Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
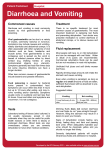
Diarrhea What is Diarrhoea? Diarrhoea is a symptom characterized by an abnormal increase in stool frequency (more than 3 times daily) or liquidity (> 80% water); The normal frequency of bowel movements varies with each individual Diarrhoea DEFINITIONS – IDSA & WGO “Diarrhea” is an alteration in a normal bowel movement characterized by an increase in the water content, volume, or frequency of stools. In adults, a decrease in consistency (i.e., soft or liquid) and an increase in frequency of bowel movements to >3 stools per day (24 hrs) have often been used as a definition for epidemiological investigations. Diarrhea is defined as daily stools with a mass greater than 15 g/kg for children younger than 2 years and greater than 200 g for children aged 2 years and older. “Infectious diarrhea” is diarrhea due to an infectious etiology, often accompanied by symptoms of nausea, vomiting, or abdominal cramps. Dysentery describes an infectious diarrhea with visible blood and mucus in the stool. “Acute diarrhea” is an episode of diarrhea of <14 days in duration. “Persistent diarrhea” is diarrhea of 14 or more days in duration. Some experts refer to diarrhea that lasts 30 days or more as “chronic.” Diarrhoea3 Causes: bacterial or viral infection through ingestion of contaminated food or drink; 1. E.Coli, S.aureus toxins mucosal cells hypersecretion of fluid watery diarrhoea with little or no fever or other symptoms; Diarrhoea Causes: 2. Invasive E. coli, salmonella and shigella: directly invade mucosal epithelial cells and cause an inflammatory reaction less fluid diarrhoea accompanied by nausea, vomiting, cramps and sometimes low-grade fever Diarrhoea Causes: 3. Viral infections, which often affect babies and young children, also produce watery diarrhoea 4. Non-infective causes: stress, alcohol, and hot spicy food 5. Drugs: antibiotics “all but varying degrees”. Depends on extent that drug disrupts normal intestinal microflora. Other: laxatives, misoprostol. Olsalazine, anticancer, antihypertensive agents, parasympathomimitic drugs, digoxin, quinidine, magnesium hydroxide, laxatives. 6. Chronic diarrhea. Lasts more than 4 weeks. Protozoal infections, food, IBS, hyperthyroidism. Diarrhoea Infectious diarrhea Infectious diarrhea is further inflammatory diarrhea. classified into non-inflammatory and Non-inflammatory diarrheas Inflammatory diarrheas Generally a less severe illness Generally a more severe illness Patients present with nonbloody, watery stools; patients are afebrile and without significant abdominal pain. Patients present with bloody diarrhea, severe abdominal pain, and fever. Examination of stool specimens does not reveal the presence of fecal white blood cells (WBC) or occult blood. Examination of stool specimens reveals the presence of large numbers of fecal leukocytes. Typically caused by rotaviruses, noroviruses, Staphylococcus aureus, Bacillus cereus, Clostridium perfringens, Cryptosporidium parvum, and Giardia lamblia. Caused by invasive pathogens including Campylobacter jejuni, Shigella species, Salmonella species, Clostridium difficile, Shiga toxin-producing Escherichia coli (STEC), and Entamoeba histolytica. Most patients require only supportive therapies Selected persons may benefit from antimicrobial therapy directed at the causative pathogen. Diarrhoea7 Consequences Normal faeces contain 60-85 % water Water loss during defecation= 70-200 mL/day In diarrhoea: water loss 4X normal K and Na loss fall in plasma pH (acidosis) serious metabolic consequences Fluid & electrolyte losses are increased if vomiting also occurs Diarrhoea Consequences In babies/children: hazardous as high proportion of total body weight is lost and dehydration can occur very rapidly Elderly are also particularly sensitive to the effects of fluid and electrolytes loss, especially if on diuretics Reduction in blood volume + RAS + aldosterone (1) loss of K (hypokalemia) (2) Excessive fluid loss reduction of renal artery flow renal failure Diarrhoea Patient Evaluation: All of the following must be considered before selecting the most appropriate management. Age Onset and duration or diarrhea Description of stool Other symptoms Medications Recent travel Medical history. Diarrhoea 10 When to refer to a physician Very young or very old. Bloody stool. High fever (greater than 38.5 ˚C). Dehydration or weight loss greater than 5 % of total body weight. Signs of dehydration: dry mouth, sunken eyes, crying without tears, dry skin that is less elastic than normal skin. Severe vomiting.. Duration: (see next slide) Diarrhoea 11 When to Refer? If diarrhoea lasts more than: 72 hours : adults and older children 48 hours : children < 3 years old & elderly 24 hours in children < 1 year old Refer Immediately in infants under 3 months