Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Obesity and the environment wikipedia , lookup
Calorie restriction wikipedia , lookup
Waist–hip ratio wikipedia , lookup
Low-carbohydrate diet wikipedia , lookup
Body fat percentage wikipedia , lookup
Thrifty gene hypothesis wikipedia , lookup
Human nutrition wikipedia , lookup
Adipose tissue wikipedia , lookup
Fat acceptance movement wikipedia , lookup
Diet-induced obesity model wikipedia , lookup
Abdominal obesity wikipedia , lookup
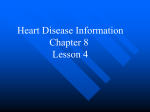
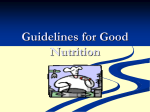
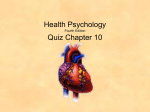
Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ For Dr Trudi Deakin, X-PERT Health (registered charity), Hebden Bridge, West Yorkshire, UK Have we been fighting the wrong demons? Despite significant advances in management strategies, coronary heart disease (CHD) remains the leading cause of morbidity and mortality. Diabetes increases risk of myocardial infarction by 55% and, between 2010–2012, 37 000 people with diabetes in England/Wales were hospitalised with CHD.1 Given the role played by fatty plaque (containing cholesterol) earlier thinking demonised dietary saturated fat. Why was saturated fat implicated in the aetiology of CHD? Was it justified? Researchers since the 1950s focused on the diet-heart hypothesis but with severe methodological limitations.2 There was also a failure to establish a cause and effect relationship between dietary saturated fat and CHD.3 The diet-heart hypothesis did appear simple, logical and well-founded suggesting that death from CHD can be prevented. However, despite it having been the cornerstone of dietary recommendations for almost 40 years, it has never been proven.2 Although a low saturated fat diet has been shown to reduce LDL-C levels in some studies,4 these findings have not been consistent5 and often have a detrimental impact on HDL-C6 without preventing CHD in people with and without diabetes.7,8 Some studies have even shown an inverse correlation between cholesterol levels and mortality.9 Thus, neither the level of serum lipids nor CHD can be related to saturated fat.10,11 A Cochrane systematic review of randomised controlled trials (RCTs) concluded that there was no evidence that reduced saturated fat diets reduce total or CHD mortality and, although there was a moderate effect for CHD events, there was high heterogeneity and the effect disappeared when only studies that significantly reduced saturated fat were included.12 Recent systematic reviews and meta-analyses conclude that current evidence does not support cardiovascular guidelines that encourage high consumption of polyunsaturated fatty acids and low consumption of total saturated fats in the primary and secondary prevention of CHD, and there is no significant evidence for concluding that dietary saturated fat is associated with an increased risk of CHD.13,14 Low fat/saturated fat dietary recommendations were launched in the US2/UK15 in the absence of supporting evidence from RCTs.16 Since then, the prevalence of obesity has tripled from 6% of women/8% of men to 25%. Diabetes prevalence has quadrupled from 1.4% to 6%.17,18 What is saturated fat? Fat is a component of every cell, serves as the primary energy reserve and is transported as triglyceride (TG). Saturated fats contain no double bonds, allowing the hydrocarbon chains to pack closely together making them 254 PRACTICAL DIABETES VOL. 32 NO. 7 solid at room temperature. Fatty acids can vary from within and between TG molecules depending on their availability. No food contains 100% of one type of fatty acid or TG. Dietary TGs are broken down by lipases before being packaged into chylomicrons and entering the plasma. Triglycerides generated by the liver are transported in very low density lipoproteins (VLDLs). Fat storage and plasma saturated fat Adipose tissue lipogenesis and lipolysis are regulated by many hormones including insulin and glucagon. Triglycerides are synthesised from non-esterified fatty acids. In the liver, saturated fat, palmitate (C16:0), is synthesised from dietary carbohydrates by de novo lipogenesis (DNL); (Figure 1). Thus, glucose promotes plasma levels of saturated fat.19,20 What is CHD? CHD is multifactorial. The diet-heart hypothesis focuses on atherosclerosis. The cascade of events involves systemic inflammation resulting from oxidised lipoproteins, enhanced monocyte-derived macrophages uptake and foam cell formation. Resulting plaques protruding into the arterial lumen can rupture, leading to myocardial infarction.21 Why is cholesterol implicated in CHD? Around 25% of cholesterol comes from the diet (exogenous) with 75% made by cells (endogenous) reducing the demand for plasma cholesterol.22 Cholesterol is available as unesterified (UC) or as cholesterol esters (CE). Dietary cholesterol needs to be de-esterified before absorption and the absorption rate is poor. Bile cholesterol can be reabsorbed by gut enterocytes.23 Blood cholesterol has been used to assess risk of CHD. LDL cholesterol (LDL-C) is commonly termed bad cholesterol and HDL-cholesterol (HDL-C), good cholesterol. However, all cholesterol is essential. The only negative is when cholesterol is deposited inside the artery wall. Cholesterol is hydrophobic and requires a protein carrier to be transported in the blood. The combination of cholesterol, TG and phospholipids and apolipoprotein forms lipoproteins. Small dense lipoproteins may enter the arterial wall, be oxidised and scavenged by monocytes and converted to macrophages and foam cells causing CHD. Cholesterol is merely the innocent passenger. Not all lipoproteins are the same. Chylomicrons (ApoB-48) are produced after a meal. VLDLs (ApoB-100) are produced by the liver and are the predominant carriers of TGs. LDLs are by-products