Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
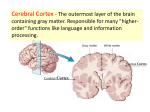
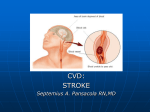
Cerebral Embolization: Prospective Clinical Analysis of 42 Cases BY JOHN STIRLING MEYER, M.D., JONATHAN Z. CHARNEY, M.D., VICTOR M. RIVERA, M.D., AND NINAN T. MATHEW, M.D. Abstract: Cerebral Embolization: Prospective Clinical Analysis of 42 Cases Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 • The sites, sources, and incidence of cerebral embolization were established in an unselected series of hospitalized patients using recommended epidemiological criteria. Criteria for diagnosis of cerebral embolization as a cause of stroke are defined. Forty-two (15%) from a total of 280 patients with various forms of cerebrovascular disease were diagnosed as having cerebral embolization. The epidemiology has been altered by antibiotics and cardiac surgery, particularly the use of prosthetic heart valves. In this series, the mortality rate was 9.5%, which is lower than in previously reported series probably due to emergency medical treatment. The heart was the most common source. Prosthetic heart valves emerged as the most common source of emboli in this scries. Ulcerated plaques of the carotid arteries in the neck ranked second. Seizures occurred in 42.8% of cases. The left cerebral hemisphere was involved approximately twice as frequently as the right one. Possible explanations based on the anatomy of the great vessels are described which predispose to embolization of the left carotid artery. Recommendations are suggested for preventing further embolization and for treatment of acute embolic cerebral infarction by the use of anticonvulsant drugs and hyperosmolar agents designed to reduce cerebral edema. cerebral emboli ADDITIONAL KEY WORDS papaverine diphenylhydantoin glycerol • Cerebral embolization has long been recognized as a common cause of death and disability; yet, surprisingly little has been written concerning its prevalence, diagnosis, and treatment because until recently clinical proof of its occurrence was often lacking. The potential epidemiological and therapeutic usefulness of case-fatality ratios in hospitalized populations, provided rigid criteria for case selection are used, has recently been reviewed.1 Development of arteriographical From the Department of Neurology, Baylor College of Medicine, and the Baylor-Methodist Center for Cerebrovascular Research, Houston, Texas. Supported by National Institute for Neurological Diseases and Stroke Grant No. NS 09287-01. Reprint requests to: Dr. lohn Stirling Meyer, Department of Neurology, Baylor College of Medicine, 1200 Moursund, Houston, Texas, 77025. Sfroke, Vol. 2, Novomber-D»cembor 1971 cerebral edema seizures prosthetic valve replacement techniques for visualizing obstruction of the cerebral arteries, and advances in surgical treatment such as carotid endarterectomy, prosthetic valve replacement, electronic pacemakers, and coronary bypass procedures, together with new methods of monitoring the electrocardiogram, have made it possible to distinguish cerebral embolism from other forms of cerebrovascular disease with considerable precision. For these reasons, few planned prospective clinical studies of the relative frequency, symptomatology, pathogenesis, and treatment of embolism in a large series of hospitalized patients suffering from stroke are cited in the literature. Available reports are almost invariably concerned with retrospective analysis of series of cases diagnosed at necropsy as embolism with retrospective inspection of 541 MEYER, CHARNEY, RIVERA, MATHEW Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 hospital records.2^* The single exception is the prospective study of a population group living in Framingham, Massachusetts.5 The Framingham study consisted of a population group of 5,106 adults without cerebrovascular symptoms followed for 12 years who were initially free of coronary heart disease and cerebrovascular disease. During this period, 11 of the 90 of this population later had strokes presumed to be due to cerebral embolism. In the Framingham study, the diagnosis of embolism was based, in the majority of cases, on clinical data without detailed ancillary diagnostic tests. The diagnosis of embolism in these cases was usually based on retrospective analysis of available clinical data provided by the patient's physician. Arteriograms were seldom carried out.1 Fisher et al.,8 in 17 of 57 brains studied at autopsy, reported infarction presumed to be due to cerebral embolism. The thought should be borne in mind that the diagnosis of cerebral embolism is often difficult to make on the basis of arteriographical findings during life since the embolus often becomes lysed or fragmented; hence, it is not surprising that these investigators failed to find the suspected embolism in the majority of cases. To overcome this difficulty, the majority of their diagnoses of cerebral embolism were based primarily on the hemorrhagic nature of the infarction. Castaigne et al.,4 in a similar autopsy series, used one or more of the following criteria for diagnosing cerebral embolism: (1) the lack of disease in the arterial wall at the site of occlusion, (2) identification of the probable source of the embolus, and (3) the presence of hemorrhagic infarction of the brain. Fisher et al.,8 in their necropsy study, employed one or more similar but not identical criteria: (1) the presence of embolic material in the occluded vessel, (2) atrial fibrillation prior to death, (3) acute myocardial infarction with mural thrombosis, (4) vegetative endocarditis, (5) recent surgical procedures on the heart or the great vessels supplying the brain, and (6) the presence of hemorrhagic cerebral infarction. As stated, their diagnosis of cerebral embolism was often based on