Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
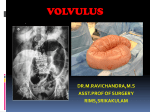
Thamer A. Bin Traiki Definition Volvulus refers to a torsion or twist of an organ on a pedicle. In colonic volvulus : The bowel becomes twisted on its mesenteric axis with partial or complete obstruction & a variable degree of impairment of its blood supply . Cont… Could happen in any portion of large bowel if that segment is attached to a long & floppy mesentery that fixed to the retroperitonium by narrow base . The sigmoid colon is involved in up to 90% of cases, The cecum <20%(this involving Rt colon & TI Cecal volvulus or cecum alone in highly mobile cecum called cecal bascule ) Transverse colon. Incidence Geographical variation . In an unusual report from the high-altitude area of the Bolivian and Peruvian Andes at 13,000 feet above sea level, sigmoid volvulus accounted for 79% of all intestinal obstruction. The reason is not clear but may be related to the increased gas volume in the bowel because of high altitude . Risk Factors Chronic constipation may produce a large, redundant colon (chronic megacolon) Aging average age at presentation being in 7th to 8th decade Neuropsychiatric condition treated with psychotropic drugs High fiber & vegetable Clinically A volvulus may reduce spontaneously, but more commonly produces bowel obstruction (Acute or subacut) , which can progress to strangulation, gangrene, and perforation. The abdomen is markedly distended & tympanic which often more dramatic than in other causes of intestinal obstruction . In case of previous attack resolved spontaneously there will be marked distention with minimal tenderness . Clinical presentation 2 presentations : ‘‘Acute Fulminating type’’ Patient is generally younger , onset is sudden, course is rapid. Generally, there is little history of previous episodes, Symptoms include early vomiting, diffuse abdominal pain and tenderness, marked prostration, and the early appearance of gangrene. Distention may be minimal, In its classic form the acute fulminating variety of sigmoid volvulus produces no distinctive diagnostic signs except for the clinical picture of an acute abdominal catastrophe; The actual diagnosis is made at celiotomy. Ann Surg 1957; 146:52–60 Subacute Progressive Type, The more common presentation. The patient is generally older, onset more gradual, and the early course more benign. There is often a history of previous attacks and chronic constipation. Vomiting occurs late, pain is minimal, Signs of peritonitis are usually not present. Abdominal distention is generally extreme in this form, Radiographic findings are usually diagnostic. Ann Surg 1957; 146:52–60 Radiographic Finding characteristic bent inner tube or coffee bean appearance, with the convexity of the loop lying in the right upper quadrant (opposite the site of obstruction). CT scan reveals characteristic mesenteric whirl sign . Gastrografin enema shows a narrowing at the site of the volvulus and a pathognomonic bird's beak . Treatment Resuscitation Nonoperative Treatment Operative Treatment Nonoperative Treatment Depends on whether the surgeon believes that the bowel is viable or nonviable . Attempt at reduction should be made by means of proctosigmoidoscopy and insertion of a rectal tube. If the volvulus can be reduced, an explosive discharge of gas and feces will occur. The rectal tube should be left in place, either taped or, ideally, sutured to the buttock for about 48 hours to avoid the possibility of immediate recurrence. Proctosigmoidoscopic examination should be undertaken even if the patient has signs and symptoms of nonviable bowel to confirm the extent of involvement and to establish the diagnosis with certainty. ???!!! The procedure should be performed with great care to avoid perforating the bowel. Flexible sigmoidoscopy and colonoscopy It has the advantage of evaluating the viability of a greater area of colonic mucosa. But the procedure must be performed with limited manipulation and limited air to minimize the risk of perforation of the distended and edematous bowel. Intraluminal stenting to prevent early recurrence can be accomplished through the use of flexible plastic tubing or a blunt-ended guide wire . An attempt at colonoscopic reduction may be considered if proctosigmoidoscopic manipulation has been unsuccessful. Cont… Outcomes : More recent studies generally indicate that if the bowel is viable, one may anticipate successful reduction of the volvulus at least 90% of the time. The risk of recurrence is high (40%). For this reason, an elective sigmoid colectomy should be performed after the patient has been stabilized and undergone an adequate bowel preparation. Operative treatment The presence of necrotic mucosa, ulceration, or dark blood noted on endoscopy examination suggests strangulation and is an indication for operation. If dead bowel is present at laparotomy, a sigmoid colectomy with end colostomy (Hartmann procedure) may be the safest operation to perform. Cecal volvulus results from nonfixation of the right colon. Rotation occurs around the ileocolic blood vessels and vascular impairment occurs early. Plain x-rays of the abdomen show a characteristic kidney-shaped, air-filled structure in the left upper quadrant (opposite the site of obstruction), and a Gastrografin enema confirms obstruction at the level of the volvulus Treatment Unlike sigmoid volvulus, cecal volvulus can almost never be detorsed endoscopically. Moreover, because vascular compromise occurs early in the course of cecal volvulus, surgical exploration is necessary when the diagnosis is made. Right hemicolectomy with a primary ileocolic anastomosis can usually be performed safely and prevents recurrence. Simple detorsion or detorsion and cecopexy are associated with a high rate of recurrence. Extremely rare. Nonfixation of the colon and chronic constipation with megacolon may predispose to transverse colon volvulus. The radiographic appearance of transverse colon volvulus resembles sigmoid volvulus, but Gastrografin enema will reveal a more proximal obstruction. Although colonoscopic detorsion is occasionally successful in this setting, most patients require emergent exploration and resection. Thank you