of VLDL metabolism and are usually the primary carriers of plasma cholesterol. HDL particles (HDL-P), produced by the liver and intestine, mature and become enriched with ApoA-1. HDLs protect against atherosclerosis by anti-inflammatory properties and reverse cholesterol transport.24,25 The size and density differ between and within types of lipoprotein due to lipidation and delipidation and this makes the standard COPYRIGHT © 2015 JOHN WILEY & SONS Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ Sugar (sucrose) Starches (polysaccharides) Fat (triglycerides) Glucose Transported in chylomicrons Stimulated by glucagon Stimulated by insulin Fructose Glycogen Lipogenesis ↑ Body fat Glycolysis Lipolysis ↓ Body fat Stimulated by glucagon De novo lipogenesis ↑ Blood triglycerides Pyruvate Stimulated by insulin Acetyl CoA Stimulated by glucagon Stimulated by insulin HMG CoA Krebs cycle HMG CoA ↑ Blood cholesterol Energy ↑ Blood ketones Figure 1. Metabolic pathways of dietary carbohydrate and fat lipid profile (LDL-C, HDL-C, and TG) less reliable measures for assessing CHD risk.26 LDL-C is not the problem Lowering LDL-C became a primary goal in CHD prevention but has limitations: • LDL-C can be measured but is usually calculated using the Friedewald equation, which can underestimate or overestimate the cholesterol content in LDL particles (LDL-P).27 • LDL-C is only an indirect marker of CHD risk as it is solely the lipoprotein which initiates atherosclerosis. LDL-P is a strong predictor of CHD as an abundance of small dense LDL-P has been shown to be atherogenic as they are much more likely to become oxidised and lodged PRACTICAL DIABETES VOL. 32 NO. 7 in the arteries.28,29 ApoB-100 and LDL-P indicate the number of atherogenic particles (<1000nmol/L is considered ideal).30 Size of LDL-P can also be measured (<25nm is associated with an increased risk of CHD).31 People with diabetes and CHD often have normal levels of LDL-C but increased numbers of small dense LDL-P32,33 resulting in a three- to six-fold greater risk of CHD.28,34 Liver DNL drives the production of TG-rich VLDLs, which cause LDL and HDL to become cholesterol-poor and TG-rich. Remnant VLDLs are smaller, carrying predominantly CE which is associated with increased CHD risk.35 Small HDL-P are excreted in the kidney further contributing to dyslipidaemia. Hepatic LDL receptors do not recognise small LDL-P so they remain in the plasma for fuelling high levels of atherogenic LDL-P (Figure 2).36–38 COPYRIGHT © 2015 JOHN WILEY & SONS 255 Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ LDL and HDL particle abnormalities in hypertrigliceridaemia TG CETP Excess dietary carbohydrate De novo lipogenesis TG-rich VLDL HL Large LDL-P (ApoB-100) Small dense LDL-P Not recognised by liver LDL receptors Abundance of small dense LDL-P Oxidised LDL-P CE CETP Large HDL-P (ApoA-1) TG Small HDL-P Excreted via the kidney Low levels of HDL-C Macrophages HL Fatty plaques TG: triglyceride; VLDL: very low density lipoprotein; CETP: cholesterol ester transfer protein; CE: cholesterol ester; LDL-P: low density lipoprotein particles; HDL-P: high density lipoprotein particles; HL: hepatic lipase; HDL-C: high density lipoprotein cholesterol. Figure 2. Creation of atherogenic small dense LDL particles Controversy exists as to whether LDL-P size, LDL-P number or discordant LDL-C and LDL-P leads to the greatest risk.39 In patients with diabetes who presented with ideal LDL-C, HDL-C and TG levels, LDL-P was only concordant with LDL-C in 22% of cases.23 Thus, when TGs are elevated and HDL-C is low, small LDL-P predominate despite normal/low LDL-C.40 Although ApoB-100 and LDL-P are believed to be better risk predictors of CHD than LDL-C, they are not routinely monitored in the UK. Non-HDL cholesterol is a better predictor of CHD risk than LDL-C and can be calculated from a non-fasting lipid profile.32 NICE has now recommended it instead of LDL-C.41 The TG/HDL-C ratio has been shown to be a good predictor of LDL-P size42 and correlates strongly with the incidence and extent of CHD43 in men44 and women.45 A ratio of <0.87 is ideal (mmol/L [2 for mg/dl]) whereas a ratio >1.74 (mmol/L [4mg/dl]) is a powerful independent predictor of developing CHD. In epidemiological studies seeking a relationship between LDL-C and the risk of CHD, up to half of patients with CHD have cholesterol levels in the normal range.46 The Framingham Heart Study demonstrated that increased total-C can be protective against mortality risk with increasing age, and lipoprotein/apolipoprotein values are likely to be more appropriate screening devices because two individuals may have an identical LDL-C but differ with respect to particle size and concentration.47 What are the real risk factors for CHD in people with diabetes? Increased risk of CHD in people with diabetes is unlikely to be associated with total-C as, in England and Wales, 40% of patients achieve a cholesterol level <4mmol/L and 77% <5mmol/L.1 In comparison, the general population UK average for men is 5.5mmol/L and 5.6mmol/L for women, with 22% of the adult population having a cholesterol level >6.5mmol/L.48 Correlation does not prove causation but of interest is the weak negative correlation between mean total 256 PRACTICAL DIABETES VOL. 32 NO. 7 cholesterol and mortality, indicating that higher cholesterol levels may protect from CVD and diabetes mortality. The orange marker in Figures 3 to 6 denotes the UK.49 Modifiable risk factors include dyslipidaemia (above), hyperinsulinaemia, hyperglycaemia, hepatic insulin resistance and non-alcoholic fatty liver disease (NAFLD).26,50–52 If saturated fat is not implicated in the aetiology of CHD, what dietary factors are? What can we learn from our human ancestors? Evidence from archaeological records suggests that hunter-gatherers