an assumption, namely, criterion 6. Investigators who have made retrograde analyses from postmortem data agree that hemorrhagic infarction may be caused by factors other than 542 embolism. For this reason, in addition to the fact that all their patients expired, their autopsy statistics have limited epidemiological or therapeutic value. The present series of cases were analyzed prospectively using rigid clinical criteria.1 The majority of these patients survived and the data to be reported may be of interest from a case mortality and epidemiological point of view. For example, the information obtained from the study of these patients indicates that certain types of recurrent embolism are characterized by ischemia in the distribution of small cerebral vessels, resulting in transient or minimal neurological deficits which do not cause death or permanent disability, particularly if adequate treatment is instituted. Case Material and Experimental Design Prospective clinical analyses were carried out in 42 patients in whom the clinical diagnosis of cerebral embolism appeared to be well established (table 1). These patients were identified from a group of 280 with cerebrovascular disease examined over a period of 14 months by at least two of the authors in a large cerebrovascular research center. The diagnosis of cerebral embolism was based on the following clinical criteria: 1. In every case a probable or certain source of cerebral embolization existed including: (a) atherosclerotic or rheumatic heart disease with atrial fibrillation confirmed by cardiological consultation and electrocardiograms, supplemented as needed by coronary arteriograms and cardiac catheterization if the diagnosis was in doubt, (b) prosthetic valve replacement, (c) insertion of pacemakers for heart block due to myocardial infarction associated with mural thrombosis of the left side of the heart, (d) ulcerated atheromatous plaques or stenosis of the internal carotid artery proved arteriographically and confirmed by biopsy and microscopical examination of the surgical specimen, (e) vertebral stenosis with ulcerated atheromatous plaques demonstrated by arteriography only, and (f) aneurysms of the aortic arch with mural thrombi demonstrated angiographically. 2. In every case there was sudden onset of a focal neurological deficit, often preceded or accompanied by a seizure or seizures. 3. Demonstration of embolic occlusion of the suspected intracranial vessel by arteriography (26 cases). 4. Localized EEG abnormality consisting of slow waves or spike activity or both in the appropriate cerebral region supplied by the vessel Stroke, Vol. 2, November-Dtctmber 1971 CEREBRAL EMBOLIZATION TABLE 1 PoHant Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Ag. Sax 1 2 3 4 5 6 7 8 9 71 31 65 59 71 55 65 56 75 F M M F F F F M F 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 56 65 63 79 72 66 64 60 76 57 54 45 74 59 60 66 F M M M F M M M M M M M M M M M 26 47 M 27 86 M 28 29 18 67 F M 30 31 32 33 34 64 48 65 23 23 M M M F M 35 61 M 36 37 38 39 40 57 81 76 63 67 M M M M F 41 42 46 67 M M Sourc* of •mboll L carotid plaque Cardiac dysrhyttimia L carotid plaque L carotid plaque Atrial fib. RHD R carotid stenosis Ml mural thrombosis R carotid plaque (ULC) Ml heart block, pacemaker failure L carotid plaque Plaque RHD, pros, valve (A) Ml atrial fib. Ml heart block, pacemaker L carotid plaque Pros, valve (AJ L carotid plaque (ULC) Ml, ASHD, fib. R carotid plaque Pros, valve (M) Carotid plaque, kink L carotid plaque Pros, valve (A) Pros, valve (M) Pros, valve (M) Pros, valve (A) Pros, valve (M) Pros, valve (A) Bilateral carotid plaques (ULC) Pros, valve (M) Mural thrombosis A arch aneurysm Ml, dysrhythmia L carotid plaque R carotid plaque Pros, valve (M) Pros, valve (A) Pros, valve (M) Mural thrombosis A arch aneurysm L carotid plaque (ULC) R carotid plaque R carotid plaque RHD, mitral stenosis Vert, artery occlusion with embolization Pros, valve (A) L carotid plaque (ULC) Location of vmboD L hemisphere L hemisphere L hemisphere L hemisphere L hemisphere R hemisphere R hemisphere R hemisphere L hemisphere Stuporous Obtunded Alert Lethargic Lethargic Alert Stuporous Alert Lethargic L hemisphere L hemisphere L hemisphere L hemisphere L hemisphere L hemisphere L hemisphere L hemisphere L hemisphere R hemisphere R hemisphere R hemisphere L hemisphere L hemisphere L hemisphere R hemisphere Alert Lethargic Alert Alert, aphasic Lethargic Confused Dysphasic Alert, dysphasic Lethargic Lethargic Lethargic Dysphasic Dysphasic, alert Postictal Lethargic Obtunded R hemisphere Alert R and L hemispheres L hemisphere L hemisphere Alert R hemisphere L hemisphere R hemisphere L hemisphere R and L hemispheres L hemisphere Lethargic Obtunded Alert Alert Comatose L hemisphere R hemisphere R hemisphere L hemisphere R hemisphere Alert Comatose Alert Alert, dysphasic Drowsy L hemisphere L hemisphere Alert Asphasic Dysphasic Lethargic Coma M = male; F = female; L = left; R = right; (A) = aorta; (M) = mitral; Vert. = vertebral; RHD = rheumatic heart disease; (ULC) = ulcerated plaque found at surgery; MI := myocardial infarction; Pros. = prosthetic; ASHD = arteriosclerotic heart disease. Strok; Vol. 2, Nov»mfaer-D«cemfa«r 1971 543 MEYER, CHARNEY, RIVERA, MATHEW two who were seen within 48 hours of onset. Severely ill patients were admitted or transferred to the intensive care units of The Methodist Hospital where blood pressure, electrocardiograms, blood gases, and electrolytes were monitored. Detailed records were kept from September, 1969, through November, 1970 (14 months), of 280 otherwise unselected consecutive patients admitted or treated by the authors with all types of cerebrovascular disease. Fifteen percent of the patient population were Negro, 84% white, and 1% Asian Indian. The criteria cited for admission to