Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropharmacology wikipedia , lookup
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Psychopharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Plateau principle wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Ciprofloxacin wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Theralizumab wikipedia , lookup
List of comic book drugs wikipedia , lookup
Update on the Pharmacodynamics
Pharmacokinetics
of Theophylline*
Leslie
Hendeles,
Pharm.D.;t
Miles
Weinberger,
M.D.
Marc
Massanari,
Pharm.D.;
theophylline’s
unlmown.
concentrations
where
obtaining
maximal
have the potential
tions
mechanism
10 to 20
Often,
of action
is used
pg/ml
there
benefit
the
is
the 15 formulations
use. Often
these
T heophylline
has
agent
controlling
for
asthma
during
States.
This
pharmacokinetics
greatest
is
of serum
of
likelihood
Slow-release
safely.
products
sold under
29 brand
with more rapid
slow absorption
names in this country.
In patients
tion, few products
have sufficiently
twice-daily
in asthma
as the range
to provide
more stable serum concentradosing intervals.
However,
clinically
imin rate and sometimes
extent of absorp-
longer
portant
differences
tion exist between
with
and
§
Theophylline
has emerged
as a major prophylactic
agent for
controlling
the symptoms
of chronic
asthma,
but it provides
little if any relief of pulmonary
symptoms
caused
by irreversible chrome
airways
obstruction.
Although
in vitro
it
inhibits
phosphodiesterase
and antagonizes
adenosine
receptors,
and
formulations
emerged
must
as a major
the
eliminato allow
be adminis-
every eight hours to prevent
breakthrough
in asthsymptoms
despite
promotional
claims to the confrar
In patients
with slower
elimination,
differences
among
products are unlikely to be clinically
important
with 12-hour
dosing intervals.
Current
products
approved
for “once-aday” dosing are clinically
inadequate
because of erratic
absorption
or excessive serum concentration
fluctuations.
Moreover,
food induces dose dumping
of potentially
toxic
amounts of theophylline
from
Theo-24, greatly
increases the
extent of absorption
of theophylline
from Uniphyl,
decreases extent of absorption
from Theo-dur-Sprinkle
capsules, but has no clinically
important
effect on Theo-Dur
tablets, Theobid,
Sb-Bid,
or Somophyllin-CRT.
The effects
of food or other factors that alter gastrointestinal
physiology
on theophylline
absorption
are unknown
for most other
products.
tered
matic
prophylactic
symptoms
of
PHARMACOLOGY
chronic
the past 10 to 15 years
in the United
has been
a result
of definition
of its
and pharmacodynamics,
the availa-
The mechanism
of theophylline’s
chial smooth
muscle
relaxant
remains
tion of phosphodiesterase
mechanism,
but this
bility
of rapid
specific
methods
of measuring
serum
concentrations,
and the development
of reliably
absorbed
slow-release
formulations.
that used
Furthermore,
Since there
have been
a great many of articles,
book
chapters,
and proceedings
from
symposia
published
on theophylline,
this review
will focus on only the most
chodilators.
recent
advances
we recognize
in knowledge
about
this
that
many
adult
patients
degrees
of airway
hyperreactivity
varying
with
an irreversible
well-controlled
benefit
from
symptoms
Therefbre,
refers
chronic
component
studies
have
theophylline
of airways
caused
by irreversible
to avoid confusion,
to reversible
irreversible
airways
airways
no
obstruction,
little or no
pulmonary
obstruction.
airway
“asthma”
in this
obstruction
and
article
COPD
to
Pediatrics,
University
Pharmacokinetics,
§Professor
of Pediatrics
and Chairman,
nary Division,
University
of Iowa.
Reprint
requests:
Dr
Hendeles,
Box
Florida,
Gainesville
32610
Pediatric
of Florida.
College
of Phar-
Allergy
J-4. JHMHC.
and PulmoUniveristy
and
Thus,
longer
be
of
be toxic in vivo.6
inhibitors
such
papaverine
are
phosphodiesterase
accepted
as
the
that
but
not
bron-
inhibition
can
of
mechanism
theophylline
effects
the-
may act as a
on intracellular
calcium8
and increased
binding
of cyclic AMP (cAMP)
to cAMP-binding
protein9
also have been
described.
Recently,
theophylline
has been
shown
to antagonize
adenosine
induced
by
by
receptors
adenosine
in vitro,
Enprofylline
and
to block
bronchial
adenosine
enprofylline,
potency
8Fmm the Division
of Clinical
Pharmacokinetics,
College of Pharmacy and Department
of Pediatrics,
University
of Florida,
Gainesville,
and the Pediatric
Allergy and Pulmonary
Division,
The University
of Iowa, Iowa City.
f Professor
of Pharmacy
and
Fellow,
Division
of Clinical
macy,
University
of Florida.
dipyridamole
ever,
obstruction.
has been a popular
proposed
is based
on in vitro studies
concentrations
that would
other phosphodiesterase
ophylline’s
action.
It has been suggested
pmstaglandin
antagonist,7
drug.
While
may
have
combined
demonstrated
in relieving
as
theory
action
as a bronelusive.
Inhibi-
receptors
a xanthine
as
bronchoconstriction
provocation.’0
derivative
that
a bronchodilator
than
does
gastric
not
How-
are not antagonized
stimulate
has
greater
theophylline.”
acid
secretion
or diuresis
and has less CNS and cardiac
toxicity
than
theophylline,
suggesting
that adenosine
antagonism
may
be responsible
for some
of the side effects
of
methylxanthines’2
As with
other
but not their
methylxanthines
theophylline
produce
transiently
can
increase
CHEST
cerebral
plasma
/ 88 / 2 / AUGUST,
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
bronchodilator
such
effects.
caffeine,
vasoconstriction,
glucose,
1985
as
and
I Supplement
inhibit
1O3S
uterine
contractions.#{176}
actions
on
centrations
It also
exerts
the cardiopulmonary
>10 p.g/ml
increase
a complex
set
of
system.
Serum
concontractility
and re-
companies
whose
products
recommendations
within
the
and/or
cannot
10 to 20 ig/ml
Similarly,
dosing
maintain
range
arguments
around
for
interval
concentrations
using
the
clock.
“low-dose”
the-
duce experimentally
induced
fatigue
of diaphragmatic
muscles,’4
decrease
the work
of breathing,4
increase
biventricular
performance,’5
stimulate
hypoxic
yen-
ophylline
in combination
been
based
on single-dose
tilatory
sion,’7
hypertenHowever,
ditive
bronchodilator
effects.
There
are no
comparing
the
relative
efficacy
and
safety
studies
of the
are
combination
of
drive,’6
reduce
pulmonary
artery
and enhance
mucociliary
clearance.’8
it is unclear
clinical
from
if these
importance
pharmacologic
or result
effects
in the
relief
of any
PHARMACODYNAMICS
range
various
studies
published
of theophylline
of serum
have
on
led
the
efficacy
to a carefully
concentrations,
and
defined
between
10 and
20
p.g/ml,
where
there
is an optimal
likelthood
of maximal
safe effect.’
It is this optimal
range
for maximal
safe
effect that has been commonly
termed
the “therapeutic range.”
The connotations
of this term
have sometimes
effect
der
been
from
10 p.g/ml
misinterpreted
to suggest
theophylline
and
at serum
no further
argue
that
theophylline
tions,#{176} and
tainly
would
However,
ward
this
is
the
studies
extension
serum
over
literature,
so.
A
that
of the
been
effect
un-
20 g/ml.
however,
Even
a
would
measurable
have
therapeutic
limited
or some
is no
for antiasthmatic
effect
is apparent
at lower
serum
higher
serum
concentrations
provide
more
effect for some
generally
have
bronchodilator
lower
not
there
concentrations
potential
effect
at serum
concentrations
cursory
examination
of the
that
argued
for a down-
range
to 5 pg/ml
to demonstration
decrease
in symptoms
concentrations
of
concentraalmost
cerpatients.
and
have
not
strated
that the measurable
effects
imal
or, alternatively,
associated
were
with
indeed
a lower
of a
at
demonmaxfre-
quency
of side
effects
than
serum
concentrations
within
the 10 to 20 pg/ml
range.