consumed a high animal fat diet53 and the modal age of death for those who survived past 15 was 72.54 Teeth were free from dental caries and there is no evidence that the diet caused any of the long-term conditions that are experienced today.55 If saturated fat caused heart disease, it would have been evident in this population. Modern-day diets since have seen an increase in calorie intake mainly from sugars, breakfast cereals and processed vegetable oils with a dramatic reduction in eggs, meat, full fat milk/dairy products and vegetables (Figures 7 and 8).56,57 The likely dietary culprits that influence CHD • Trans fats due to insulin resistance, inflammation and endothelial dysfunction.58 • PUFA from processed vegetable oils due to an unbalanced intake of omega-6:omega-3 fatty ratio59 and omega-6 fats pro-inflammatory impacts on health.60,61 • Processed food and snacks that have become the norm increasing refined vegetable fat and carbohydrate intakes.20,56 • Excessive consumption of sugars and refined starches due to the low-fat dietary recommendations and food manufacturer influences which have been shown to be detrimental to health,62 increase insulin resistance,63 atherogenic dyslipidemia,64–67 NAFLD inflammation68 and energy expenditure.69 COPYRIGHT © 2015 JOHN WILEY & SONS Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ Diabetes deaths per 100 000 CVD deaths per 1000 000 1200 1000 800 600 400 200 0 4.5 4.7 4.9 5.1 5.3 5.5 5.7 5.9 Mean cholesterol (mmol/L) 6.1 6.3 800 700 600 500 400 300 200 100 0 4.7 4.9 5.1 5.3 5.5 5.7 5.9 Mean cholesterol (mmol/L) 6.1 1980 Cakes and pastries Breakfast cereal Sugar sweetened beverages 2000 Figure 7. UK starch and sugar intake per adult 1980–2013 In contrast, diets lower in carbohydrate70,71 which include animal foods that are naturally high in fat tend to be healthy and nutritious (non-factory farmed meat,72 eggs,73 milk and dairy products74,75 and coconut products76). Why should we stop demonising saturated fat? It is now accepted by the Academy of Nutrition and Dietetics that carbohydrate contributes a greater amount to CVD risk than saturated fat.77 The diet-heart hypothesis has been meticulously measured and found incorrect. The PRACTICAL DIABETES VOL. 32 NO. 7 5.1 5.3 5.5 5.7 5.9 Mean cholesterol (mmol/L) 6.1 6.3 30 25 20 15 10 5 0 4.7 4.9 5.1 5.3 5.5 5.7 Mean cholesterol (mmol/L) 5.9 6.1 Figure 6. Females in European countries: diabetes death rates per mean country cholesterol level. (Orange marker denotes the UK) 350 300 250 200 150 100 50 0 2013 Biscuits Sugar, preserves and confectionary 4.9 35 4.5 Amount per adult per week (ml) 900 800 700 600 500 400 300 200 100 0 4.7 Figure 4. Males in European countries: diabetes death rates per mean country cholesterol level. (Orange marker denotes the UK) 6.3 Figure 5. Females in European countries: CVD death rates per mean country cholesterol level. (Orange marker denotes the UK) Amount per adult per week (g) 4.5 Diabetes deaths per 100 000 CVD deaths per 100 000 Figure 3. Males in European countries: CVD death rates per mean country cholesterol level. (Orange marker denotes the UK) 4.5 40 35 30 25 20 15 10 5 0 1980 Butter 2000 Margarine Vegetable oils 2013 Total fats Figure 8. UK fats and oils intake per adult 1980–2013 simple fact is dietary saturated fat does not increase blood levels of cholesterol and cause CHD. It is now time to retire that theory and concentrate on researching and recommending a diet to people with diabetes that will benefit their health and reduce risk of morbidity and mortality. Declaration of interests The author is Chief Executive of the charitable not-forprofit organisation, X-PERT Health. References References are available in Practical Diabetes online at www.practicaldiabetes.com. COPYRIGHT © 2015 JOHN WILEY & SONS 257 Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ Against Leonie Garden, Senior Diabetes Specialist Dietitian, The James Cook University Hospital, NHS South Tees, Middlesbrough, UK National dietary guidelines were introduced in the UK in 1983 by the National Advisory Committee on Nutritional Education recommending that overall fat consumption be reduced to 30% of total energy intake with saturated fat intakes comprising no more than 10% of total energy.1 This equates to no more than 20g per day for women and 30g per day for men. These guidelines followed the publication of the Seven Countries Study by Keys in 1970 which highlighted a link between high serum cholesterol levels and coronary heart disease (CHD) incidence, with higher levels of saturated fat consumption tending to be related to CHD disease.2,3 Recent publications have questioned this guidance and whether we should continue to follow its dietary principles.4–6 The risk of CHD is multifactorial and cannot be blamed on one single nutrient or lifestyle factor. It is therefore essential to consider the diet as a whole and move away from recommendations built on one particular nutrient.7 The science The carbon atoms in saturated fats are linked only by single bonds. Principally derived from animal fats, they have a relatively high melting temperature and are solid at room temperature.8 Evidence has shown that low-density lipoprotein (LDL) receptors are down-regulated by the consumption of saturated fat thus reducing the rate of LDL removal from the circulation.9 The consequence of this is a raised level of LDL, and therefore total cholesterol in the blood. The process of atherogenesis is enhanced by an increased intake of saturated fat leading to an increase in the risk of CHD.3 An increase in total fat intake results in postprandial activation of factor VII and suppresses clot breakdown. Saturated fat increases platelet activity, whereas polyunsaturated fats have the opposite effect.8 Death from CHD is significantly elevated in those