the study with a diagnosis of embolism were employed within two days of hospitalization. Forty-two (15%) of the patients met the criteria cited and were diagnosed as having cerebral embolism (tables 1-5). In 43% of cases, the neurological deficit was preceded or accompanied by a seizure (table 6). In the majority of patients, occlusion of the vessel thought to be embolized was confirmed by arteriography (table 3). In all those in whom EEGs were recorded, focal abnormality was observed in the area supplied by the vessel thought to be involved, and in many the brain scans showed an abnormal uptake of radioisotope in the same areas. A few patients had multiple episodes of cerebral embolization, and in a few others embolism took place in other parts of the body. The remainder of the 280 patients suffered from acute signs and symptoms due to cerebral thrombosis, intracranial hemorrhage, and subarachnoid hemorrhage. Complete medical, cardiological, and neurological examinations were performed in all patients. The most frequently observed neurological sign in patients with cerebral embolism was asymmetrical deep tendon reflexes (83.3%) (table 2). Motor deficits consisting of hemiparesis or hemiplegia were present in 73.8%, and the cranial nerves were involved in 71.4% (fig. 1). Homonymous hemianopia was observed in 23.8% of those with cranial nerve involvement and was attributed to the high frequency of lesions at the junction of the middle cerebral and posterior cerebral arteries. The sensory examination was abnormal in 42.9% of these patients. TABLE 2 Abnormal Neurological Findings Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Abnormal tendon jerks Motor Cranial nerve involvement Second Homonymous hemianopia Monocular blindness Fifth Seventh Ninth, tenth Twelfth Extensor plantar response Disturbed consciousness Sensory Numbtr Percent (41 tat..) 35 31 30 83.33 73.80 71.40 10 4 7 20 2 2 25 29 18 23.80 9.50 16.70 47.60 4.80 4.80 59.50 69.00 42.90 considered to be occluded by the embolus (27 cases). 5. An abnormal uptake of technetium in brain scans in the area thought to be infarcted (ten cases). 6. Evidence of multiple cerebral embolic episodes (nine cases). 7. Evidence of embolism to other parts of the body (three cases). All of the patients examined were admitted to the Baylor-Methodist Center for Cerebrovascular Research or were seen in neurological consultation on the medical and cardiovascular services of The Methodist Hospital and treated by the authors in collaboration with the referring physicians.* Two or more of these criteria were present in each patient (tables 1-6). All patients were examined within 24 hours of the onset of symptoms with the exception of •The following persons kindly cooperated: Dr. Michael E. DeBakey, Dr. E. Stanley Crawford, and Dr. James Alexander, Baylor College of Medicine, Houston, Texas; Dr. John Oschner, the Oschner Clinic, New Orleans, Louisiana; and Dr. H. S. Roane, the Green Clinic, Ruston, Louisiana. TABLE 3 Laboratory Findings T*«t pmr1ormm4 Arteriogram Electroencephalogram Brain scan CSF pressure exceeding 180 mm H,O 544 No. cases •tadlod % Normal % Abnormal 28 30 11 7 10 9 93 90 91 20 50 50 Sfrokn, Vol. 2, Nov«mber-Dec«mb»r 1971 CEREBRAL EMBOLIZATION TABLE 4 Source* of Cerebral Embolization Porcvnt (41cu«) Nurabar of CCUM 1. Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Cardiac Prosthetic valves (75% RHD) Mitral stenosis (rheumatic heart disease) Arteriosclerotic heart disease Myocardial infarction Pacemaker failure Arrhythmias II. Carotid plaques (ulcerated) Right Left III. Carotid stenosis (nonulcerated) IV. Aortic aneurysms with mural thrombi V. Carotid kinking VI. Vertebral thrombosis with embolization Electroencephalography was performed in 30 patients, arteriography in 28, and brain scans in 11. Lumbar punctures were performed in half the patients (table 3). THERAPEUTIC MEASURES Therapy was instituted in all patients within 48 hours of the neurological deficit. Since seizures increase cerebral metabolism and are likely to worsen the neurological deficit or prove fatal in patients with heart disease, the 43% of patients 47.6 20 ii 26.2 l 2.4 14.3 6 7.1 4.8 2.4 % 2 1 33.3 14 S 9 4 2 1 1 11.9 21.4 9.5 4.8 2.4 2.4 who had seizures were treated with intramuscular diphenylhydantoin (100 mg three times daily) and phenobarbital (32 mg three times daily). Eighteen patients were given diazepam, 5 to 10 mg intravenously, which successfully arrested seizures immediately after administration. Two additional patients received oral phenobarbital and diphenylhydantoin prophylactically because of spike activity in the EEG and the assumption of imminent clinical seizures. In neither of these two patients did seizures occur. FIGURE 1 Microembolus of right retina from aortic valve prosthesis. The white, nonrefractile appearance is characteristic of platelet material. Sfrok*. Vol. 2, Novamb»r-0etember T97J 545 MEYER, CHARNEY, RIVERA, MATHEW TABLE 5 Sources and Sites of Cerebral Embolization (42 Cases) Numbar Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Total (all sources) Left hemisphere Right hemisphere Bilateral Cardiac origin Left hemisphere Right hemisphere Bilateral Carotid plaque origin Left hemisphere Right hemisphere Bilateral Porcant (41 casai) 27 13 2 64 31 5 13 4 3 65 20 15 9 5 0 64 36 0 percent received papaverine hydrochloride intramuscularly in doses of 60 mg every six hours for five days or 450 mg daily by mouth in order to increase the cerebral collateral circulation to the infarcted area.8 Ten percent were treated with low molecular weight dextran.6 All patients with embolism from prosthetic heart valves (26%) were treated with dipyridamole, 100 mg four times daily, since this drug has been shown to be effective in preventing further embolization. Anticoagulants were not used during the first three weeks of the acute ictus because of the danger of increasing the risk of cerebral hemorrhage. Anticoagulants had been used in the management during the chronic stage in patients with recurrent cerebral embolism due to valvular heart disease and prosthetic replacements. Results Forty-three percent of patients were treated with continuous or intermittent inhalation of 40% to 100% oxygen since this minimizes anoxia in the ischemic brain.0 In 38% intermittent 5% CO. plus oxygen inhalation was administered for 15 minutes every hour in order to enhance the cerebral collateral circulation and oxygen delivery to the ischemic zone.7 In an effort to reduce cerebral edema, 33% were treated for four days with 10% glycerol either intravenously (1.2 gm/kg of body weight daily) or orally (1.5 gm/kg of body weight daily).