Moreover,
no studies
examining
the efficacy
of serum
concentrations
less
than 10 pg/ml
have demonstrated
degree
of efficacy
of theophylline
the remarkably
in preventing
toms that interfere
with sleep,’92’
reduction
for emergency
medications19
n3#{176}including
steroids,2
and blocking
of exercise-induced
chospasm3#{176} documented
pg/ml.
As to the argument
attained
ftr some patients
concentrations
safe clinical
effect
The
most
is well
in need
corticobron-
at concentrations
above
10
that more effects
might
be
at serum
concentrations
over
20 pg/ml,
it is acknowledged
not with adequate
safety.
serum
high
symp-
that this may
10 to 20 g/ml
likely
supported
to obtain
by multiple
be so, but
range for
maximal
clinical
104S
decreases
with
exercise-induced
these
drugs
on an annual
basis,
expensive
and less
theophylline
doses,
even
doses
the
symptoms.
This
since the intensity
13 agonists,3#{176} and
not inhibited
when
ments
titrated
suppressing
of asthmatic
important,
have
ad-
the-
frequency
and
would
be
and duration
parof
continued
use
bronchospasm
are given orally.
of oral
is
Last,
#{176}
the combination
therapy
is more
convenient
than
a slow-release
product
when
the
used
cost
alone
in individualized
of serum
level
measure-
is included.
Thus,
the
target
issue
then
10 to 20 g/ml
safe
maximal
is no longer
range
effect
is
when
products,
and
the
whether
optimal
desired,
but
maintain,
and
sustain
these
given the interpatient
variability,
realities
or not
to
likelihood
how
to
of
attain,
serum
concentrations
the range of available
of patients’
lifestyles.
COPD
Although
serum
a
definite
relationship
concentration
asthma,
serum
pulmonary
and
over,
several
ies’5
have
exists
effect
concentrations
function
in
in patients
double-blind,
with
patients
exercise
be
tients
with
investigated
most
the
noticeable
COPD
effect
4
in
of theophylline
walking,
a large
in
since
increase
El
Placebo
0
Theophyllune
riririririri
Cough
stud-
rest (standing)
and
any potential
benefit
during
experience
Wheezing
with
COPD.#{176}4 More-
and theophylline
at
(Fig 1). Jenne
et al,4
with emphysema
during
(walking).
Theoretically,
would
with
poorly
placebo-controlled
little
or no difference
demonstrated
for example,
between
patients
correlate
symptom
control
between
placebo
serum
concentrations
>10 pg/ml
Dyspnea
studies’5
and by considerable
clinical
experience
by
many clinicians
over the past ten years.
It appears
that
to some extent
efforts
to promote
a wider
therapeutic
range,
ie, 5 to 20 pg/ml,
have been
motivated
by drug
carefully
in
bronchodilatation
Asthma
The
alone
severity
ticularly
COPD.
toxicity
with
ophylline
of symptoms
with an oral
agonist
studies
demonstrating
Sputum
Walkung
pain the
Feeling
FIGURE
1. Mean
symptom
scores
from
patients
with
COPD who
received
placebo
and individualized
oral doses of theophylline,
each
for one month,
in a double-blind,
cross-over
manner.
(Reproduced
with permission
of Journal
of American
Medical Association.’)
Recent
Advances
in Management
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
of Obstructive
AirWayS
Disease
work
of breathing,
found
a modest
lung
work,
particularly
increase
and
theophylline
slight
during
in FEy,,
subjective
at a mean
exercise.
a small
They
decrease
improvement
concentration
improvement
work.
Patients
ferred
in this
theophylline
study
of
COPD
did not alter
theophylline
there
where
in the
that
overall
effects
management
diaphragmatic
correpre-
20
treating
or
with
COPD,
respiratory
are no
preventing
but there
support
this conjecture.
Since
theophylline
particularly
in COPD
disease.
work
some
of
stimulabenefit
in
failure
controlled
associated
studies
toxic
drug,3#{176}
may be more
effects3’
and
concentrations
result
of impaired
the small
potential
from cor pulmonale,
be weighed
against
must
at risk of
as a
the potential
greater
caution
risk of toxicity.
If it is used
in COPD,
must be exercised
to prevent
accumu-
lation
serum
of toxic
concentrations.
In such
it might
be prudent
to maintain
at the lower
end of the therapeutic
FIGURE
2.
average
coated
child
tablets
is rapidly,
from
oral
the
patients,
and
and
plain,
com-
doses,
release
rapid-release
fluctuations
particularly
products
mulated
in
disintegration
formulations
in
serum
in
have
various
ways
and dissolution
can
result
to
in
between
absorbed
products,
absorption
may
ences
in serum
result
in
concentration
However,
dosing
if the
8
9
is either
relatively
interval
on Absorption:
and
pathology
release
erratic,
The
influence
on the
Food
absorption
markedly
(a bead-filled
capsule
with pH-independent
given to children
8 to 12 years old,
but
important
Theo-bid,
data).
effect
absorbed
bioavailability
the
the
from
on
Somophyllin-CRT,
In contrast,
food
amounts
that,
on
Theo-Dur
excessive
serum
or
results
concentrations
is appropriate
for
coating
rapidly
at 7.4 to 8.0,
after a meal.4’
Food
the
of
absorption
Uniphyl,
appears
from
71
a
clinical
dissolves
of toxicity,
taken with
much
24-hour
incompletely
effect
product
that,
absorbed
dissoluis pH-
at pH
on
6.8
but
rate
from
like Theo-24,
when
taken
fasting.41
CHEST
I 88 / 2 I AUGUST,
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
1985 / Supplement
a
with
a
dose was
3). Apparently,
Theo-24
beads
slowly
no
In
the pH range of the small intestine
also appears
to increase
the extent
without
another
to be
only
and
(Fig
the
of
Sb-Bid
in dump-
of theophylline
average,
is
most severe
symptoms
after a single dose
taken
fasting
coating
on
the
tab-
was taken with food but had
the dose was taken
fasting.39
subject
with the
peak concentration
dependent;
has
Theo-Dur
when
taken
fasting.3#{176}39 During
study,
four of eight
volunteers
when
Theo-24
effects
when
the
of
bio-
formulations
evaluated.
Sprinkle
dissolution)
clinically
be
serum
levels
patients.3#{176}’4’
theophylline
adequately
of
can
incomplete,
constant
in most
previously
tion
of
rates
12
range
around
the
from the so-called
decrease
the
rate
of
of the drug.
However,
in
11
rate
generally
was 31.4 compared
the same 1,500-mg
differences
10
elimination
the therapeutic
of theophylline
of slow
been
and
bacon
and eggs breakfast
peak of 12.5 g/ml
when
clinically
important
differfluctuations3#{176}37 (Fig 2).
interval
7
metabolizers,3#{176}37
slowpopular.
They
are for-
extent
and,
particularly,
rate
of absorption
differ
among
the 29 brands
of the 15 slow-release
formulations available
in this country.
Even among
completely
6
product
of Food
physiology,
developed
rectal
supabsorbed.3#{176}
5
concentrations
ing of potentially
toxic
Theo-24,3#{176} a product
uncoated
concentrations
rapid
become
qt2t,
9128
theophylline
toxicity
adverse
Because
10mg/kg
10.9mg/kg
impairs
tions are
positories
but
of the
serum
formulations
not
percent
recent
nearly
completely
absorbed,
are erratically
and incompletely
4
3
or too rapid to achieve
over a 24-hour
dosing
tablets,
while
enteric
coating
(eg, Choledyl)
delays
dissolution,
which
can result
in incomplete
absorption
and/or
unpredictable
absorption
rates.’5
Rectal
solu-
large
rate
patient,
once-daily
no
consistently,
2
maintained
within
clock. #{176}Absorption
has
serum
concentrations
range.
liquids
Oyrocaps.