with diabetes mellitus. They are three to four times more likely to die from CHD and two to three times more likely to suffer a stroke.10 This risk is not related to hyperglycaemia per se but to disturbances in other metabolic parameters such as blood lipids, which occur in the presence of poor glycaemic control. Diabetes is a non-modifiable risk factor for CHD. However, dietary approaches resulting in a reduction in total cholesterol and LDL cholesterol have been shown to improve CHD outcomes in people with diabetes.11 No-one can ignore the overwhelming body of evidence which shows that a diet rich in saturated fat leads to an increase in total serum cholesterol levels.7,12 Palmitic, myristic and lauric acid are three fatty acids which have been shown in both clinical studies and meta-analysis to raise levels of LDL cholesterol.13 An elevated LDL level is a significant modifiable risk factor for CHD. It has been shown that saturated fat looks as if it interferes with the way in which the body regulates cholesterol.8 Cutting down on saturated fat and substituting 258 PRACTICAL DIABETES VOL. 32 NO. 7 it with unsaturated fat leads to reductions in LDL cholesterol, total cholesterol to high-density lipoprotein (HDL) ratio and therefore CHD risk.14 Recent publications Recent controversy over saturated fat consumption began in 2013 when Malhotra published a paper in the British Medical Journal suggesting that saturated fat has been falsely demonised.4 However, he concluded by suggesting that we should all consume a Mediterranean style diet which is high in monounsaturated fats – surely contradicting his original claims? In March 2014, the Annals of Internal Medicine followed suit publishing a meta-analysis of 72 studies examining the effect of different fats on CHD risk.5 They concluded that ‘current evidence does not clearly support guidelines that encourage high consumption of polyunsaturated fatty acids and low consumption of total saturated fat’. The study contained flaws which included erroneously identifying a study examining omega-3 fatty acids to show a negative effect when in fact it had shown a strong positive effect. They also omitted two key studies on omega-6 fatty acids from their analysis. However, the main issue was that the studies reviewed failed to take into account what people consumed when they reduced their saturated fat intake.5 A further study published in 2014 in the Open Heart journal also calls into question the value of low saturated fat diets but incorrectly declares that current UK dietary guidelines encourage the replacement of saturated fats with carbohydrates.6 This is untrue and the guidelines make no such statement.1 It is important to note that no new evidence has actually been produced in any of the aforementioned recent publications. Nutritional science is complicated and multifaceted. This can therefore result in compelling arguments regarding the effect of dietary components on health and CHD risk. However, recent studies contradict 50 years of evidence-based practice despite there being an undisputed link between high levels of saturated fat consumption and LDL cholesterol levels.14 Researchers will often try to pull apart nutrients in order to assess their individual health benefits. This often results in misleading guidelines as nutrients are rarely eaten in isolation. It is very difficult to measure the effect of diet on health and therefore draw solid conclusions from the data. Studies assessing diet are more challenging to conduct than drug trials, as ensuring that people stick to a prescribed diet is near impossible and carefully controlling the diet of thousands of people over many years would be unfeasible. Dietary assessment techniques often result in flawed data. A 24-hour dietary recall may not represent a ‘typical day’, but also people tend to underestimate their intake which also happens when an average dietary intake is asked for. Food frequency questionnaires only list a certain number of foods so therefore are unlikely to represent all foods consumed for all participants. Dietary assessments are performed at the beginning of studies but people change their dietary habits over time.9 Many of the studies included in the meta-analysis did not take into account what people consumed in place of COPYRIGHT © 2015 JOHN WILEY & SONS Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ Foodstuff Calories (kcal) Saturated fat (g) Total calories (kcal) Total saturated fat (g) Full fat versions 20g butter 300ml full-cream milk 30g cheddar cheese 148 198 125 11 8 6 471kcal 25g Low fat versions 20g low-fat spread 300ml skimmed-milk 30g half-fat cheddar 56 96 82 1 0 4 234kcal 5g 237kcal 20g Difference Table 1. The calorie and saturated fat savings that could be made by switching from high fat dairy products to low fat alternatives19 Food Low fat alternative Calorie saving (kcal) Saturated fat saving (g) 35g sugar coated cereal with 100ml whole milk 25g porridge oats with 200ml skimmed milk 35 3 Apple Danish Slice of toast with jam and margarine 186 5 Chocolate muffin Slice of malt loaf 315 11 Bakewell tart 160g cherries 128 5 Beef burger – grilled Roast beef – 75g 159 7 Chicken Kiev Chicken breast – 95g 207 8 130g battered fish Baked cod/haddock – 125g 154 5 168g deep fried chips 195g boiled new potatoes 330 4 120g potato salad (with mayo) 160g sweet potato mash 210 5 50g milk chocolate Banana 179 9 4 chocolate digestives 125g natural yoghurt, 140g strawberries 59 8 Croissant Slice of granary bread with 5g light margarine 98 5 Chocolate cornflake cake 30g cornflakes with 100ml skimmed milk 104 6 80g apple pie 30g dried apple rings 143 3 50g tortilla chips 30g dried fruit and nuts 97 1 Table 2. Examples of the calorie and saturated fat savings that could be made by switching from high fat processed