* Forty-three percent received dexamethasone, 12 mg intravenously, followed by intramuscular injection of 4 mg every four hours for five days to achieve the same end. Fifty-two *U.S.P. commercial laboratory glycerol was used. When given orally, it was mixed with orange or lemon juice for flavoring. The intravenous preparation was made by dissolving 50 gm of glycerol in 500 ml of commercially available 5% glucose or normal saline. The bottles were steam autoclaved for 20 minutes at 250° F in the HiVac autoclave on the liquid cycle without drying time. During autoclaving, the tops of the bottles were loosened and taped with masking autoclave tape. When the cycle was finished, the tops were tightened and sealed immediately. Commercially available intravenous Soluset plastic tubing was connected to an indwelling intravenous catheter. TABLE 6 Incidence of Seizures in 42 Cases of Cerebral Embolization Total with seizures Focal Generalized 546 18 14 4 (42.8%) (78.0%) (22.0%) The age and sex of 42 patients with cerebral embolism are shown in table 7. Men exceeded women by a ratio of approximately 3:1. The mean age for the males was 61 years and for the females 56 years. The mean age for the entire group was 60 years and the median age was 63.5 years. Thirty-nine of the patients with cerebral embolism were white, two were Negro, and one was an Asian Indian. This disproportionate ratio of Caucasian to Negro probably represents the higher incidence of hypertensive intracranial vascular disease in the Negro race and a higher incidence of extracranial ulcerative plaques in the carotid arteries in the white population. 10 ' 11 Six (14.2%) of the patients TABLE 7 Age and Sex Distribution Aga Mala Pemala 0 1 1 4 7 12 4 2 31 1 1 0 0 4 1 4 0 11 11-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90 Total Mean.Female Male Total 56.45 61.00 59.80 Total (parcant of 41) 1 2 1 4 11 13 8 2 42 Median-. Female Male Total (2.4) (4.8) (2.4) (9.5) (2.62) (31.0) (19.0) (4.8) 59 64 63.5 Stroka, Vol. 2, Novamber-Decamber 7971 CEREBRAL EMBOLIZATION LET v LT P - ^^^^A/\\yK^'^V^^\j^^^'^ RF-LF l5O I Sec FIGURE 2 Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 0/ patient with left focal seizures showing epileptogenic focus arising in right posterior quadrant of the head regions examined. were diabetic and 21 ( 5 0 % ) were hypertensive, which is a low incidence compared with cases of cerebral infarction due to thrombosis.8' 12 Probably the high incidence of embolism caused by rheumatic and valvular heart disease accounts for the difference.18 The electroencephalograms, brain scans, and arteriograms were abnormal in more than 90% of the patients tested (table 3 ) . Focal abnormalities were noted in the majority of EEGs (fig. 2) and in brain scans in areas diagnosed clinically as being infarcted. Arteriograms confirmed occlusion of the vessel thought to be occluded by embolization in 9 3 % of patients in whom the test was carried out (fig. 3 ) . In 50% of cases, the initial CSF pressure was more than 180 mm H 2 O, which was attributed to cerebral edema. Table 4 shows the sources of cerebral emboli in the present series of patients. The heart was the most common source (47.6%) followed by emboli from ulcerated plaques in the carotid arteries ( 3 3 . 3 % ) . Other sources were carotid stenosis without ulceration (9.5%) and aortic aneurysm with mural thrombi ( 4 . 8 % ) . Rare causes were carotid kinking due to atherosclerosis and proximal vertebral thrombosis. The majority of emboli ( 6 4 % ) lodged in the left cerebral hemisphere, 31 % were in the right hemisphere, and 5% were bilateral (table 5). When embolization was of cardiac origin, it appeared to have a predilection for the left hemisphere. In contrast, a high percentage Stroke, Vol. 2, Novembtr-December 1971 (although not all) of emboli from carotid plaques lodge in the ipsilateral hemisphere. CONVULSIVE SEIZURES DUE TO CEREBRAL EMBOLIZATION Eighteen (42.8% ) of the patients in our series with cerebral embolization had convulsive seizures (table 6 ) , the majority ( 7 8 % ) of which were focal seizures of the Jacksonian type. The remainder were generalized. This incidence of seizures is four times higher than that reported by Dodge et al.,14 in a retrospective analysis of autopsied cases of cerebrovascular disease. In all patients with seizures, this was the first evidence of neurological deficit. In a few patients, seizures recurred after a three-week interval, but one patient had recurrent seizures after six weeks and another one at 12 months following the embolic episode. In the latter two patients, the seizures coincided with withdrawal of anticonvulsive drugs. Discussion The reported incidence of cerebral embolism as a cause of stroke found at autopsy or from clinical evaluation without benefit of electrocardiography, EEG, and brain scan varies from a low of 8% reported by Carter15 in a retrospective study of patients with cerebrovascular disease to 46% observed by Jorgensen and Torvik 10 and 50% reported by Adams and Vander Eecken. 