9121,
9128
12.3mg/kg
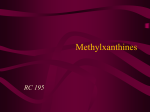
Predicted
steady-state
serum
concentrations
for an
(ti/I = 3.7 hours;
V = 422 mI/kg)
receiving
plain,
Unand four
slow-release
products
at 12-hour
dosing
intervals.
The
more
rapid
the rate of absorption,
the greater
the
fluctuation
and the longer
the amount
of time the serum
concentration remains
in the subtherapeutic
range
(less
than
10 g/ml).
(Reproduced
by permission
of Pharmacotherapy.5t)
lets,aL
(unpublished
absorbed
1
availability
Absorption
Theophylline
StoghylIk,
0128
128mg/kg
Time (hours)
Influence
age,
GI
PHARMACOKINETICS
pletely
o
0
absorption
to
sensitive
to its arrythmogenic
accumulating
excessive
serum
metabolism
benefit
PhYSOCOntIn.
of
are clinically
and
is a potentially
patients,
who
S
#{163}
debut
effects
patients,
of this
performance,”
might
offer
-
8.2mg/kg
200&300,
airways
contractility,’4
breathing,4
biventricular
tion of hypoxic
drive’6
Thso-Dur
#{149}
PWafl Tiblit.,
altered
the
In another
Thus,
in COPD
these
O
double-blind
reversible
exercise
performance.5
can be demonstrated
on
25
carefully
excluded,
theophylline
to a small and significant
degree
is no evidence
important
Effects
placebo
that theophylline
was not excluded.
patients,
obstruction
was
creased
dyspnea
but
over
the possibility
of dyspnea
30
but
of 12 .ig/ml,
-
Serum Theophyiiine
(pg/mi)
during
neither
spirometric
nor subjective
lated
with
the decrease
in lung
study,
but
perception
in
105S
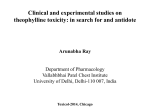
Subject
VA
30
Nausea.
Vomiting
Headache
25
Fasting
After
Serum
Theophyihne
Concentration
rates
which
Breakfast
20
8
16
24
32
Time
40
48
serum
concentrations
in an individual
subject
after a single 1,500mg
dose ofTheo-24
taken fasting
and after
breakfast.
Shaded
area indicates
the period
during
which patient
experienced
nausea,
repeated
vomiting,
or severe, throbbing
headache.
The pattern
of drug release
during
the food regimen
is
consistent
with
“dose-dumping.”
(Reproduced
with permission
of
Chest.
Food decreases
the
from Theolair-SR,
rate, but
a product
tion
dissolution,
in
significantly
increase
from
children
Theolair-SR
or Slo-Phyllin
from products
not extent,
with pH
and
adults.47
the
rate
of theophylline
but
not from
also
absorp-
Theo-Dur
tablets
Gyrocaps.49
Theoretically,
absorption
with pH-dependent
dissolution
may be
the effect
of food
and
pH
characteristics
of slow-release
may
alter
products
unaffected
should
by Ibod
be considered
and
other
factors
for routine
as
use.
theophylline
enters
the
systemic
on average
40 percent
becomes
protein
and
the
remaining
free
throughout
ing reported
elevated
due
theophylline
both children
a single
by the volume
after
to the
to plasma
distributes
lower
temperature
binding
increased
apparwhich
averages
0.5 IJkg
among
Since the peak concentration
distributes,
and adults.
loading
dose
of distribution,
concentration,
and
during
in vitro testing.3#{176}The
distribution,
the
space
into
on
volume
of distribution
and hepatic
cirrhosis,
protein
circulation,
bound
drug
body water.
The 60 percent
protein
bindin previous
studies
was artifactually
pH that occurred
ent volume
of
serum
the
is equal
to the dose divided
1 mg/kg will increase
the
average,
2 g/ml.
The
during
uncorrected
is slightly
larger,
acisince
is reduced
in these
is eliminated
from
by
Elimination
Theophylline
at variable
individuals
occurs
as a result
body.
Interpatient
ing
concurrent
reports
have
been
normal-weight
diac
thyroid
published
in
to differences
that change
function,
on
smokConflict-
the
subjects
or between
influence
and
men
and
require
a major
However,
the
or stable
COPD
reduced.
the
fever
cause
event,
warrant
cine
ance,
is the
or the
the magnitude
a temporary
viral
of the
dosage
during
febrile
it is unclear
if
infection.
effect can
reduction.
In either
be sufficient
Influenza
was also thought
to reduce
theophylline
but several
subsequent
well-controlled
Cigarette
ance
on
achieve
the
demonstrate
any
therapeutic
serum
among
than
have rapid
clearlarger
doses
to
hepatic
of theophylline,
metabolism
in part
Changes
protein
alter
persistent
eater
clearance,
alterations
Recent
Advances
even
but
the
magnitude
of
to require
changes
in
except
when
radical
in diet
occur,
eg,
a heavy
a high-carbohydrate
vegetarian.
in Management
Airways
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
in
in theophylline
clearof dietary
carbohydrate
and is unlikely
for individuals
becoming
increased
but
there
is a correlation
clearance,
suggesting
in thyroid
function
con-
to the variability
in the amount
can
from
thyrotoxicosis,
euthyroid
asthmatic
patients,
between
T4 and theophylline
that interpatient
differences
non-
is more
rapid than
in adolescents
increases
the
presumably
during
than
clearance
More
average
clearance
has also been
found
with cystic
fibrosis.3#{176} Hyperthyroidism
clearance
important
concentrations
the elderly,
in nonsmokers.
to
vac-
clearstudies
clinically
and marijuana
smokers
average3#{176} and
require
smokers.
Even
rapid in smokers
meat
be quite
to prevent
in patients
with
cor pulmonale3’
clearance
is reduced
tract
infections,3#{176} but
and
women.3’
can
decrease
clearance
without
of
clearis no
and
clearance
hepatitis,
car-
cor pulmonale
dosage
Theophylline
viral respiratory
tribute
ance,
and
the decrease
in theophylline
with hepatic
cirrhosis,
acute
decompensation,
large
of
variability
ing, aberrations
in diet, and other
drugs.5’
Effects
of Disease
and Altered
Physiology:
and
the body
P-450
dosage
illness,
age,
un-
the cytochrome
Variability
of
with
change
is not large
dose requirements
patients.5’
by
liver.
kidneys
to rela-
appears
to be due
biotransformation
have failed
to
interaction.3#{176}
Distribution
Once
metabolites
in the
the
is metabolized
clearance
is large and
in the rate of hepatic
is not
the
dif-
such
clinical
by
remainder
some
of
Approx-
rates of elimination.
Total body clearance,
of volume
of distribution
and elimination
most
accurately
reflects
theophylline
toxic reaction.
cholestasis52
ferently,
since product
formulation
design
and rates of
absorption
vary.
Studies
are needed
to define
these
effects
on most
slow-release
products.
Clearly,
only
products
is eliminated
the
from
In contrast,
associated
more
rapid
in patients
with less acid gastric
contents,
such as the elderly,
or during
concurrent
administration of H2-receptor
antagonists.
Thus,
absorption
parallel
pathways,
capacity-limited.
obesity,
old age, and gender
on theophylline
ance.
Available
evidence
suggests
that
there
clinically
important
difference
between
obese
of absorpdependent
Antacids
or
among
removal
56
(houra)
3. Theophylline
FIGURE
106$
while
the variable
the product
rate constant,
0
mean
demia
10 percent
requirements
5
pH
imately
changed,
tively
inactive
enzyme
system
(pg/mi)
tion
through
multiple
are saturable
of Obstructive
Disease
patients,
the
before
total
serum
guide
final
tration
range,
dose
level
should
not
exceed
measurements
dosage,
and
the
should
be at the
eg, 10 g/ml.