foods to low fat alternatives19 saturated fat. It is possible that numerous people may have increased their intake of refined carbohydrates which in turn may increase their risk of CHD. Current advice Current advice remains to state that we should consume no more than 10% of energy from saturated fat. Saturated fat should be replaced with unsaturated fats, particularly monounsaturated fats not carbohydrates.15 This comes from evidence collected from various randomised controlled trials. For example the RISCK trial analysed results from 548 participants over a six-month period. They concluded that total cholesterol and LDL PRACTICAL DIABETES VOL. 32 NO. 7 cholesterol levels were significantly lower after consumption of a low saturated fat diet in comparison to a control group.16 In 2009, a meta-analysis was carried out looking at 16 studies which modified the amount of saturated fat consumed. Results showed that in the studies where serum cholesterol was reduced by replacing saturated fat with polyunsaturated fat myocardial infarction rates and deaths from CHD were significantly reduced.17 The year 2015 has seen the publication of a Cochrane Collaboration systematic review which concluded that cardiovascular events could be reduced by 17% by reducing saturated fat consumption by lowering and/or modifying fat intake.18 COPYRIGHT © 2015 JOHN WILEY & SONS 259 Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ What also needs to be considered is that foods containing high levels of saturated fat also contain numerous calories. Table 1 shows the calorie and saturated fat savings that could be made by switching from high fat dairy products to low fat alternatives.19 Considering the current obesity epidemic, a reduction in calories consumed can only be a positive result and therefore this alone has to be one of the leading influences for continuing with current dietary guidelines. What to eat in place of saturated fat? Recent studies reporting that saturated fat has been falsely vilified have been embraced by the media and have led to newspaper headlines such as ‘Butter is NOT bad for you’ and ‘Saturated fat is ok after all’. This is likely to lead to confusion and will possibly result in an increase in consumption of high fat processed foods. One of the most important things to consider when reducing any nutrient in the diet is what is eaten in its place. Replacing saturated fat with refined carbohydrates has potentially negative side effects and can result in insulin resistance and dyslipideamia.5 In 2009, Jakobsen et al. showed that substitution of saturated fat with polyunsaturated fat resulted in a significant reduction in coronary heart disease risk whereas exchanging it for carbohydrates resulted in a modest increase in risk.20 A meta-analysis carried out by Mozaffarian et al. in 2010 found a significant reduction in risk of CHD events where a reduction in saturated fat was accomplished by substitution primarily with polyunsaturated fat.21 We should be aiming to decrease overall energy intake by reducing the amount of high fat processed foods we consume. See Table 2 for examples.19 Conclusion Dietary recommendations will not fit all individuals when taking into account disease status, age and activity levels. In those with diabetes, the reduction in amounts of carbohydrate foods consumed may be beneficial; however, these should not be replaced with saturated fats, but rather monounsaturated fats, lean protein foods and vegetables. Advice continues to suggest limiting foods which contain high levels of saturated fat, particularly meat products, and swapping these for foods rich in unsaturated fats, such as fish and nuts. Diets which are known to be cardio-protective – including the Mediterranean diet, a vegetarian diet and the DASH diet (Dietary Approaches to Stop Hypertension) – all advocate a low intake of saturated fat. A diet focused on fruit, vegetables, legumes, nuts and whole grains will have limited space for saturated fats. However, when considering weight control, it is important to remember that even monounsaturated fats are high in calories. Just because a diet is low in fat does not mean it needs to be high in carbohydrate. Moderation is key and focusing on overall intake is essential. Dietary intake is an individual choice but I for one will not be increasing the saturated fat content of my diet in light of this ‘new’ research! Declaration of interests There are no conflicts of interest declared. References References are available in Practical Diabetes online at www.practicaldiabetes.com. POEMs In T2DM, intensive glucose control modestly reduces CV events, but not mortality, after 10 years Clinical question Are there long-term benefits to more intensive glycaemic control in patients with type 2 diabetes? Reference Hayward RA, et al., for the VADT Investigators. Followup of glycemic control and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015;372(23):2197–206. Synopsis The Veterans Affairs Diabetes Trial (VADT) originally randomised 1791 veterans with type 2 diabetes mellitus to receive intensive or usual glycaemic control, and achieved mean HbA1c levels of 6.9% and 8.4%, respectively, after a median of 5.6 years. The original trial found a non-significant trend toward fewer cardiovascular events in the intensive therapy group, but no change in mortality. Two other large, similar trials reported similar findings, although one found increased mortality in the 260 PRACTICAL DIABETES VOL. 32 NO. 7 intensive glycaemic control group. Follow-up studies for these two other trials have had mixed results, one finding increased mortality and no change in events, with the other finding fewer events but no change in mortality. The current study linked patients in the original VADT to national disease registries (92% of