17 The latter two studies were based on autopsy findings in which hemorrhagic infarction was the main criterion. In another autopsy series in which rigid criteria 547 MEYER, CHARNEY, RIVERA, MATHEW Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 FIGURE 3 Carotid arteriogram showing occlusion of the left middle cerebral artery from embolus arising from mural thrombosis of the heart after pacemaker was inserted for complete heart block resulting from myocardial infarction. other than hemorrhagic infarction were used,18 the incidence was only 8.7%. Kannel et al.6 provided the only available prospective study of a population group and reported an incidence of 15% of strokes due to cerebral embolism, which is identical with the incidence in our selected series of hospitalized patients suffering from all types of stroke in which the embolic nature was confirmed using the criteria described. Males predominated in our study, and 548 other studies have also shown a male preponderance of cerebral embolism,19 although Kane and Aronson 18 and Kannel et al. s found a higher female incidence. In the productive years of life (before age 65) incidence of arteriosclerotic disease of the intracranial and extracranial vessels is highest in males. After the age of 65 and the menopause, the incidence of cerebrovascular disease is higher in females than in males.10 In the present series, rheumatic heart disease was a major cause of cerebral Stroke, Vol. 2, Novemb«r-O«c«mber 7971 CEREBRAL EMBOLIZATION FIGURE 4 Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Photograph of a variant ball valve inside the cage (a) and out of the cage (b). The patient had numerous episodes of platelet emboli (two to the right and three to the left cerebral hemisphere) which were treated with dipyridamole. This valve was replaced by Dr. E. Stanley Crawford because of the possibility of "sticking" in the cage. Since surgical replacement four months ago, the patient has been asymptomatic. Note the platelet depositions and the swollen, irregular surface. Also note the fibrous overgrowth around the seating of the valve cage. (This photograph was kindly made available by Dr. Crawford.) embolism and the incidence was highest in females. The finding that the heart is the most common source of emboli is in agreement with all other prospective studies;11 however, the development of improved surgical techniques for patients with chronic rheumatic heart disease has resulted in changes in the epidemiology of cerebral embolism. Prosthetic heart valves now have become the most common source of cerebral embolization. Rheumatic valvular disease usually with prosthetic replacement of diseased valves was the source of embolization in more than half of the patients with cerebral emboli of cardiac origin. This is in contrast with the series of patients reported ten years ago by Carter18 and others 20 in whom untreated rheumatic valvulitis was the most common cause of cerebral embolization. The prophylactic use of antibiotics in treating rheumatic heart disease brought about a reduction in incidence of this disorder as well as subacute bacterial endocarditis as a cause of stroke,12 but now that chronic cases are being treated by inserting prosthetic valves it is again becoming a common source of cerebral emboli. In our series, prosthetic aortic valves were the source in 22% and prosthetic mitral valves in 44% of patients with cerebral emboli of cardiac origin. Ball valve variance occurs most commonly in the aortic prosthetic valves, Stroke, Vol. 2, Novemb«r-D»ctmb»r 7971 presumably due to the high pressure in this system which causes distortion and lipid and platelet deposition on the ball of the valve.21-2This was particularly true of the early silastic ball valves of the Starr-Edwards type. In one patient, not included in this series, with cerebral embolism in whom the valve was replaced because of repeated small vessel emboli, white deposits having a thorny, linear appearance were observed on the circumference of the valve (fig. 4 ) . These appeared to be due to aggregated platelets and did not have the characteristic appearance of red organized thrombus which tends to occur soon after insertion of the valves, usually at the site of the suture line to the myocardium or on the cage of the valve. An example of a ball from a valve is shown in figure 5 on which may be seen white platelet deposits. From a neurological and therapeutic point of view, emboli from prosthetic valves cause two distinctly different types of cerebral embolization: 1. Recurrent small cerebral emboli, best illustrated in case No. 20 in this series. Four small cerebral emboli had lodged in the left hemisphere and three in the right hemisphere in this patient. In patients with emboli of this type, the neurological symptoms consist of typical transient ischemic attacks of less than 24 hours' duration with hemiparesthesias, 549 MEYER, CHARNEY, RIVERA, MATHEW FIGURE 5 Aortic valve showing variance removed from a patient on February 5, 1971. The prosthetic valve had been originally inserted on April 1, 1966. Irregular lipid deposits can be seen on the valve (arrows). (Obtained through the kindness of Dr. George Magovern, Allegheny General Hospital, Pittsburgh, Pennsylvania.) Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 hemiparesis, and minor episodes of dysphasia. These episodes may or may not be associated with ball valve variance, and in several of our patients murmurs of the type due to insufficiency of the prosthetic valve were not present. These small platelet emboli tend to occur three to five years after insertion of the StarrEdwards type of ball valve, particularly those fabricated from silastic material. Such emboli are believed to be fibrinoplatelet in nature, and dipyridamole appears to be more effective in their prevention than anticoagulant therapy alone.28 2. Larger cerebral emboli, which cause more severe and persistent neurological deficits that last for weeks with incomplete recovery, are believed to be due to dislodged fragments of red thrombus from accumulations on the cage of the valve or at its seating in the myocardium. They occur most commonly during the immediate postoperative period and, in rare instances, three to five years later when granulation tissue invades the struts of the cage. Anticoagulant therapy is useful in this group of patients. This was found to be the case in one of our patients not included in the present series in whom the valve was removed and replaced due to cerebral embolism with a protracted neurological deficit. Following replacement of the valve in this patient, there have been no further neurological symptoms. Cardiac dysrhythmias occurred in the vast majority but not all of our patients with cerebral embolism of cardiac origin. Atrial fibrillation occurred in 8 5 % , but regular sinus 550 rhythm was present at the time of embolization in 15%. This conclusion was based not only on physical examination and repeated electrocardiograms but also on EEG monitoring in the intensive care unit. There is no doubt that cerebral embolization of cardiac origin is usually associated with cardiac dysrhythmia; however, it should be stressed that cerebral embolization may occur in rare instances when the sinus rhythm is normal, e.g., following myocardial infarction or prosthetic replacement of a diseased valve. While it could be argued that a brief episode of fibrillation may have been missed at the time of embolism, this seems unlikely since the ECG was continuously monitored in an intensive care unit. Recurrent small cerebral emboli from prosthetic valves occurred in 11 of our patients who were on anticoagulant therapy. Institution of dipyridamole therapy in those with recurring embolism, despite treatment with anticoagulants, was effective in decreasing the incidence of further neurological deficit due to embolization from prosthetic valves, even though anticoagulation therapy was discontinued. The results obtained with this drug thus tend to confirm the findings of Sullivan et al.,23 who found in a controlled study that the combination of dipyridamole and anticoagulants was more effective than anticoagulants alone and also suggested that dipyridamole alone without anticoagulants may be effective in preventing cerebral embolism of the platelet type from prosthetic valves. All of the present series of patients have been followed for six to 15 Strok; Vol. 2, November-December 797) CEREBRAL EMBOLIZATION Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 months, and none of those given large doses of dipyridamole, 100 mg four times daily, have had further cerebral embolic episodes. The incidence of cerebral emboli from mural thrombosis due to myocardial infarction reported by Carter16 was higher than in our series. As stated, cerebral emboli from this source tend to be large and produce a severe neurological deficit. It is doubtful that dipyridamole would prevent these large emboli of the red thrombus type. Unfortunately, anticoagulants are contraindicated during the acute stage (three weeks) of cerebral infarction because of the risk of intracranial hemorrhage. In such cases, anticoagulant therapy was delayed for three weeks and then instituted. Ulcerated atherosclerotic plaques at the bifurcation of the internal carotid artery were the second most frequent cause of cerebral embolization in our patients (33.3%). The presence of these lesions was confirmed in every case by arteriography and biopsy of the surgical specimen. Carotid endarterectomy now has been proved to be the most appropriate form of treatment in these patients to lessen both the risk of further embolization or death.11 The relatively low incidence of myocardial infarction as a source of cerebral embolism in the present series of patients is probably due to the increased incidence of cerebral emboli as a result of new techniques of treating heart disease such as insertion of prosthetic valves and pacemakers. Pacemakers are usually inserted in patients with heart block from myocardial infarction, and emboli from mural thrombi may be dislodged in the heart as the cardiac rate is changed. While these are lifesaving procedures, they still carry a calculated and acceptable risk of cerebral embolization which can be reduced by medical treatment. The left hemisphere was involved more frequently than the right one when emboli were of cardiac origin. Brain stem embolization occurred simultaneously with cerebral embolism in only two patients. Embolization of the vertebral and basilar arteries due to myocardial infarction without concurrent embolization of the carotid arteries may be a cause of cortical blindness due to "saddle embolism" of the basilar artery where it bifurcates into both posterior cerebral Strck; Vol. 2, Nov«mb«r-Dectmber 7977 arteries. This did not occur in a single patient in our series and is admittedly a rare complication.24' 25 The higher incidence of cerebral embolism via the left carotid artery compared to the right one has never been satisfactorily explained. Two factors are suggested which may account for this: (1) cerebral embolization of the left hemisphere, which is the dominant hemisphere in more than 90% of people, causes more pronounced, recognizable clinical signs and symptoms than embolization of the nondominant side. Hence, the patient is more likely to seek medical attention and the neurological deficit is more easily recognized, and (2) the innominate artery usually arises at an oblique angle from the aortic arch, the angle being in the direction opposite the curvilinear trajection of the ejected bolus of blood with each systole (fig. 6), while the left common carotid artery normally rises vertically from the left side of the aortic arch. Hence, FIGURE 6 Diagram of aortic arch and major branches showing direction of blood flow after each systole. 