radiographic abnormalities in any one of the pair. None of the included donors had any surgical procedure performed on their scapulae or humeri. This study was approved by the University of Pittsburgh's Institutional Review Board. All scapulae were radiographed anteroposteriorly and laterally. Each scapula was placed in a custom fixture replicating a neutral supine position and adjusted to minimize/eliminate version measurement inaccuracies due to scapula rotation. CT was used to validate the new cross-sectional glenoid version measurement methodology, although the results can be directly applied to MR imaging as well. The middle third of the medial edge of the scapula was positioned parallel to the long axis of the CT table such that the slices were approximately perpendicular to the glenoid articular surface (Fig. 1). High-resolution volumetric CT axial images (slice thickness: 1 mm, FOV: 20×20 cm2) were obtained producing a “patient supine clinical simulation” CT image study. Fig. 1. Scapula orientation for crosssectional imaging. Slice location is selected axial slice for version measurement. 3D computer models were generated for each scapula using bone segmentations (Amira®). The axial slice similar to that passing through the 3D scapula model’s glenoid center was selected from the “patient supine clinical simulation” CT images data set. The selected CT axial slice was used to measure glenoid version on “full-scapula” and “partial-scapula” FOV images. “Full-scapula” FOV true glenoid version were measured as the angle between the line joining the anterior and posterior glenoid margins with the horizontal6 (Fig. 2A). Fig. 2. (A) “Full-scapula” image true glenoid version measurement. (B) “Partial-scapula” image glenoid version (*) measurement. To closely resemble the clinical situation, the selected CT images were cropped to exclude the medial portion. Glenoid version was measured on the cropped images: line A connected the anterior and posterior glenoid articular margins, the transverse axis line B connected the point of intersection of the cortical bone within the scapula neck to the midpoint of line A, line C was perpendicular to line B. Glenoid version was the angle between line A and line C and retroverted if the posterior margin was below line C (Fig. 2B). The mean and standard deviation for “full” and “partial-scapula” glenoid version were computed. Differences between gender and sidedness were tested with two-tailed independent and paired samples ttests (SPSS, Inc., level of significance:0.05). Original and repeat “full” and “partial-scapula” glenoid version measurements were made two times by three observers. Each observer was trained using three additional sample cases not included in the analysis. Repeated measures ANOVA tested for differences between “partial-scapula” glenoid version measurements across the three observers, two occasions, and three observers-two occasions. Test-retest reliability (precision) was defined as the mean difference between repeated measurements of “partial-scapula” glenoid version. Inter- and intra-observer reliability were estimated using intraclass correlation (ICC) and standard error of measurement (SEM). Accuracy was defined as the mean difference between “full-scapula” glenoid version (truth) and “partial-scapula” glenoid version measurements. A correction factor was calculated and applied to the three observers “partial-scapula” glenoid version measurements. One-way ANOVA analysis tested for mean differences between “full” and “partial-scapula” glenoid version measurements for the original and corrected data. Results: Overall, males were more retroverted (-3°±3°; p=0.02) than females (0°±3°). Glenoid version in rights and lefts was approximately equal (-2°±4°; p = 0.95). “Full-scapula” glenoid version (-0.4°±3°) was less retroverted than that from the “partial-scapula” image (-7.5°±3°; p=0.01). “Partial-scapula” glenoid version measurements were reliable. Table 1 gives ICC and SEM results. Glenoid version measurement accuracy was 7.1°±4.0°. Adding a 7° correction factor to “partialscapula” glenoid version measurements yielded values not significantly different than truth (-0.5°±3°; p=0.995). Table 1. ICC and SEM results. InterIntra-Observer Observer 1 2 3 0.7233 0.6349 0.8953 0.9175 ICC SEM 1.6° 2.2° 0.9° 0.9° 0.0001 0.0111 0.0001 0.0001 P-Value Discussion: This study described and validated a new method for accurately measuring glenoid version on “partial-scapula” axial crosssectional images. Scapular positioning to obtain accurate glenoid version measurement was optimized. As per literature this was needed whether the FOV includes the full scapula or not3,5,7. Glenoid version varies from superior to inferior glenoid8. Clinical utilization has chosen the mid glenoid for measuring. This is the position we selected to test and validate. As all tested scapulae were “normal”, this technique was not demonstrated for use in dysplastic or deformed scapulae. CT was more accessible for our research. Nevertheless, the principles validated here are applicable to MR imaging. This study demonstrated that true glenoid version is different than “partial-scapula” glenoid version. However, the inaccuracy of the partial scapula view version measurements can be reduced if not completely eliminated by a correction factor. Significance: To improve spatial resolution and examination of shoulder structure clinical CT and MR imaging studies frequently exclude the entire scapula preventing replication of previously published glenoid version measurements. A novel measurement method is presented to enable version measurements on “partial-scapula” cross-sectional imaging studies. References: [1] Churchill, 2001, J Shoulder Elbow Surg, 10(4). [2] Wirth, 1994, Clin Orthop Rel Res, 308. [3] Hoenecke, 2010, J Shoulder Elbow Surg, 19(2). [4] Tetreault, 2004, J Orthop Res, 22(1). [5] Nyffeler, 2003, J Shoulder Elbow Surg, 12(5). [6] Friedman, 1992, J Bone Joint Surg Am, 74(7). [7] Rouleau, 2010, J Shoulder Elbow Surg, 19(8). [8] Inui, 2002, Clin Orthop Rel Res, 403. Poster No. 2222 • ORS 2012 Annual Meeting