Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
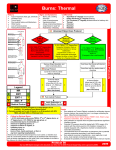
Burn Care: Pediatric Considerations Judah Slavkovsky April 24th, 2014 Today in 1184 BC: The Greeks sack Troy Introduction • Burns declining steadily over last 20yrs – 1.24 million burns yr, 1/3 children – 60-80K hospitalizations, 30K children – 4K deaths, 1K children • Likely to be hospitalized, unlikely to die Two Mechanisms: • House fires: – Leading cause of burn related deaths in children – Esp. 0-5y – Preschool also high (2x national average) Two Mechanisms Cont. • Scalds – V common, under 3y – Both accidental and non-accidental – Reaching, pulling appliance cords, climbing into hot baths Real and durable progress last 20yrs • Advances: – Fluid resus – Early excision and grafting – Infection control – Tx of inhalation injury – Nutritional support – Management of the hypermetabolic state Real and durable progress • Largest improvement in burn mortality has been in children (0-14y) • 1949 – 50% mortality with 49% TBSA • 2014 – 50% mortality with 98% TBSA Mortality Predictors in >80% TBSA Burns • • • • TBSA >95% Children under 2y Inhalation injury Delay in IV access IV Access • Need IVF w/i 1st hr – delay major driver of mortality Pediatric Resuscitation Considerations - Get access FAST • Systemic capillary leak – pronounced for first 1824hrs With small circulating volume, access delay of > 30m - Profound shock • Peripheral IV best, through burn - OK • Central lines OK – femoral often easiest with edema • Low threshold for IO – OK for all ages Peds Resus • Hyponatremia – V. frequently observed in first 48hrs – High urinary Na losses – Check frequently • Potassium replacement: Oral K phos – Hypophosphatemia ->frequent • Neonates: small glucose stores – Separate maintenance IVF w dextrose Peds Resus cont • Children much more prone to vasogenic edema – over exuberant catecholamine and chemokine response to burn • Parkland Formula – underestimation esp. with deep, electrical, inhalation injury • Capillary leak omnipresent – Albumin use more frequently – 8hrs after - burn albumen remains in circulation • Maintain serum levels >2.5 Over Resus • Pulm edema, ARDS, compartment syndromes • Cerebral edema – Head of bed elevation – 1st 24-48hrs Resus guideposts • UOP – 1ml/kg/hr children, 2ml/kg/hr infants • Pulse pressure, distal extremity color, capillary refill • MAP, base deficit, lactate • All parameters can be erroneous - Data review: No better markers • New: – Thermal dilution catheters (PiCCO) The PiCCO Catheter • Pulse Couture Cardiac Output – Arterial line – Femoral in children (6cm – 3F) – Calibrated with thermodilution (like pulmonary artery cath) – Arterial pressure wave form used to establish stroke volume with mathematical algorithm • CO • SVR • Stroke volume variability A few words on inhalation injury • Flow: r4 • Peds mortality: isolated burn: 1-2% - presence of inhalation inj: 40% • Nebulized heparin and acetylcysteine The Burn Wound • Early tangential excision and grafting: Pillar burn care – Zora Jansekovic 1960s (Yugoslavia) – Originated in children Unable to tolerate infections and metabolic derangements of autolysis Coverings • Autografts • Xenografts • Allografts Dermatome at scalp xenoderm New(er) techniques • Large full thickness burns with loss of dermis – more prevalent in children • Nearly all structural skin properties – dermis – Flexibility, elastic recoil, strength • Dermal substitutes Integra • MGH and MIT • Dermal analog – Porous matrix of cross-linked bovine collagen and glycosaminoglycan – “Scaffolding” organizes cellular invasion and capillary growth – Silicone overlay – humidity and bacterial barrier • Incorporates into wound bed – 2-3w later thin STSG layered over 5 picute figure of boy AlloDerm • Cryopreserved allogeneic dermis • Obtained from cadaver donors – Hypertonic saline, epithelium removed – Detergent inactivate cellular and viral components – Freeze dried – rehydrated before use • Basement membrane proteins intact – Combined with thin overlying epithelial autograft at time of closure • Limited use – but animal models suggest least scar contractures of available dermal substitutes Scalds • Most common form of burn, esp <4y • Exception to rule of early excison – Less area excised and blood loss – with delayed surgery (2nd, 3rd week) – Often difficult to judge depth of tissue injury – If under 20-30%TBSA Wait Teen age shald Scalds • Prolonged period of dressing changes • Synthetic and biosynthetic membranes – Biobrane • Nylon/silicone bilaminated neoepidermis, w/ porcine type I collegen • No increase in infections, fewer dressing changes, reduced pain med use – Suprathel • Copolymer of D&L – lactide • Derived from starch • Less pain – similar healing times Boy scald Hypermetabolic Response: developing field • Major cause of poor outcome in children – seem to have an overly robust response. • Severe alterations in metabolism of – Glucose, lipids, amino acids • Severe Catabolism – Protein loss from muscle and organs – Multiple organ dysfunction • Hypermetabolism linked to organ function and survival Cause • Not entirely clear – Thousands of identified genes w/ altered expression after major burn • Many w roles in mitochondrial and immune function – Hypothymic thermoregulatory “reset” • Increased heat production, HR, cardiac output • Persistent increases in: – – – – – Catecholamines Glucocorticoids Glucagon Dopamine Additional players: nitric oxide, complement cascades, neutrophil-adherence complexes, reactive oxygen species, and endotoxins Persists • Thought to resolve after wounds closed • Accumulating evidence process lasts much longer – 3 yrs + • At 3 yrs all higher than baseline – Energy needs, circulating catecholamines, urine cortisol – Insulin resistance, impaired glucose intolerance Growth • Near complete lack of bone growth for 2y – Endogenous glucocorticoids, Vit D – Long term osteopenia – Possible reductions in peak bone mass – Linear growth delay (height and weight) 1 yr after burn • Slowly resolves to near nml rate by post burn yr 3. • Never catch up Loss of growth (velocity) All pts: >40% TBSA Same pattern true of girls – but fewer data points Fat redistribution • Multiple organs infiltrated • Best studied: Liver – Children w/ major burns: 3-5 fold increase in hepatic triglycerides • Increases subsequent risks: – Infection – Progression to sepsis Treatments of Hypermetabolic Response: Unsolved problem • Early and accurate feeding – Initiate w/i 1st 12hrs • Glutamate? • Keep room warm – 77ᵒF to 91ᵒ – Reduced energy expenditure from 2 to 1.4 times predicted need • Exercise early – Resistance – Rigorous play Pharmacologic Aids • Propranolol – Effects on tachycardia – Slows catabolism of skeletal muscle – Reduces fatty liver: inhibits peripheral lipolysis – Reduces bone demineralization – Reduces hypertrophic scaring More Meds: • Recombinate Growth Hormone – No improvement over exercise alone – Interest in using for growth catch up • Oxandrolone – anabolic steroid – Augments exercise effect – Improves bone rates of growth Conclusions • Children are over represented in burn care • Nearly all survive • Any delay in resuscitation affects mortality • Evolving approaches to cover large wounds • Scalds are often smaller than first appear - wait • Hypermetabolism after burns is profound, long lived and a largely unsolved riddle in burn care.