400
are
final
target
lower
end
phylline.
mg/day
obtained
serum
of the
to
14
J
Eur
Murciano
D,
theophylline
concen-
with
therapeutic
Respir
on
chronic
OF
THEOPHYLLINE
Matthay
obstructive
RA,
chronic
CONCENTRATION
As
a result
of
physician
methodology,
ophylline
communities
in serum
are now
in the United
pensive
are
office
rapid,
facilities
methods
specific,
serum
or blood
have
immunoassay
by Ames
on a plastic
strip
measured
in
Another
method
thein most
inex-
of measuring
theophylline
that
require
small
very
recently
utilizes
a colormetric
by
amounts
indicator
photometer
Syntex
HJ,
MR.
structive
line:
of
that
pulmonary
ML,
Efficacy
tion.
Ann
3 Eaton
disease
with
Effects
BA,
Intern
Med
1980;
patients
orally
administered
JAMA
TR,
McGowan
chronic
19
20
a
JW,
Siever
effect
and
22
5 Mahler
JR.
DA,
obstruction.
6 Bergstrand
H.
Respir
7 Horrobin
BA,
23
DE.
MS.
CR,
coupling
of action
muscle.
Sharp
JT
work
standing
Lunell
CK,
J.
Loke
Sus-
of
MJ,
Respir
Dis
1985;
DJ,
and
Effects
Med
1978;
in
65:903-
of aminophylline
Am
Rev
5, West
Respir
RO.
on
Dis
1978;
Hemodynamic
obstructive
of theophylline
et al, eds.
MM,
pulmonary
on mucociliary
Sustained
release
Amsterdam:
Bronsky
in asthmatic
Pollock
J,
serum
theophylline
Hambleton
dis-
transport.
theophylline
Excerpta
Evaluation
J
F, Cooper
in
Medica,
G,
1984:
and
theophylline
1977;
J Med
Pedi-
Cavanaugh
M,
of cromoglycate
symptoms
M, Thompson
1981;
of chronic
R, Huntley
in
W. The
steroid-dependent
value
asthma.
304:71-75
L, Green
M,
of orally
in the
J,
Taylor
of
exercise-
cromolyn.
Comparison
in controlling
theophylline
Dusdieker
of
1:381-85
Weinberger
maintenance
Relationship
inhibition
with
M,
S. et al.
bronchodilaror
84:421-27
M.
to
comparison
Weinberger
Lancet
1974;
D, Weinberger
and
Godfrey
of oral
Pediatr
concentration
E,
NassifEC,
EA.
children.
Kiechel
26
theophylline.
27
P Methylxanthine
as
mesenteric
prostaglandin
artery
Smith
GD,
Ekwo
administered
control
Pros-
preparation.
WJ. The
insulin
stimulus-secre-
release.
3’5’-cycic
JG,
cAMP
Smith
VII.
EE,
Weinberger
metaproterenol
of chronic
J
Clin
29
Pharmacol
Effect
protein
1979;
AE,
on
tracheal
30
J
asthma.
M.
and
Pediatr
Am
N, Andersson
a xanthine
with
mediator
J
Allergy
KE,
FER,
for treatment
Rev
31
Adenosine-induced
Respir
Dis
1984;
theo-
1982;
101:
M,
KE,
lacking
chronic
adenosine
obstructive
in asthma
Clin
Persson
CC.
its
CGA.
receptor
lung
MJ.
and
Immunol
Persson
Adenosine
antagonism
Effects
Tabachnik
E, Scott
Sustained
L, Bighley
L,
Frequent
toxicity
AL.
disease.
Eur
J
Clin
by
methylxan-
effects
of theo-
Rev
effect
34
Pediatr
Dis
JL,
1979;
theo-
1982;
C, et
in the
100:489-92
CD,
infusions
Intell
11:1218
Clin
of
Rozea
P,
oral
salbutamol
Dis
Pharm
1977;
drug
tolerance
to
Carin
beta,
73:949-57
1976;
Bandler
T. Multifocal
Lancet
Ludden
L,
Theobald
C,
in exercise-induced
114:493-500
Guarnieri
of theophylline.
clearance
5, Lewth
advance
JP,
JR,
McNay
A, MacLeod
a significant
and
Respir
Michael
Isles
J
and
Richardson
RH,
Hepler
from IV aminophylline
1978;
Seale
Inhaled
Am
N,
J
Am
17:585-92
development
Chest
SD,
DA.
Vicuna
TM,
in patients
with
atrial
1985;
1:12-13
Schwertner
H.
tachycarImpaired
cor pulmonale.
J Clin
Br
7:33-37
Weinberger
M,
formulation
to absorption
1978;
as a bronchocon-
1984; 74:302-06
Extrapulmonary
33
Drug
The
agents.
Anderson
J,
asthma.
ill patients.
a toxic
theo-
children.
of ephedrine
1975;
theophylline:
of childhood
JH,
Clin
Sustained-release
Interaction
P, Correia
Hendeles
michael
Plummer
asthma
of erythromycin.
KJ.
J.
P. Guidicelli
in bronchial
in preschool
Ther
release
J.
influence
Simons
E.
treatment
Pharmacol
antagonism,
GH,
Pharmacol
theophylline
of
flow
of asthma
Bronsky
Clin
Levine
C, Duroux
ventilatory
136:790-93
Weinberger
dia:
129:
Luciuk
1982;
asthma.
ST
H, Thuillez
and
airflow
obstruction:
Ther
1982; 31:579-86
phylline
Lindsay
smooth
28:3687-88
Holgate
in asthma.
of theophylline
from
M, Bah
kinetics
critically
A proposed
monophosphate.
TB.
to soluble
‘Ikttersfield
Svedmyr
C, Mathieu
Simons
al.
antag28
F, Malaisse
Richer
phylline.
Hamet
behave
1982; 22:395-402
ST, Mann
JS, Cushley
strictor
110$
J
JV. Effect
man.
DiGiorgi
of CRAO.
Weinberger
Child
131:22-25
32
E,
Pharmacol
Holgate
Andersson
treatment
adrenergic
Niedzwicki
Biochem
in patients
13
25
in non-reversible
51:232-41
enprofylline,
thine.
BL.
35:365-72
effect
JGH,
and chronic
Pharmacol
and
380-84
12
The
Theophylline
109):37-44
Franks
adenosine
bronchoconstriction
11
24
in
13:33-40
fur
binding
Cushley
Wells
dyspnea
Rev
of glucose-induced
1972;
while
inhibition
Malaisse-Lagae
site
RP,
rat
SM,
on lung
disease
PE,
61(suppl
a perfused
tion
Miech
Am
inhibitors
1977;
JV, Cohen
reduces
1980;
Manku
DF,
in
Invest
10
SW.
phylline
1982;
130:600-05
Phosphodiesterase
phosphodiesterase
the
1984;
performance
Am
in chronic
1967;
Comparison
tolerance
Chest
therapy
Snyder
disease.
Dis
taglandins
Solano
pulmonary
Dis 1984;
theophylline
airway
8 Brisson
WS,
theophylline
Matthay
obstructive
onists
Druz
obstructive
Rev Respir
tained-release
9
Clarke
of
obstruc-
exercise
PB,
Circulation
asthma.
T, Nieuuehner
Niewoehner
Ashekian
(cromolyn)
244:2286-90
airflow
JO,
of aminophylline
Cinchansky
ob-
theophyl-
1980;
TR,
airflow
of maintenance
severe
chronic
walking.
Am
J
Med
281-87
4 Jenne
Eur
J
A, Zaret
ventricular
disease.