participants) and also to regular record reviews and surveys (77% agreed to participate). The median follow up was 9.8 years for cardiovascular events and 11.8 years for assessment of total mortality. They found a small but statistically significant reduction in the primary combined outcome of myocardial infarction, stroke, new or worsening heart failure, cardiovascular death, or amputation (44.1 versus 52.7 per 1000 person-years; p=0.04). There was no significant difference between groups in the likelihood of cardiovascular death or all-cause mortality. The greatest contribution to the reduction in cardiovascular events was fewer non-fatal myocardial infarctions. COPYRIGHT © 2015 JOHN WILEY & SONS Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ For Dr Trudi Deakin, X-PERT Health (registered charity), Hebden Bridge, West Yorkshire, UK References 1. Diabetes UK. Are diabetes services in England and Wales measuring up? A summary of findings from the National Diabetes Audit 2011–12 for people with diabetes and anyone interested in the quality of diabetes care. https://www. diabetes.org.uk/Upload/Professionals/Service%20improvement/NDA%20201112%20Summary_Report_printer-ready.pdf [accessed 9 June 2015]. 2. Hite AH, et al. In the face of contradictory evidence: report of the Dietary Guidelines for Americans Committee. Nutrition 2010;26(10):915–24. 3. Ravnskov U. Is atherosclerosis caused by high cholesterol? QJM 2002; 95(6):397–403. 4. Shekelle RB, et al. Diet, serum cholesterol, and death from coronary heart disease. The Western Electric study. N Engl J Med 1981;304(2):65–70. 5. Nichols AB, et al. Daily nutritional intake and serum lipid levels. The Tecumseh study. Am J Clin Nutr 1976;29(12):1384–92. 6. Mensink RP, et al. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a metaanalysis of 60 controlled trials. Am J Clin Nutr 2003;77(5):1146–55. 7. Howard BV, et al. Low-fat dietary pattern and risk of cardiovascular disease: The women’s health initiative randomized controlled dietary modification trial. JAMA 2006;295(6):655–66. 8. Wing RR, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med 2013;369(2):145–54. 9. Ulmer H, et al. Why Eve Is not Adam: Prospective follow-up in 149,650 women and men of cholesterol and other risk factors related to cardiovascular and all-cause mortality. J Women’s Health 2004;13(1):41–53. 10. Mann GV. Coronary heart disease – the doctor’s dilemma. Am Heart J 1978;96(5): 569–71. 11. Multiple Risk Factor Intervention Trial Research Group. Multiple risk factor intervention trial. Risk factor changes and mortality results. JAMA 1982;248(12): 1465–77. 12. Hooper L, et al. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev 2015;6:CD011737. doi: 10.1002/14651858.CD011737. 13. Schwingshackl L, Hoffmann G. Dietary fatty acids in the secondary prevention of coronary heart disease: a systematic review, meta-analysis and meta-regression. BMJ Open 2014; 4(4): e004487. doi: 10.1136/bmjopen-2013. 14. Chowdhury R, et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann Intern Med 2014;160(6):398–406. 15. National Advisory Committee on Nutritional Education (NACNE). A discussion paper on proposals for nutritional guidelines for health education in Britain. 1983. 16. Harcombe Z, et al. Evidence from randomised controlled trials did not support the introduction of dietary fat guidelines in 1977 and 1983: a systematic review and meta-analysis. Open Heart 2015;2(1):e000196. doi: 10.1136/openhrt-2014. 17. Health & Social Care Information Centre. Statistics on obesity physical activity and diet (England). 2014. 18. Diabetes UK. State of the Nation: Challenges for 2015 and Beyond. London: DUK, 2014. 19. Forsythe CE, et al. Comparison of low fat and low carbohydrate diets on circulating fatty acid composition and markers of inflammation. Lipids 2008;43(1):65–77. 20. Volk BM, et al. Effects of step-wise increases in dietary carbohydrate on circulating saturated fatty acids and palmitoleic acid in adults with metabolic syndrome. PloS one 2014;9(11):e113605. 21. Stary HC, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Arterioscler Thromb Vasc Biol 1995;15(9):1512–31. 22. Lammert F, Wang DQ. New insights into the genetic regulation of intestinal cholesterol absorption. Gastroenterology 2005;129(2):718–34. 23. Zhao B, et al. Hepatic overexpression of cholesteryl ester hydrolase enhances cholesterol elimination and in vivo reverse cholesterol transport. J Lipid Res 2008;49(10):2212–7. 24. Cuchel M, Rader DJ. Macrophage reverse cholesterol transport: Key to the regression of atherosclerosis? Circulation 2006;113(21):2548–55. 25. Okuda LS, et al. Advanced glycated albumin impairs HDL anti-inflammatory activity and primes macrophages for inflammatory response that reduces reverse cholesterol transport. Biochim Biophys Acta 2012;1821(12):1485–92. 26. Taskinen MR, Boren J. New insights into the pathophysiology of dyslipidemia in type 2 diabetes. Atherosclerosis 2015;239(2):483–95. 27. Meeusen JW, et al. Reliability of calculated low-density lipoprotein cholesterol. Am J Cardiol 2015;pii:S0002-9149(15)01337-5. doi: 10.1016/j.amjcard.2015.05.013. [Epub ahead of print]. 28. Superko HR, Gadesam RR. Is it LDL particle size or number that correlates with risk for cardiovascular disease? Current Atherosclerosis Reports 2008;10(5):377–85. PRACTICAL DIABETES VOL. 32 NO. 7 29. Chait A, et al. Susceptibility of small, dense, low-density lipoproteins to oxidative modification in subjects with the atherogenic lipoprotein phenotype, pattern B. Am J Med 1993;94(4):350–6. 30. Mathews SC, et al. Achieving secondary prevention low-density lipoprotein particle concentration goals using lipoprotein cholesterol-based data. PloS one 2012;7(3):e33692. 31. Lahdenpera S, et al. Regulation of low-density lipoprotein particle size distribution in NIDDM and coronary disease: importance of serum triglycerides. Diabetologia 1996;39(4):453–61. 