551 MEYER, CHARNEY, RIVERA, MATHEW Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 emboli are more likely to pass through the latter vessel. Furthermore, if an embolus should enter the innominate artery, the trajectory of force in the reverse direction tends to direct it toward the subclavian rather than the carotid artery. In our view, the latter explanation seems the most important since all our patients had detailed neurological evaluations and it is doubtful that right hemispheric lesions were missed. Other investigators have confirmed the preponderance of left hemispheric infarction.18 Reports to the contrary are rare.15 The unusually high incidence of seizures (42.8%) as a manifestation of cerebral embolization found in our patients was striking, regardless of the source of emboli. A seizure, usually focal, involving the face, hand, and arm was frequently the initial symptom. Seizures of such a focal nature occurred in 78% of our patients; the remainder were generalized. Hence, seizures that occur as a manifestation of cerebrovascular disease should raise the question of embolism in the differential diagnosis of their cause. Such acute seizures were invariably controlled with intravenous diazepam and repeated seizures were prevented with diphenylhydantoin and phenobarbital. Rapid institution of therapy is undoubtedly lifesaving in patients with severe heart disease, particularly in the postoperative period. The importance of long-term anticonvulsive therapy was illustrated by two patients who had recurrent focal seizures several weeks or months after withdrawal of diphenylhydantoin and phenobarbital. In addition to controlling seizures and preventing further embolization, it seems logical that therapy should be directed toward reducing cerebral edema and promoting increased collateral blood flow to the infarcted area. Such therapy may decrease the size of the infarction, thereby enhancing the dissolution and removal of the embolic fragments. Regional edema was extensive enough in 50% of our patients to increase the intracranial pressure. Glycerol, 500 ml in 10% solution of saline, infused daily for four days was found to be extremely effective in reducing cerebral edema as judged by the clinical course of the patient and repeated measurement of CSF pressure. This innovation in therapy was believed to contribute to the low mortality rate of 9.5% (four of 42 patients) and rapid recovery in the 552 present series. Carter,20 in a series of patients with untreated cerebral embolism, reported that one-third (33.34%) died from the immediate effects of embolism. In another series, Carter11"' reported a higher incidence of myocardial infarction (31%) versus 14% as the cause of cerebral embolism. Although such differences in case series may influence case-mortality ratios, infarction of the brain was responsible for death in only 7% of the series reported in this communication. The other causes of death were cardiac in origin. The neurological deficits in the present series were comparable in severity with those found in other series. Harris and Levine27 also reported immediate mortality of one-third of their patients with cerebral embolism. Wells,28 in a series of patients with acute cerebral embolism, reported that 16 of 53 (30.84%) patients died as a result of embolism and its immediate complications. Whisnant,29 in a series of patients with cerebral infarction due to thromboembolism, reported an acute mortality rate of 27 %. Cerebrospinal fluid pressure was reduced in all four patients in whom lumbar puncture was repeated at the completion of treatment. In other patients with acute cerebral infarction not included in the present series, this form of therapy has resulted in a measurable increase in regional cerebral blood flow.80 Dexamethasone, although less effective than glycerol, has been shown recently to reduce cerebral edema and to improve the prognosis of stroke patients.S1'32 Low molecular weight dextran increases cerebral blood flow and oxygen delivery to infarcted brain presumably by decreasing cerebral edema and platelet adhesiveness.9 Intermittent inhalation of 5% CO2 in oxygen has been shown to increase regional cerebral blood flow in areas of infarction by increasing the collateral circulation.88'84 The effect of 5% CO2 inhalation in clearing the brain of fat emboli has been demonstrated clinically by Harnett et al.3B Likewise, papaverine administered by intramuscular or intravenous injection increases total and regional blood flow following hemispheric infarction and has been shown to decrease the mortality rate and improve the quality of survival in controlled clinical trials.8'36 It appears from the present clinical study that diagnostic methods are now available to Stroke, Vol. 2, Novemb*r-D*cembsr 1971 CEREBRAL EMBOLIZATION accurately diagnose cerebral embolization during life. Therapeutic measures are discussed which may prevent further cerebral emboli, reduce seizure activity which is common, and minimize the neurological deficit due to acute cerebral embolism. 14. 15. References 1. 2. 3. Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 4. 5. 6. 7. 8. 9. 10. 1 1. 12. 