SA, Weil
induced
bronchospasm
atrics
1977; 60:840-44
82:538-42
The
left
in normal
effects
N EngI
Church
on breathlessness
with
of
22-25
re-
of chronic
5, Sahn
Parker
the
92:758-61
FM,
of theophylline
Treatment
in “irreversible”
MacDonald
Effects
in patients
N Engl
Gottschalk
and
pulmonary
responses
therapy
Diagnostics
study,
Church
of theophylline
ML,
JE.
controlled
Green
DE.
18
21
Kasik
obstructive
In: Jonkman
is
can be performed
on only
from a finger
stick.
WL,
a double-blind,
2 Eaton
in
Dull
B.
fatigue
disease,
J,
Loke
right
upon
Lakshminarayan
ease.
REFERENCES
1 Alexander
and
117:33-38
17
(Seralyzer).
Medical
and
blood
strength
pulmonary
Berger
ventilatory
become
available.
An
a dry reagent
contained
reflectance
quires
no instrument
12 j.il-dmp
of whole
for
readily
States.
16
and
measuring
with
a
demand
available
In addition,
and
109):17-28
Y, Pariente
10
increased
improved
61(suppl
311:349-53
15
MEASURING
1980;
Lecocguic
M,
diaphragmatic
of aminophylline
METHODS
Dis
Aubier
Hendeles
L, Bighley
of oral
L. The
relation
theophylline.
of product
N Engl
J
Med
299:852-57
Hendeles
L,
lafrate
macokinetic
basis
theophylline
products.
Recent
P. Weinberger
for
Advances
the
Clin
selection
Pharmacokinet
In Management
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
M.
and
A clinical
use
of
1984;
of Obstructive
and
slow
pharrelease
9:95-135
Airways
Disease
reports
as
drugs
ophylline;
but
interactions
that
potentially
well-controlled
have
not
studies
been
of
a
with
on these
reported
in the
Table 2-Predicted
During
a 12-Hour
the-
alleged
literature.
theophylline
Fluctuationt
product,
dose,
..
and
tV=
Manufacturer
Plain
or maintenance
prophylactic
therapy
for chronic
asthma,
the absorption
characteristics
of the formulation,
and the rate of elimination
of the drug
in the
individual
patient.
For the treatment
toms
in the patient
with
intermittent
inhaled
13 agonist
such
as terbutaline
provides
greater
bronchodilation
fects than theophylline.3#{176} However,
is required,
the most
an intravenous
rapid and ensured
between
formulations,
and
interchangeably.3#{176}
To
benefit
achieve
from
the
various
rapid
generally
these
products
the
greatest
theophylline
concentrations
should
be
20 jig/ml
therapeutic
width
of the therapeutic
range
concentration
cent
(% Fluctuation
oral
within
the
must
be less
than
10 to
the
peak
function
elimination
of the
rate
100 per-
within
this
Fluctuations
rate
of the product,
from the patient,
absorption
of theophylline
range,
even
in
concentration
vals (Table
clinically
important
fluctuations
2). However,
elimination,
such
differences
when
among
as most
if
are
by the
differdo not
in
serum
interrapid
children,
the
a
the
and
given at 12-hour
patients
with
average
ciga-
rette
or marijuana
smoker,
and about
25 percent
of
nonsmoking
adults,
most
products
are absorbed
too
rapidly
to be given
routinely
twice
daily
without
excessive
serum
concentration
All but two of these products
hours
to avoid
tional
claims
Recently,
excessive
fluctuations,
to the contrary.3#{176}
the FDA approved
Theo-24,
Theo-Dur
tablets
for once-a-day
ever,
none
of these
products
108S
fluctuations
must be given
(Table
2).
every eight
despite
Uniphyl,
promo-
465
125
230
73
130
47
Theobid
140
54
Theovent-LA
167
60
43
18
155
57
S-R
Gyrocaps
Somophyllin-CRT
SR
Elixophyllin
Rorer
Sb-bid
Slow-release
Gyrocaps
tablets
Cord
Laboratories
Constant-T
Key Pharmaceuticals
Theo-Dur
Mead
Theo-Dur
Quibron
Johnson
200, 300
100
T/SR
39
17
88
35
128
48
Mundipharma
Phyllocontin
165
58
Norwich-Eaton
LaBID
252
77
Parke-Davis
Choledyl
154
57
Biker
Theolair
1221:
471:
theophylline,
see
*For
a comprehensive
SA
SR
tPercent
fluctuation
serum
concentration
and
the
average
indicate
the
values
The
has
for the average
child.
that
peak
and
1:Prediction
taken with
when
p.g/ml
methodology
dosing,
with
of the
even
bid.,
derivation
of the
once-a-day
tuations
mean
averaged
half-life
of
then
12-hour
of these
previously.’37
food,
rate
Fluctuations
of this product
of absorption
concentrations
range
around
unless
and
if peak
are
or
may be smaller
is pH dependent,
the
within
the
the clock
labeling,
serum
in Management
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
of
than
ten
the FDA
196 percent
about
seven
Advances
10 to 20
in most
from
Theo-24394’
by food. Absorption
half-life
if
is slowed.
from Theo-Dur,
a 100 percent
or without
food,45
is too rapid
administration.
Howis capable
of reliably
than
maintaining
intervals
for
are
of 100
be more
range,
validation
adult
in excess
with
8-hour
claims
patient
variable,
is greater
multiple-dose
study on which
Recent
ex-
respectively.
will
therapeutic
attained;
and
described
hr),
compatible
and
absorption
is markedly
affected
theophylline
product
with
somewhat
smoking
concentrations
the
are
(7.7
Fluctuations
not
for dose
taken
fasting.
food, since dissolution
taken
#{247}
trough
may
cigarette
of advertising
maintaining
serum
jag/ml
therapeutic
patients,
Uniphyl4’
serum
therefore
within
as 20
been
adult
average
regardless
intervals.
concentration
fluctuations
nonsmoking
concentrations
advisable,
serum
actual
for the
trough
as high
a-day
slow-release
because
of circadian
variation
in absorption.
Half
(t#{189})
are the medians
for the average
child (3.7
to those
serum
and
x 100;
fluctuations
percent
levels
of
peak-trough
=
predictions
of elimination
twice
review
34.
similar
jig/ml.
hr
Theophyl-SR
Aerolate
Laboratories
Predicted
as 20
Theophyl,
Bronkodyl
K-V Laboratories
hr)
100)
the
length
of the dosing
interval
selected
physician.37
In patients
with slow elimination,
ences
in rates of absorption
between
products
result
Graham
ceed
lives
concentrations
is as high
Laboratories
reference
Trough
to maintain
7.7
Resbid
=
Peak_Trough
hr
Theolair
(IV) fordelivery
around
the clock. Since the
range
is only 10 jig/ml,
serum
fluctuations
Slo-Phyllin,
Slo-Phyllin
can be used
tY2=
3.7
Name
capsules
Cord
of maximum
asthma,
serum
maintained
&
Riker
Bead-filled
side efaddition
release
likelihood
for chronic
Johnson
Johnson,
of acute
sympasthma,
an
or albuterol
with
fewer
when
the
Brand
tablets
Rorer,
of medication,
but plain,
uncoated
or chewable
tablets,
liquids
or liquid-filled
capsules,
and rectal
solutions
(but not suppositories)
may also be satisfactory.