old Diarrhoea Diarrhoea 13 Diarrhoea 14 Treatment of children based on the degree of dehydration Diarrhoea 15 Treatment Oral rehydration therapy (ORT) Opioids Adsorpants Dietary management In UK: belladonna extract Diarrhoea Oral rehydration therapy (ORT) First line treatment of acute diarrhoea the very young & elderly (particularly important) ORT not intended to relieve symptoms Use of antidiarrheals (antimotility drugs or adorbants) is regarded unnecessary and sometimes undesirable Use of antidiarrheals (for comfort/convenience) is used as adjunct to ORT Diarrhoea Oral rehydration therapy (ORT) Mode of action: replace water and electrolytes lost through diarrhoea and vomiting; K & Na: replace ions citrate and/or bicarbonate: correct acidosis glucose: carrier for Na ions and hence water across the mucosa of the small intestine Diarrhoea Oral rehydration therapy (ORT) ORT is not intended to stop diarrhoea, but acute diarrhoea is self-limiting and normally ceases within 24-48 hours; ORT can be recommended for patients of any age, even when referral to a doctor is considered necessary Diarrhoea ORT is not intended to stop diarrhea, but acute diarrhea is self-limiting and normally ceases within 24–48 hours. ORT can be recommended for patients of any age, even when referral to a doctor is considered necessary. An oral rehydration product (Dioralyte Relief [Sanofi-Aventis]) containing powdered rice starch in place of glucose is claimed to achieve even greater rehydration than glucose over time, and the rice starch is claimed to help produce firmer stools, leading to faster recovery compared with glucose. A Cochrane Review found that polymer (including rice)-based ORS showed some advantages compared with glucose-based ORS for treating diarrhea of any cause. Diarrhoea 20 Dose & Administration of ORS the content of 1 sachet or 2 effervescent tablets should be dissolved in 200-250 ml of water (freshly bolied and cooled in case of infants) discard unused solution 1 hr after reconstitution or no longer than 24 hrs (if refrigerated) Dose, adults: 200-400 ml after every loose motion, or 2-4 L over 4-6 hrs Diarrhoea Dose & Administration of ORS Patients may prefer to sip 1-2 tsp every few minutes rather than drink large quantities less frequently children > 2 yrs: cupful (200ml) after every loose stool children < 2 yrs: ¼- ½ cupful Infants: 1-1.5 normal feed volume Both breast and bottle-fed babies should continue to be fed normally (without dilution) Diarrhoea Contraindications & cautions No contraindications to ORS unless the patient is vomiting frequently IV fluid and electrolyte replacement; fluid overload from excessive administration of ORS is highly unlikely unless continued for babies and young children > 48 hrs (recognised by puffy eyelids) rapidly withhold ORS and other liquids Diarrhoea Opioids Loperamide, Morphine, Codeine Mode of action: 1. increase tone of both small and large bowel and reduce intestinal motility (enhances fluid and electrolyte reabsorption); 2. increase the sphincter tone and decrease secretory activity along GIT Diarrhoea Loperamide It is a synthetic opioid agonist that has a high affinity for, and exerts a direct action on opiate receptors in the gut wall; also has a high first-pass metabolism so very little reaches the systemic circulation; effective in reducing the duration of diarrhea (25 vs 40 hrs with placebo) Diarrhoea Loperamide 50 fold more potent than morphine and 23 times more potent than diphenoxylate in its effect on GI motility, but penetrates the CNS poorly, thus has lower risk of CNS side effects; Other mechanisms: disruption of cholinergic and non-cholinergic mechanisms of peristalsis, inhibition of calmodulin function and inhibition of voltage dependent Ca channels Diarrhoea Loperamide Indications: traveller’s diarrhoea non-specific acute diarrhoea chronic diarrhoea associated with inflammatory bowel disease AAP does not recommend use in children < 6 years old Used when patient is afebrile or have mild fever and does not have bloody stool Diarrhoea Loperamide Dosage & Administration dosage forms: caplets (2 mg), and liquid (1 mg/5ml) Dose: 4 mg initially, then 2 mg after each loose stool/ Do not exceed 16 mg/day Consult product instructions for pediatric dose Diarrhoea Loperamide Contraindication Loperamide should not be used in patients with fecal leukocytes, high fever, or blood or mucus in the stool (dysentery); Loperamide may cause paralytic ileus in patients with desentery Paralytic ileus: paralysis or inactivity of the intestine that prohibits the passage of material within the intestine. May be a result of anticholinergic drugs, injury or surgery Diarrhoea Adsorbents Kaolin, pectin, attapulgite and bismuth subsalicylate; Kaolin: a natural hydrated aluminum silicate. Not absorbed from GIT, 90% metabolized in gut and excreted in faeces