Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
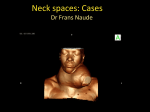
Cervical Nodes: When to Worry and What to do. Donna Sutherland MD, FRCSC CancerCare Manitoba, Head and Neck Surgery University of Manitoba, Department of Otolaryngology Objectives Be familiar with various types of masses that present in the neck Give a differential diagnosis of a neck mass Know the risk factors for Head and Neck cancer Be aware of the historic and clinical features concerning for malignancy Describe the appropriate clinical work-up of a neck mass History Location Onset / Duration Assoc. pain Fluctuation in size Single or multiple Fever, chills, sweats Weight loss H & N cancer risk factors - smoking, alcohol use H & N Symptoms - hoarseness - dysphagia, odynophagia - throat pain - cough - FB sensation - bleeding - otalgia Physical Exam Location Size Consistency Mobility – fixed? - moves w/swallowing? - moves w/tongue protrusion? Full Head and Neck Exam - scalp, skin - ears, nose - nasopharynx - oral cavity - oropharynx - larynx - cranial nerves - neck exam Physical Exam Have a system for your examination The neck can be broken down into regions – Anatomical triangles – Named lymph node groups – Numbered lymph node regions Neck Masses I. Neoplasms II. Infections A. Benign III. Congenital B. Malignant IV. Miscellaneous II. Infections A. Abscess B. Cervical lymphadenitis 1. Suppurative lymph node 2. Deep neck space abscess 1. 2. 3. Bacterial Granulomatous Viral Treat cervical adenitis with Antibiotics only if evidence of a bacterial infection is found on clinical exam. III. Congenital Masses A. B. C. Thyroglossal Duct Cyst - midline Branchial Cleft Cyst - lateral Dermoid - midline Treatment – Surgical excision I. Neoplasms A. Benign - benign thyroid gland tumors - benign salivary gland tumors - lipomas - schwannomas (nerve sheath) - vascular tumors Salivary Gland Disease Inflammatory - sialadenitis - sialolithiasis (calculi /stone) Neoplastic - benign - malignant Vascular Tumors Paragangliomas (Glomus tumors) z z z Hemangioma Lymphangioma Arteriovenous malformations I. Neoplasms B. Malignant 1. Primary - Lymphoma - Thyroid carcinoma - Salivary gland carcinoma - Sarcoma 2. Metastatic - Head & Neck primary - Infraclavicular primary Head and Neck Cancer Most common histology – Squamous cell carcinoma Most common sites Oral cavity Larynx Head & Neck Cancer Etiology: Smoking and alcohol Head & Neck Cancer Epidemiology: Risk increases with age, males > females Head & Neck Cancer Common Presenting Symptoms – Larynx – Hoarseness, throat pain, ear pain, dysphagia, odynophagia – Oral cavity – Growth with ulceration - pain & tenderness – Neck mass - Spread to lymph nodes (WORRY) ** Investigate oral lesion, throat symptom, or neck mass present > 4 weeks Oral Cancer (Squamous cell carcinoma) Benign oral growths Fibroma Papilloma Mucocele Leukoplakia Benign oral ulcers Traumatic Aphthous ulcer (Canker sore) Relationship Between Age and Neck Mass Etiology Pediatric (0-15yrs) Congenital>Inflammatory>>Neoplastic Young Adult (15-50) Inflammatory>Congenital>>Neoplastic Older Adult (50+ yrs) Neoplastic(malignant)>Inflammatory>> Congenital When to (Worry About) Investigate a Neck Node - Neck Node >1.5-2 cm - persistent adenopathy > 4 weeks - neck node in patient with no preceding history of URTI or H&N infection - neck node or upper AD complaint not explained by clinical exam (older, smoker, EtOH) Fine Needle Aspiration Biopsy ** The single most useful diagnostic test for a neck mass** Evaluation of a Neck Mass Warning: ** DO NOT PERFORM AN INCISIONAL BIOPSY OF A NECK MASS ** Imaging for a Neck Mass CT scan MRI scan Ultrasound Plain x-rays Sialogram Thyroid nuclear scan Angiography Take Home Points Use a headlight and free up both hands to perform a head and neck exam The most useful investigation for a neck mass after your history and physical is a FINE NEEDLE ASPIRATION BIOPSY Do not perform an incisional biopsy on a neck mass prior to a FNA biopsy Do not treat an unexplained H&N symptom or neck mass with repeated courses of antibiotics Head and Neck Cancer - Key Points Histology - Squamous Cell Carcinoma Etiology - Smoking / Alcohol Common sites - Oral cavity & larynx Common presenting symptoms Oral growth / ulcer Hoarseness, throat pain, ear pain, odynophagia Neck mass Consider the diagnosis Biopsy – Biopsy oral / pharyngeal lesions – Fine Needle Biopsy of Neck Masses So, When to Worry? Cervical node >1.5 – 2 cm, present for >4 weeks Cervical node with no preceding history of URTI or H&N infection Persistent voice, throat or swallowing complaint not explained by physical exam