13. Borhani NO: Differences among hospitals in case-fatality ratios of cerebrovascular disease. Ann Int Med 72: 953-955, 1970 Wells CE: Premonitory symptoms of cerebral embolism. Arch Neurol 5: 490-496, 1961 Fisher CM, Gore I, Okabe N, et a l : Atherosclerosis of the carotid and vertebral arteries—extracranial and intracranial. J Neuropath Exp Neurol 4 : 455-476, 1965 Castaigne P, Lhermitte F, Gautier J-C, et a l : Internal carotid occlusion. A study of 61 instances in patients with post-mortem data. Brain 93: 231-258, 1970 Kannel WB, Dawber TR, Cohen ME, et a l : Vascular disease of the brain—epidemiologic aspects: The Framingham study. Amer J Public Health 55: 1355-1366, 1965 Meyer JS, Fang HC, Denny-Brown D: Polarographic study of cerebral collateral circulation. Arch Neurol Psychiat 72: 296-312, 1954 Gotoh F, Meyer JS, Tomita M : Carbonic anhydrase inhibition and cerebral venous blood gases and ions in man. Demonstration of increased oxygen availability to ischemic brain. Arch Int Med 117: 39-46, 1966 Meyer JS, Gotoh F, Gilroy J, et a l : Improvement of brain oxygenation and clinical improvement in patients with stroke associated with papaverine hydrochloride. JAMA 194: 957-961, 1965 Gilroy J, Barnhart M l , Meyer JS: Treatment of acute stroke with dextran 40. JAMA 210: 293298, 1969 Fields WS, North RR, Hoss WK, et a l : Joint study of extracranial arterial occlusion as a cause of stroke. I. Organization of study and survey of patient population. JAMA 203: 955968, 1968 Fields WS, Maslenikov V, Meyer JS, et a l : Joint study of extracranial arterial occlusion. V. Progress report of prognosis following surgery or nonsurgical treatment for transient cerebral ischemic attacks and cervical carotid artery lesions. JAMA 211:1993-2003, 1970 Meyer JS: Acute stroke; biochemical and therapeutic studies. Minn Med 47: 2 6 5 - 2 7 1 , 1964 Dyken M L : Precipitating factors, prognosis, and demography of cerebrovascular disease in an Indiana community. A review of all patients Sfroke, Vol. 2, November-December 1971 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. hospitalized from 1963 to 1965 with neurological examination of survivors. Stroke 1 : 2 6 1 269 (July-Aug) 1970 Dodge PR, Richardson ED, Victor M : Recurrent convulsive seizures as a sequel to cerebral infarction. Brain 77: 610-638, 1954 Carter AB: Immediate treatment of cerebral infarction. Seven years' personal experience. Lancet 1 : 3 4 5 - 3 5 1 , 1960 Jorgensen L, Torvik A : Ischaemic cerebrovascular diseases in an autopsy study. Part 1 : Prevalence, location, and predisposing factors in verified thrombo-embolic occlusions, and their significance in the pathogenesis of cerebral infarction. J Neurol Sci 3: 490-509, 1966 Adams RD, Vender Eecken H M : Vascular diseases of the brain. Ann Rev Med 4 : 213252, 1953 Kane WC, Aronson SM: Cardiac disorders predisposing to embolic stroke. Stroke 1 : 164172 (May-June) 1970 Leussenhop A J : Occlusive disease of the carotid artery. Observations on the prognosis and surgical treatment. J Neurosurg 16: 705730, 1959 Editorial: Neurological complications of infective endocarditis. Brit Med J 2 : 619, 1970 Lee SJK, Haraphongse M, Callaghan JC, et a l : Hemodynamic changes following correction of severe aortic stenosis using the Cutter-Smeloff prosthesis. Circulation 4 2 : 719-728, 1970 McHenry M M , Smeloff EA, Fong WY, et a l : Critical obstruction of prosthetic heart valves due to lipid absorption by silastic. J Thorac Cardiovas Surg 59: 413-425, 1970 Sullivan JM, Harken DE, Gorlin R: Effect of dipyridamole on the incidence of arterial emboli after cardiac replacement. Circulation 39 and 40 (suppl 1) : 1149-1153, 1969 Gilroy J, Meyer JS: Medical Neurology London, Macmillan Co, p 515-516, 1969 Loeb C, Meyer JS: Strokes Due to VertebroBasilar Disease. Infarction, Vascular Insufficiency and Hemorrhage of the Brain Stem and Cerebellum. Springfield, Illinois, Charles C Thomas, 1965 Carter AB: Prognosis of cerebral embolism. Lancet 2 : 514-519, 1965 Harris AW, Levine SA: Cerebral embolism in mitral stenosis. Ann Int Med 15: 637-643, 1941 Wells CE: Cerebral embolism; the natural history, prognostic signs and effects of anticoagulation. Arch Neurol Psychiat 81 : 661-611, 1958 Whisnant JP: Epidemiology of stroke in Rochester, Minnesota. American Heart Association, Joint meeting of the Council on 553 MEYER, CHARNEY, RIVERA, MATHEW Cerebrovascular Disease and the Council on Epidemiology on the Epidemiology of Cerebrovascular Disease, New Orleans, Louisiana, March 4, 1970 30. Mathew NT, Meyer JS, Ericsson AD, et a l : New method for measuring regional cerebral blood flow and blood volume -in man using the gamma camera. Trans Amer Neurol Assoc, in press, 1971 3 1 . Patten BM, Mandel J, Bruun B, et a l : Double blind study of the effect of dexamethasone on acute stroke. Neurology 2 1 : 403, 1971 (abstract) 32. Russek H I , Russek AS, Zohman BL: Cortisone in immediate therapy of apoplectic stroke. JAMA 159: 102-105, 1955 33. Cooper ES, West JW, Jaffe ME, et a l : Effect of CO2 inhalation on cardiac function and cerebral blood flow in stroke patients. Circulation 42 (suppl 3) : 120, 1970 (abstract) 34. Meyer JS, Fukuuchi Y, Kanda T, et a l : Regional measurements of cerebral blood flow and metabolism using intracarotid injection of hydrogen, with comments on intracerebral steal. In Ross Russell RW (ed) : Brain and Blood Flow. London, Pitman Medical and Scientific Publishing Co., p 71-79, 1971 35. Harnett RW, Lowe KG, Paterson JR, et a l : Treatment of cerebral-fat embolism. Lancet 2 : 762-764, 1959 36. McHenry LC Jr, Jaffe ME, Kawamura J, et a l : Effect of papaverine on regional blood flow in focal vascular disease of the brain. New Eng J Med 282: 1 167-1 170, 1970 Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 554 Strokm, Vol. 2, Novmbar-Dac»mber 1971 Cerebral Embolization: Prospective Clinical Analysis of 42 Cases JOHN STIRLING MEYER, JONATHAN Z. CHARNEY, VICTOR M. RIVERA and NINAN T. MATHEW Stroke. 1971;2:541-554 doi: 10.1161/01.STR.2.6.541 Downloaded from http://stroke.ahajournals.org/ by guest on June 12, 2017 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1971 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/2/6/541 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/