There
are no clinically
important
differences
in rates
of
absorption
in Serum
Concentrations
with Selected
Slow-release
Products*
SELECTION
dosing
interval
must
be based
on the specific
clinical
indication,
ie, treatment
of acute
asthmatic
symptoms
of theophylline
mulation
provides
Fluctuations
Dose interval
Theophylline
%
PRODUCT
Selection
interact
and
of
absorbed
for once-
elimination,
hours.
based
concentration
in volunteers
hours,
but
of Obstructive
a
In the
approval
flucwith
a
only
46
Airways
Disease
Adults
and
children
over
1 year
INITIAL
DOSE
old:
The leser
after
FIRST
Adults
and
Children
of 400
or 16 mg/kglday
3 days
INCREMENTAL
children
45 kg:
mglday
INCREASE
5 45 kg:
The lesser
600mg/day
of 600 mg/day
20 mg/kg/day
for ages
16mg/kg/day
for ages9
after
or--
ff0
9
3 days
+
Adults
Children
SECOND
INCREMENTAL
and children
545 kg:
<
45 kg: The lesser
INCREASE
800mg
of 800 mg/day
24 mg/kg/day
1 to 9
for ages 9fo 12
for ages 12 to 16
20 mg/kg/day
18 mg/kg/day
Check
serum
concentration
have been
or--
for ages
about
4 hourS
missed
or added
after a dose
for 3 days
when
none
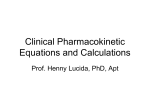
4.
Scheme
for establishing
optheophylline
dosage
in ambulatory
patients
to prevent
transient
caffeine-like
side effects.
This
is a conservative
application
of the recommendations
incorporated
into
the
FDA-approved
package
insert.
Ideal body weight
should
be used
for obese
patients.
In
patients
with
cardiac
decompensation,
cor pulmonale,
or liver dysfunction
or in
those
taking
drugs
such
as cimetidine
that
markedly
impair
metabolism,
the
initial
dose before
a serum
concentration
measurement
is obtained
should
not exceed 400 mg/day.
(Reproduced
by permission
of the New
England
Journal
of
FIGURE
timal
SERUM
CONCENTRATION
DIRECTIONS
10 to 20 xg/ml
Maintain
dose
CONCENTRATION
20 to 25 y.g/ml
25 to 30 1Lg/mI
Over 30 g/ml
Decrease
Skip next
Skip next
RECHECK
FURTHER
7.5 to 10 p.g/ml
Below 7.5 g/ml
Increase
dose about
25% it tolerated.
Increase
dose about 25%nd
RECHECK
FOR GUIDANCE
IN FURTHER
DOSE
‘Finer adfustmenls
in dosage may be needed
mandate earlier reexamination
it tolerated.
RECHECK
SERUM
THEOPHYLLINE
AT 6 TO 12 MONTH
INTERVALS.
dose at least 10%
dose and decrease
subsequent
doses at least 25%.
2 doses,
decrease
subsequent
doses 50%, and
SERUM
THEOPHYLLINE
FOR GUIDANCE
IN
DOSE
ADJUSTMENT.
for some patients:
drug
inferactions
SERUM
THEOPHYLLINE
ADJUSTMENT.
or physiologic
abnormalities
may
oral
Medicine.tm)
percent
when
the
same
doses.w
In contrast,
the United
States),
when
taken
dose
was
divided
fasting,3#{176}’’4’ will
result
fluctuations
with
once-daily
dosing
nonsmoking
adult,
but higher
doses
because
of incomplete
absorption’39
percent
of the dose)
and,
if taken
ophylline
In one
when
were
toxicity
may
study,
Uniphyl
taken
fasting,
absorbed
when
appears
from
hour products
to slow
but
the
these
with
absorption
into
Theo-24
(Pulmo-’flmelets
an ultraslowly
absorbed
in
result
from dose dumping.396#{176}
was only 55 percent
absorbed
substantially
larger
dose was taken with
and other
ultra-slow
sufficiently
tion
with
will
current
absence
frequency
relatively
be available
technical
of
constant
amounts
food.4’ It
Variations
quently,
for once daily
limitations
of the
dosing.
products
data
documenting
that
of dosing
from
twice-a-day
absorpWith
and
the
the
decreasing
the
to once-a-day
guide
Unless
a
clearance
of theophylline
among
must be low to circumvent
transient
caffeine-like
sideeffects
(eg, 400 mg fur otherwise
healthy
adults)
and
slowly
titrated
over a period
of nine days to average
to minimize
fluctuations
in the
individuals
result
in large differences
in dosage
requirements
to maintain
serum
concentrations
within
the 10 to 20 p.g/ml
therapeutic
range.
Initial
dosage
requirements
concurrent
complete
dosing
appears
to be
than
an advance
in
DOSAGE
data on experimental
24absorption
that attempts
and
once-a-day
gimmick
acceptable
in the average
will be needed
(on average,
71
with
food,
the-
during
24-hour
dosing
generally
result
in incomplete
absorption
proportional
to the
degree
of slowing.
Thus,
innovative
technology
will be needed
before
product
improves
compliance,
more
of a marketing
formulation
technology.
12-hr
outside
product
according
physiologic
serum
to age and
abnormalities
concentrations
should
the final dosage
adjustments
this
slow
titration
process
frequency
In patients
the presence
of
(Fig 4). Subsebe
obtained
to
(bottom
of Fig 4).
is followed,
the
of adverse
effects
will be unacceptably
with cardiac
failure,
liver dysfunction
high.
or cor
pulmonale,
where
theophylline
clearance
may fluctuate, alternative
therapy
with
other
safer
drugs,
eg,
inhaled
13 agonists,
should
be selected
for maintenance
therapy.
If theophylline
use cannot
be avoided
in such
CHEST
/ 88 / 2 / AUGUST,
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
1985
I Supplement
109S
patients,
the
before
total
serum
guide
final
tration
range,
dose
level
should
not
exceed
measurements
dosage,
and
the
should
be at the
eg, 10 g/ml.
400
are
final
target
lower
end
phylline.
mg/day
obtained
serum
of the
to
14
J
Eur
Murciano
D,
theophylline
concen-
with
therapeutic
Respir
on
chronic
OF
THEOPHYLLINE
Matthay
obstructive
RA,
chronic
CONCENTRATION
As
a result
of
physician
methodology,
ophylline
communities
in serum
are now
in the United
pensive
are
office
rapid,
facilities
methods
specific,
serum
or blood
have
immunoassay
by Ames
on a plastic
strip
measured
in
Another
method
thein most
inex-
of measuring
theophylline
that
require
small
very
recently
utilizes
a colormetric
by
amounts
indicator
photometer
Syntex
HJ,
MR.
structive
line:
of
that
pulmonary
ML,
Efficacy
tion.
Ann
3 Eaton
disease
with
Effects
BA,
Intern
Med
1980;
patients
orally
administered
JAMA
TR,
McGowan
chronic
19
20
a
JW,
Siever
effect
and
22
5 Mahler
JR.
DA,
obstruction.
6 Bergstrand
H.
Respir
7 Horrobin
BA,
23
DE.
MS.
CR,
coupling
of action
muscle.
Sharp
JT
work
standing
Lunell
CK,
J.
Loke
Sus-
of
MJ,
Respir
Dis
1985;
DJ,
and
Effects
Med
1978;
in
65:903-
of aminophylline
Am
Rev
5, West
Respir
RO.
on
Dis
1978;
Hemodynamic
obstructive
of theophylline
et al, eds.
MM,
pulmonary
on mucociliary
Sustained
release
Amsterdam:
Bronsky
in asthmatic
Pollock
J,
serum
theophylline
Hambleton
dis-
transport.
theophylline
Excerpta
Evaluation
J
F, Cooper
in
Medica,
G,
1984:
and
theophylline
1977;
J Med
Pedi-
Cavanaugh
M,
of cromoglycate
symptoms
M, Thompson
1981;
of chronic
R, Huntley
in
W. The
steroid-dependent
value
asthma.
304:71-75
L, Green
M,
of orally
in the
J,
Taylor
of
exercise-
cromolyn.
Comparison
in controlling
theophylline
Dusdieker
of
1:381-85
Weinberger
maintenance
Relationship
inhibition
with
M,
S. et al.
bronchodilaror
84:421-27
M.
to
comparison
Weinberger
Lancet
1974;
D, Weinberger
and
Godfrey
of oral
Pediatr
concentration
E,
NassifEC,
EA.
children.