32. Brunzell JD, et al. Lipoprotein Management in Patients With Cardiometabolic Risk: Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008;31(4):811–22. 33. Sachdeva A, et al. Lipid levels in patients hospitalized with coronary artery disease: an analysis of 136,905 hospitalizations in Get With The Guidelines. Am Heart J 2009;157(1):111-7 e2. 34. Lamarche B, et al. Small, dense low-density lipoprotein particles as a predictor of the risk of ischemic heart disease in men. Prospective results from the Québec Cardiovascular Study. Circulation 1997;95(1):69–75. 35. May HT, et al. A new ratio for better predicting future death/myocardial infarction than standard lipid measurements in women >50 years undergoing coronary angiography: the apolipoprotein A1 remnant ratio (Apo A1/ [VLDL(3)+IDL]). Lipids Health Dis 2013;12:55. 36. de Nijs T, et al. ApoB versus non-HDL-cholesterol: diagnosis and cardiovascular risk management. Crit Rev Clin Lab Sci 2013;50(6):163–71. 37. Ford ES, et al. Temporal changes in concentrations of lipids and apolipoprotein B among adults with diagnosed and undiagnosed diabetes, prediabetes, and normoglycemia: findings from the National Health and Nutrition Examination Survey 1988–1991 to 2005–2008. Cardiovasc Diabetol 2013;12:26. 38. Sniderman AD. The measurement of apolipoprotein B should replace the conventional lipid profile in screening for cardiovascular risk. Can J Cardiol 1992;8(2):133–8. 39. Malave H, et al. Evaluation of low-density lipoprotein particle number distribution in patients with type 2 diabetes mellitus with low-density lipoprotein cholesterol <50 mg/dl and non-high-density lipoprotein cholesterol <80 mg/dl. Am J Cardiol 2012;110(5):662–5. 40. Cromwell WC, et al. LDL particle number and risk of future cardiovascular disease in the Framingham Offspring Study – implications for LDL management. J Clin Lipidology 2007;1(6):583–92. 41. National Institute for Health and Clinical Excellence. Cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. July 2014. https://www.nice.org.uk/guidance/ cg181/resources/guidance-lipid-modification-cardiovascular-risk-assessment-andthe-modification-of-blood-lipids-for-the-primary-and-secondary-prevention-ofcardiovascular-disease-pdf [accessed 9 June 2015]. 42. Wägner AM, et al. Triglyceride-to-HDL cholesterol ratio in the dyslipidemic classification of type 2 diabetes. Diabetes Care 2005;28(7):1798–800. 43. Hanak V, et al. Accuracy of the triglyceride to high-density lipoprotein cholesterol ratio for prediction of the low-density lipoprotein phenotype B. Am J Cardiol 2004;94(2):219–22. 44. Cordero A, et al. Usefulness of triglycerides-to-high-density lipoprotein cholesterol ratio for predicting the first coronary event in men. Am J Cardiol 2009;104(10):1393–7. 45. Bittner V, et al. The triglyceride/high-density lipoprotein cholesterol ratio predicts all-cause mortality in women with suspected myocardial ischemia: a report from the Women’s Ischemia Syndrome Evaluation (WISE). Am Heart J 2009;157(3): 548–55. 46. Lamarche B, et al. Fasting insulin and apolipoprotein B levels and low-density lipoprotein particle size as risk factors for ischemic heart disease. JAMA 1998;279(24):1955–61. 47. Kronmal RA, et al. Total serum cholesterol levels and mortality risk as a function of age. A report based on the Framingham data. Arch Intern Med 1993;153(9): 1065–73. 48. World Health Organisation. WHO Global Infobase: Data For Saving Lives. https://apps.who.int/infobase/Indicators.aspx [accessed 9 June 2015]. 49. World Health Organisation. WHO Global Infobase: Data for Saving Lives. https://apps.who.int/infobase/Comparisons.aspx [accessed 9 June 2015]. 50. Miselli M-A, et al. Plasma triglycerides predict ten-years all-cause mortality in outpatients with type 2 diabetes mellitus: a longitudinal observational study. Cardiovasc Diabetol 2014;13(1):135. 51. Birkenfeld AL, Shulman GI. Nonalcoholic fatty liver disease, hepatic insulin resistance, and type 2 diabetes. Hepatology 2014;59(2):713–23. 52. Cummings MH, et al. Increased hepatic secretion of very-low-density lipoprotein apolipoprotein B-100 in NIDDM. Diabetologia 1995;38(8):959–67. 53. Cordain L, et al. The paradoxical nature of hunter-gatherer diets: meat-based, yet non-atherogenic. Eur J Clin Nutr 2002;56(Suppl 1):S42–52. 54. Gurven M, Kaplan H. Longevity among hunter-gatherers: A cross-cultural examination. Population Devel Rev 2007;33(2):321–65. 55. O’Keefe J, Cordain L. Cardiovascular disease resulting from a diet and lifestyle at odds with our Paleolithic genome: How to become a 21st-century hunter-gatherer. Mayo Clin Proc 2004;79:101–8. COPYRIGHT © 2015 JOHN WILEY & SONS 260a Debate ‘Saturated fat doesn’t increase coronary heart disease in people with diabetes’ 56. Department for Environment Food and Rural Affairs. Family Food 2013: Annual statistics about food and drink purchases in the UK. 2014. https://www.gov. uk/government/collections/family-food-statistics [accessed 9 June 2015]. 57. Department for Environment Food and Rural Affairs. National Food Survey: Household consumption of food from 1942 to 2000. http://webarchive.national archives.gov.uk/20130103014432/http://www.defra.gov.uk/statistics/foodfarm/ food/familyfood/nationalfoodsurvey/ [accessed 9 June 2015]. 58. Lopez-Garcia E, et al. Consumption of trans fatty acids is related to plasma biomarkers of inflammation and endothelial dysfunction. J Nutrition 2005;135(3):562–6. 59. Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med 2008;233(6):674–88. 60. Ramsden CE, et al. n-6 fatty acid-specific and mixed polyunsaturate dietary interventions have different effects on CHD risk: a meta-analysis of randomised controlled trials. Br J Nutr 2010;104(11):1586–600. 61. Ramsden CE, et al. Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. BMJ 2013;346:e8707. 62. Stanhope KL, et al. A dose-response study of consuming high-fructose corn syrupsweetened beverages on lipid/lipoprotein risk factors for cardiovascular disease in young adults. Am J Clin Nutr 2015;101(6):1144–54. 63. Le Stunff C, Bougneres P. Early changes in postprandial insulin secretion, not in insulin sensitivity, characterize juvenile obesity. Diabetes 1994;43(5):696–702. 64. Feinman RD, et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition 2015;31(1):1–13. 65. Volek JS, et al. Carbohydrate restriction has a more favorable impact on the metabolic syndrome than a low fat diet. Lipids 2009;44(4):297–309. 66. Mozaffarian D. Saturated fatty acids and type 2 diabetes: more evidence to reinvent dietary guidelines. Lancet Diabetes Endocrinol 2014;2(10):770–2. 67. Musunuru K. Atherogenic dyslipidemia: cardiovascular risk and dietary intervention. Lipids 2010;45(10):907–14. 68. Sanders FW, Griffin JL. De novo lipogenesis in the liver in health and disease: more than just a shunting yard for glucose. Biological Rev 2015; doi: 10.1111/brv.12178. [Epub ahead of print]. 69. Feinman R, Fine E. ‘A calorie is a calorie’ violates the second law of thermodynamics. Nutrition J 2004;3:9. 70. Bueno NB, et al. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. Brit J Nutr 2013; 110(7):1178–87. 71. Santos FL, et al. Systematic review and meta-analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors. Obesity Rev 2012; 13(11):1048–66. 72. Daley C, et al. A review of fatty acid profiles and antioxidant content in grass-fed and grain-fed beef. Nutrition J 2010;9(1):10. 73. Fuller NR, et al. The effect of a high-egg diet on cardiovascular risk factors in people with type 2 diabetes: the Diabetes and Egg (DIABEGG) study – a 3-mo randomized controlled trial. Am J Clin Nutr 2015;101(4):705–13. 74. Whigham LD, et al. Efficacy of conjugated linoleic acid for reducing fat mass: a meta-analysis in humans. Am J Clin Nutr 2007;85(5):1203–11. 75. Tong X, et al. Dairy consumption and risk of type 2 diabetes mellitus: a meta-analysis of cohort studies. Eur J Clin Nutr 2011;65(9):1027–31. 76. Assuncao ML, et al. Effects of dietary coconut oil on the biochemical and anthropometric profiles of women presenting abdominal obesity. Lipids 2009;44(7): 593–601. 77. Academy of Nutrition and-Dietetics. Academy Comments re The DGAC Scientific Report: May 8, 2015. www.eatrightpro.org/resource/advocacy/take-action/ regulatory-comments/dgac-scientific-report [accessed 9 June 2015]. Against 10. Colberg SR, et al.; American College of Sports Medicine; American Diabetes Association. Exercise and type 2 diabetes: American College of Sports Medicine and the American Diabetes Association: joint position statement. Exercise and type 2 diabetes. Med Sci Sports Exerc 2010;42(12):2282–303. 11. Van Horn L, et al. The evidence for dietary prevention and treatment of cardiovascular disease. J Am Dietetic Assoc 2008;108:287–331. 12. Marshall JA, Bessesen DH. Dietary fat and the development of type 2 diabetes. Diabetes Care 2002;25(3):620–2. 13. Sanders TA. Reappraisal of SFA and cardiovascular risk. Proc Nutr Soc 2013;72(4):1–9. 14. Heart UK. Statement on saturated fat. 2014. Available at: http://heartuk.org.uk/ latest-news/article/heart-uk-statement-on-saturated-fat [accessed 27 May 2015]. 15. Diabetes UK. Evidence based nutrition guidelines for the prevention and management of diabetes. London: Diabetes UK, 2011. 16. Jebb SA, et al.; RISCK Study Group. Effect of changing the amount and type of fat and carbohydrate on insulin sensitivity and cardiovascular risk: the RISCK (Reading, Imperial, Surrey, Cambridge, and King’s) trial. Am J Clin Nutr 2010;92(4):748–58. 17. Skeaff CM, Miller J. Dietary fat and coronary heart disease: summary of evidence from prospective cohort and randomised controlled trials. Ann Nutr Metab 2009;55:173–201. 18. Hooper L, et al. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev 2015;6:CD011737. doi: 10.1002/14651858.CD011737. 19. Cheyette C, Balolia Y. Carbs and Cals, 4th edn. London: Chello Publishing Ltd, 2013. 20. Jakobsen MU, et al. Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr 2009;89(5):1425–32. 21. Mozaffarian D, et al. Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials. PLoS Med 2010;7(3):e1000252. doi: 10.1371/journal. pmed.1000252. Leonie Garden, Senior Diabetes Specialist Dietitian, The James Cook University Hospital, NHS South Tees, Middlesbrough, UK References 1. National Advisory Committee on Nutritional Education (NACNE). A discussion paper on proposals for nutritional guidelines for health and education in Britain. 1983. 2. Keys A. Coronary heart disease in seven countries: the study program and objectives. Circulation 1970;41(4):1–8. 3. Keys A. Coronary heart disease in seven countries: summary. Circulation 1970;41(4):186–95. 4. Malhotra A. Saturated fat is not the major issue. BMJ 2013;347:f6340. doi: 10.1136/bmj.f6340. 5. Chowdhury R, et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis. Ann Intern Med 2014;160(6):398–406. 6. DiNicolantonio J. The cardiometabolic consequences of replacing saturated fats with carbohydrates or omega-6 polyunsaturated fats: do the dietary guidelines have it wrong? Open Heart 2014;1:e000032. doi:10.1136/openhrt-2013-000032. 7. Bahl R. The evidence base for fat guidelines: a balanced diet. Open Heart 2015;2:e00029. doi:10.1136/openhrt-2014-000229. 8. Thomas B, Bishop T. Manual of Dietetic Practice, 4th edn. Oxford: Blackwell Publishing, 2007. 9. Siri-Tarino PW, et al. Saturated fatty acids and risk of coronary heart disease: modulation by replacement of nutrients. Curr Atheroscler Rep 2010;12(6):384–90. doi: 10.1007/s11883-010-0131-6. 260b PRACTICAL DIABETES VOL. 32 NO. 7 COPYRIGHT © 2015 JOHN WILEY & SONS