Attapulgite is another naturally occur clay mineral, consisting of hydrous Mg-Al-silicate; kaolin & attapulgite have varying and relatively weak adsorptive properties in respect to diarrhoea producing bacteria Diarrhoea Adsorbents Mode of action: 1. adsorb the microbial toxins and microorganisms to their own surfaces drugs not absorbed from the GIT toxins and MOs are excreted in stool; 2. Hydrophilic adsorbents (e.g. pectin and bulkforming agents; ispaguala, methylcellulose, and sterculia), bind water within the intestine causing watery stool to become more formed Diarrhoea Adsorbents the main constituents in the antidiarrhoeal preparations for young children (whom opiates and antimuscarinics are contraindicated); not absorbed from GIT harmless and safe to use Debate: reduce evacuation of faecesprolong presence of pathogens/toxins in bowel. Adsorption: non-specific process (medicines) Diarrhoea Dietary Management Traditionally: withdrawal of feedings, initiation of clear liquids, with a slow reintroduction of feedings in 24 hrs However, oral intake does not worsen diarrhoea, clinically significant nutrient malabsorption is uncommon (80-95% CHO, 70% of fat and 75% of the nitrogen from protein) in acute diarrhoea and bowel rest is generally not necessary Diarrhoea What foods are best for refeeding? most infants and children with diarheoa can tolerate full-strength breats milk and cow’s milk; The familiar BRAT (bananas, rice, apple sauce and toast) is frequently prescribed insufficient calories, protein and fat especially in strict or prolonged use and is not recommended by AAP Diarrhoea What foods are best for refeeding? Diet should include: complex carbohydrate-rich foods (e.g. rice, potatoes, bread, cereals) Yogurt lean meats Fruits and vegetables Diarrhoea What foods are best for refeeding? Avoid: fatty foods foods rich in simple sugars that may cause osmotic diarrhoea spicy foods that may cause GI upset Caffeine (WHY??) Diarrhoea PROBIOTICS: AN UPDATE Diarrhoea 43 Background Probiotics are live organisms that are ingested to provide therapeutic or preventative benefit for the host. The most commonly used are the lactic acidproducing bacteria bifidobacteria and lactobacilli. Probiotics also include the yeast Saccharomyces boulardii. Probiotics are commonly promoted to strengthen the immune defenses. Diarrhoea 44 Bifidobacteria spp Saccharomyces boulardii Diarrhoea 45 Probiotics, Beneficial Microbes Beneficial microbes such as bifidobacteria live in the intestinal ecosystem with potentially pathogenic bacteria. Beneficial microbes prevent the overgrowth of “bad bacteria” by producing antimicrobial agents. Additionally, beneficial microbes competitively limit pathogenic bacterial overgrowth by occupying receptor sites and vying for space and nutrients. Beneficial microbes may also increase intestinal production of mucin, which stimulates the production of mucus, forming a protective barrier on the intestinal lining Diarrhoea 46 Diarrhoea 47 In order to be effective, probiotics must be able to withstand a wide range of pH variation. Many microbes cannot withstand the protective acid barrier of the stomach and the effects of bile. An effective probiotic also must be able to colonize the gut and be able to attach to the intestinal epithelium. Additionally, the probiotic should not disturb healthy intestinal microbes Diarrhoea 48 Probiotic Bacteria and Yeasts Bifidobacteria are anaerobic, rod-shaped, gram-positive bacteria. Bifidobacteria are the most prominent beneficial microbes in the colon. Bifidobacteria produce antimicrobial substances that have a broad spectrum of antimicrobial activity Diarrhoea 49 Bifidobacteria that are commonly used as probiotics include Bifidobacterium longum, B. breve, B. infantis, B. bifidum, B. lactis, and B. adolescentis. Bifidobacteria supplements are most commonly combined with other probiotics. Lactobacilli are a group of gram-positive rods that are obligate and facultative anaerobes. Diarrhoea 50 Other bacteria sometimes used as probiotics include Streptococcus thermophilus and Leuconostoc species. The yeasts Saccharomyces boulardii and S. cerevisiae are also used Diarrhoea 51 Probiotics for Diarrhea Probiotics may be useful as adjunctive treatment of adults and children with infectious diarrhea. Several species of Lactobacillus seem to reduce the duration of diarrhea, particularly in rotaviral infections. For antibiotic-associated diarrhea, Lactobacillus rhamnosus GG, S. boulardii, and probiotic mixtures appear to be effective prophylactic agents. Given along with antibiotics, these probiotics can reduce the incidence of diarrhea by about 60% to 65%. The effectiveness of probiotics on treatment of antibiotic-associated diarrhea is less clear. Diarrhoea 52 Diarrhoea 54 Diarrhoea 57 SAFETY Diarrhoea 58 Diarrhoea 59 SUMMARY Diarrhoea 60 Diarrhoea 61 Diarrhoea 62