Kiechel
26
theophylline.
27
P Methylxanthine
as
mesenteric
prostaglandin
artery
Smith
GD,
Ekwo
administered
control
Pros-
preparation.
WJ. The
insulin
stimulus-secre-
release.
3’5’-cycic
JG,
cAMP
Smith
VII.
EE,
Weinberger
metaproterenol
of chronic
J
Clin
29
Pharmacol
Effect
protein
1979;
AE,
on
tracheal
30
J
asthma.
M.
and
Pediatr
Am
N, Andersson
a xanthine
with
mediator
J
Allergy
KE,
FER,
for treatment
Rev
31
Adenosine-induced
Respir
Dis
1984;
theo-
1982;
101:
M,
KE,
lacking
chronic
adenosine
obstructive
in asthma
Clin
Persson
CC.
its
CGA.
receptor
lung
MJ.
and
Immunol
Persson
Adenosine
antagonism
Effects
Tabachnik
E, Scott
Sustained
L, Bighley
L,
Frequent
toxicity
AL.
disease.
Eur
J
Clin
by
methylxan-
effects
of theo-
Rev
effect
34
Pediatr
Dis
JL,
1979;
theo-
1982;
C, et
in the
100:489-92
CD,
infusions
Intell
11:1218
Clin
of
Rozea
P,
oral
salbutamol
Dis
Pharm
1977;
drug
tolerance
to
Carin
beta,
73:949-57
1976;
Bandler
T. Multifocal
Lancet
Ludden
L,
Theobald
C,
in exercise-induced
114:493-500
Guarnieri
of theophylline.
clearance
5, Lewth
advance
JP,
JR,
McNay
A, MacLeod
a significant
and
Respir
Michael
Isles
J
and
Richardson
RH,
Hepler
from IV aminophylline
1978;
Seale
Inhaled
Am
N,
J
Am
17:585-92
development
Chest
SD,
DA.
Vicuna
TM,
in patients
with
atrial
1985;
1:12-13
Schwertner
H.
tachycarImpaired
cor pulmonale.
J Clin
Br
7:33-37
Weinberger
M,
formulation
to absorption
1978;
as a bronchocon-
1984; 74:302-06
Extrapulmonary
33
Drug
The
agents.
Anderson
J,
asthma.
ill patients.
a toxic
theo-
children.
of ephedrine
1975;
theophylline:
of childhood
JH,
Clin
Sustained-release
Interaction
P, Correia
Hendeles
michael
Plummer
asthma
of erythromycin.
KJ.
J.
P. Guidicelli
in bronchial
in preschool
Ther
release
J.
influence
Simons
E.
treatment
Pharmacol
antagonism,
GH,
Pharmacol
theophylline
of
flow
of asthma
Bronsky
Clin
Levine
C, Duroux
ventilatory
136:790-93
Weinberger
dia:
129:
Luciuk
1982;
asthma.
ST
H, Thuillez
and
airflow
obstruction:
Ther
1982; 31:579-86
phylline
Lindsay
smooth
28:3687-88
Holgate
in asthma.
of theophylline
from
M, Bah
kinetics
critically
A proposed
monophosphate.
TB.
to soluble
‘Ikttersfield
Svedmyr
C, Mathieu
Simons
al.
antag28
F, Malaisse
Richer
phylline.
Hamet
behave
1982; 22:395-402
ST, Mann
JS, Cushley
strictor
110$
J
JV. Effect
man.
DiGiorgi
of CRAO.
Weinberger
Child
131:22-25
32
E,
Pharmacol
Holgate
Andersson
treatment
adrenergic
Niedzwicki
Biochem
in patients
13
25
in non-reversible
51:232-41
enprofylline,
thine.
BL.
35:365-72
effect
JGH,
and chronic
Pharmacol
and
380-84
12
The
Theophylline
109):37-44
Franks
adenosine
bronchoconstriction
11
24
in
13:33-40
fur
binding
Cushley
Wells
dyspnea
Rev
of glucose-induced
1972;
while
inhibition
Malaisse-Lagae
site
RP,
rat
SM,
on lung
disease
PE,
61(suppl
a perfused
tion
Miech
Am
inhibitors
1977;
JV, Cohen
reduces
1980;
Manku
DF,
in
Invest
10
SW.
phylline
1982;
130:600-05
Phosphodiesterase
phosphodiesterase
the
1984;
performance
Am
in chronic
1967;
Comparison
tolerance
Chest
therapy
Snyder
disease.
Dis
taglandins
Solano
pulmonary
Dis 1984;
theophylline
airway
8 Brisson
WS,
theophylline
Matthay
obstructive
onists
Druz
obstructive
Rev Respir
tained-release
9
Clarke
of
obstruc-
exercise
PB,
Circulation
asthma.
T, Nieuuehner
Niewoehner
Ashekian
(cromolyn)
244:2286-90
airflow
JO,
of aminophylline
Cinchansky
ob-
theophyl-
1980;
TR,
airflow
of maintenance
severe
chronic
walking.
Am
J
Med
281-87
4 Jenne
Eur
J
A, Zaret
ventricular
disease.
SA, Weil
induced
bronchospasm
atrics
1977; 60:840-44
82:538-42
The
left
in normal
effects
N EngI
Church
on breathlessness
with
of
22-25
re-
of chronic
5, Sahn
Parker
the
92:758-61
FM,
of theophylline
Treatment
in “irreversible”
MacDonald
Effects
in patients
N Engl
Gottschalk
and
pulmonary
responses
therapy
Diagnostics
study,
Church
of theophylline
ML,
JE.
controlled
Green
DE.
18
21
Kasik
obstructive
In: Jonkman
is
can be performed
on only
from a finger
stick.
WL,
a double-blind,
2 Eaton
in
Dull
B.
fatigue
disease,
J,
Loke
right
upon
Lakshminarayan
ease.
REFERENCES
1 Alexander
and
117:33-38
17
(Seralyzer).
Medical
and
blood
strength
pulmonary
Berger
ventilatory
become
available.
An
a dry reagent
contained
reflectance
quires
no instrument
12 j.il-dmp
of whole
for
readily
States.
16
and
measuring
with
a
demand
available
In addition,
and
109):17-28
Y, Pariente
10
increased
improved
61(suppl
311:349-53
15
MEASURING
1980;
Lecocguic
M,
diaphragmatic
of aminophylline
METHODS
Dis
Aubier
Hendeles
L, Bighley
of oral
L. The
relation
theophylline.
of product
N Engl
J
Med
299:852-57
Hendeles
L,
lafrate
macokinetic
basis
theophylline
products.
Recent
P. Weinberger
for
Advances
the
Clin
selection
Pharmacokinet
In Management
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
M.
and
A clinical
use
of
1984;
of Obstructive
and
slow
pharrelease
9:95-135
Airways
Disease
35
Cinchansky
E,
Pediatr
36
Weinberger
oral
to
clearance
1977;
in
Relationship
children
with
of
theophylline
chronic
asthma.
56
J
57
91:655-60
J, Mirtallo
Dasta
M.
dosage
JM,
sustained-release
Altman
M.
theophylline
obstructive
pulmonary
Comparison
tablets
disease.
in patients
J
Am
of standard
Hosp
Pharm
chronic
1979;
36:613-
A, Spino
cystic
fibrosis.
Vozeh
of
M,
formulation
and
theophylline
Pediatr
38
39
Hendeles
1981;
MM.
report
on 24-hour
lations
with
Administration
1984;
4: 181-98
NH,
and
the
3rd
61
prod-
Baltimore,
Oct
J.
sprinkle
product
P, Purohit
and
Sips
J
Eur
MA,
theophylline
tions
in fasted
1983;
4:63-72
Pedersen
Walter
of
Clin
Kulstad
a slow
Pediatrics
1984;
RB,
DS,
from
enteric
Irwin
coated
non-fasted
and
J.
from
FA,
Dijkman
from
JH.
Theolin
26:405-07
Welling
PG.
Absorption
sustained
subjects.
S, Moller-Pedersen
of theophylline
22:196-200
of theophylline
Pharmacol
on the
a sustained-release
1982;
Patel
and
of food
Effect
of
5, de Wolff
bioavailability
Clin
JB.
release
Pharmacol
PM,
not affect
Osman
tion
J
Edelbroek
Retard.
AA,
pattern
tablet.
AP,
release
Biopharm
Influence
of
lbrmula-
Drug
Dispos
of food on the
absorp-
Somophyllin-CRT
Clin
Allergy
(in
press)
47
Pedersen
5, Moeller-Petersen
tion
and
rate
Myhre
tion
Allergy
KI,
Walstad
of two
different
line.
49
Br
Shargel
J
Clin
Shaw
J
LM,
serum
51
influence
Pharm
Fuchs
Hendeles
1981;
binding.
rapid
of antacid
Effect
and
timed-release
influencing
Pharmacol
M.
Ther
Theophylline:
theophylline
1982;
32:490-96
a “state
of the
1983; 3:2-44
D, Lissner
B, Zilly W, Bombard
Schuppan
E. Pharmacokinetics
with liver diseases.
on
drug
70:599-602
Clin
Pharmacotherapy
StaibAH,
Yu ABC.
K. Factors
L, Weinberger
absorp-
of theophyl-
15:683-87
JE,
from
L, Mayock
on the
formulations
1983;
Sci
absorp-
theophylline
of antacid
sustained-release
JA,
release
37:531-34
The
Pharmacol
Fields
protein
review.
52
1982;
of theophylline
products.
of food on the
Influence
of a sustained
BA.
L, Stevens
bioavailability
50
J.
bioavailability
preparation.
48
art”
G, Richter
and metabolism
of theophylline
in patients
Int J Clin Pharmacol
Ther Toxicol
1980; 18:
500-02
53
KC,
1978;
Lauer
BA,
55
during
JHC,
TD,
acute
Upton
theophylline.
Jusko
Enhanced
tobacco
Bell
Chai
H.
Altered
respiratory
viral
theophylline
illness.
WJ,
BA.
Clin
JJ,
Schentag
Pharmacokinetic
Pharmacokinet
Clark
biotransfbrmation
smokers.
Clin
JH,
drug
1984;
Gardner
of theophylline
Lancet
Pharmacol
Ther
1978;
interactions
9:309-34
M,
Yurchak
AM.
in marihuana
and
24:405-10
of thyroid
1984;
Ther
and
inhaled
Rev
Respir
intervals
L,
DH,
Dis
Meyer
1980;
ML,
Wubbena
of
acute
infused
122:365-71
AB.
dosed
Presented
Academy
Disposition
at 12 and
at the
36th
Pharmaceutical
24
Annual
Sciences,
p 108
P. Weinberger
of once-a-day
McFadden
of the
and
Straughn
theophylline
1984 abstract
JR,
sympathomimetics
[Abstract].
APhA
Snapper
comparison
M.
theophylline
dose
Food-induced
[Letter].
1984;
Lancet
2:
M,
basis
Hendeles
L. Slow-release
for product
selection.
N EngI
theophylline:
ration-
J Med 1983; 308:760-
compared
the tablet fbrm of a beta
agonist such as albuterol
vs oral theophylline?
Dr Hendeles:
There has been a comparison
study with TheoDur
given
every
eight
hours
and Alupent
tablets given every
Has
anybody
hours.
There
were
significant
differences
between
the
two groups fuvoring
the theophylline
regimen,
particularly
when a standardized
exercise
stress test was used as an endpoint. The oral beta adrenergic
agonists were not efficacious
in blocking
exercise-induced
bronchospasm,
whereas
the
inhaled
beta agonists
had a potent
effect even though
the
same degree
of brochodilatation
was obtained
through
both
furmulations.
In other words,
if you raise the FEy1 to the
same point, the inhaled
adrenergic
agonist will block exercise-induced
asthma and the oral form will not, suggesting
that the topical
effect of the beta adrenergic
agonist
is
important.
Theophylline,
with a therapeutic
serum level, has
a reasonably
good effect on exercise-induced
bronchospasm,
but not as good as inhaled
beta adrenergic
agonists.
Audience:
There have been a number
of studies comparing
the cardiovascular
effects
of theophylline
and beta adrenergic agonists.
Usually beta adrenergic
agonists
appear
to
have a bit more potential
for causing cardiac
ectopy.
In your
discussion
on this point, could
you clarify
the experimental
design?
Dr Hendeles:
In the study
which
I cited, there were some
patients
receiving
Digoxin
whose
levels
were
measured
and
were in the therapeutic
range.
Arterial
blood
gas abnormal!ties were not associated
with arrhythmias.
The most important factor
was stopping
or adding
theophylline
to the
therapeutic
regimen.
So theophylline
itself or through
synergy
with other agents may cause cardiac
arrhythmia.
In
patients
with normal
hearts
without
pre-existing
cardiac
arrhythmia,
the combination
of inhaled
beta adrenergic
agonists
with theophylline
in usual clinical
doses
does not
arrhythmia.
It’s
only
when
excessive
doses
are
employed
1:1132-33
Jonkman
with
and
produce
Chang
pharmacokinetics
54
dosing
Weinberger
eight
by food.
caused
Influence
Pharmacol
adrenergic
on
of
in
DIsCussIoN
Trials,
absorption
F
of asthma:
AL,
Uniphylline.
4, 1984
Erratic
disposition
127:417-21
Clin
Goldstein
of controlled-release
May,
64
of the
CA,
Am
of the
study
Clinical
1983;
kinetics.
Golub
Montreal,
85:758-65
Conference
and
Dis
JJ, Follath
Staub
therapy
Meeting
ale
formula-
Annual
Biopharmaceutics
E, et al. Theophylline
Respir
1471
L.
theophylline
Fanta
MA,
Hendeles
dumping
60
Vaughan
1985;
hour
Food and
controlled-release
at
in
Gal
Food does
46
M,
of Theo-dur
Moller-Petersen
theophylline
45
Hill
M,
of parenteral
Audience:
Presented
bioavailability
TH,
Gonzalez
A
Pharmacotherapy
Chest
absorption,
theophylline
Leeds
59
formu-
C. A pharmacokinetic
schedules
qd?
74:534-38
1984;
44
now
to obtain
C,
toxicity.
of Maryland,
5,
release
J
39:634-38
food.
Pedersen
and
Rev
theophylline
aminophylline.
serum
asthma.
theophylline
a “once-a-day”
A, Edwards
Concepts
University
bid
used
Milavetz
from
A. Theophylline
and
of
chronic
Theo-24.
for
M,
dosing
Current
fluctuation
tid,
of data
of theophylline
1984;
Karim
effects
L. Relationship
with
slow-release
approval
B, Cope
tions
43
with
dumping
as a cause
Purkiss
to
qid,
on analyses
L, Weinberger
recommended
42
Theophylline
dosing
Drug
Allergy
41
interval
in children
Otten
Emergency
kinetics
emphasis
Hendeles
L, Vaughan
99:145-52
Weinberger
uct
dosing
concentration
Food-induced
40
L, Wong
Am
on
Rossing
58
ER.
Weinberger
M, lhbachnik
36:634-40
17
37
S,
function
and
with
Isles
that cardiac
arrhythmia
occurs.
Audience:
But my question
was specifically
addressed
as to
whether
or not the threshold
for causing cardiac arrhythmia
was lowered
because
of other drugs they were using.
Dr Hendeles:
It’s entirely
possible that some of them were on
oral terbutaline
or fenoterol
and it is possible
that the effects
were additive.
CHEST
I 88 / 2 / AUGUST,
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21484/ on 04/06/2017
1985
/ Supplement
ills