Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Oesophagostomum wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
Meningococcal disease wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Onchocerciasis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Schistosomiasis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Diagnosis of HIV/AIDS wikipedia , lookup
History of tuberculosis wikipedia , lookup
Leptospirosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
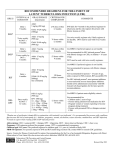
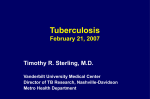
Pulmonary Board Review Tuberculosis Curtis M. Grenoble, MHS, PA-C Lock Haven University PA Program Fall 2008 Historical Perspective • During the 1800’s 1 in 5 persons in the US had active TB! • “captain of all men of death” – leading killer • 1985 there were 9.3 cases per 100,000 • Resurgence in early 1990’s – HIV, and public policy as well in the late 80’s • Now 7.4 cases per 100,000 Reported TB Cases* United States, 1982–2007 28,000 No. of Cases 26,000 24,000 22,000 20,000 18,000 16,000 14,000 12,000 10,000 1983 1986 1989 1992 1995 Year *Updated as of April 23, 2008. 1998 2001 2004 2007 No. of Cases Number of TB Cases in U.S.-born vs. Foreign-born Persons United States, 1993–2007* 20000 15000 10000 5000 0 1993 1995 1997 1999 2001 2003 2005 2007 U.S.-born *Updated as of April 23, 2008. Foreign-born Transmission of Tuberculosis Causative organism: Mycobacterium tuberculosis Aerosolized droplets containing MTB Persons at Risk • • • • • • • • • • HIV Homeless Live or work in crowded conditions Immigrants IVDA Prison Immunosuppresion for any reason DM Debilitation – ETOH HCW Purpose of Targeted Testing • Find persons with TB disease / LTBI that would benefit from treatment • Groups that are not high risk should not be tested DECISION TO TEST IS A DECISION TO TREAT! • • • • • • • • High Risk Groups: Close contacts of a person known or suspected to have TB Foreign-born persons of high incidence countries Residents and employees of high-risk congregate settings Health care workers (HCW) serving high-risk clients Medically underserved, low income populations Children exposed to adults in high-risk categories Persons who inject illicit drugs Persons with HIV / certain medical conditions How is the skin test read? • Test is read by a trained health worker 48 - 72 hours after the tuberculin injection • Diameter of the indurated area is measured transversely across the forearm • Erythema (redness) is not measured • Test result is measured in millimeters (mm) – ≥ 5mm: HIV+, recent TB exposure, x-ray evidence, immunosuppressed – ≥ 10mm: recent immigrants from high risk country, illicit drug users, HCW, correctional facilities, LTC facilities, DM CRF – ≥ 15mm: Persons with no known risk, HCW otherwise at low risk and received baseline testing at start of employment False Positive PPD Skin Tests • Error in administering the test • Cross-reaction with nontuberculous mycobacterial antigens • Any previous bacille Calmette-Guérin vaccination Delayed Positive Reaction • Booster phenomenon Latent Tuberculosis Infection LTBI Person: • Not acutely ill • Not contagious Germs: • “Sleeping” but still alive • Surrounded (walled off ) by body’s immune system In LTBI • TB germs are “sleeping” and body defenses are keeping them from growing • The TB skin test is usually positive • Chest x-ray = normal • Sputum culture = negative Isoniazid Regimens • INH daily for 9 months (270 doses within 12 months) • INH twice/week for 9 months (76 doses within 12 months) • INH daily for 6 months (180 doses within 9 months) • INH twice/week for 6 months (52 doses within 9 months) Isoniazid Regimens • 9-month regimen of INH - Preferred • 6-month regimen - less effective but is an alternative • Daily vs. intermittent (twice weekly) – Use directly observed therapy (DOT) for intermittent regimen • Completion of Therapy –Determined by total number of doses administered –Not on duration alone. Alternative Regimens: Rifampin • Rifampin (RIF) - daily for 4 months is an acceptable alternative when treatment with INH is not feasible. – Side effect • Rifabutin - alternative to Rifampin (e.g. - HIV-infected persons receiving protease inhibitors) Hepatitis Risk in LTBI Treatment • Incidence of hepatitis in persons taking INH is lower than previously thought (0.1 to 0.15%) • Hepatitis risk increases with age – Uncommon in persons < 20 years old – Nearly 2% in persons 50 to 64 years old • Risk increased with underlying liver disease or heavy alcohol consumption Laboratory Monitoring INH Patients • Baseline LFT’s • HCG, HIV, Hepatitis Panel, Etoh • Obtain repeat LFT’s during treatment only if patient becomes symptomatic, or if high risk for toxicity • Discontinue INH if transaminase levels are • • 3 times the upper limit of normal if symptoms of hepatotoxicity (rash, anorexia, N/V, RUQ pain, fatigue, weakness, dark urine, numb hands/feet) 5 times the upper limit of normal if patient is asymptomatic What causes TB infection to become TB disease? Wall breaks down due to a weakened immune system ~10% of those infected with develop disease over their lifetime TB disease Germs: • Awake and multiply • Cause damage Person: • May feel sick • May be contagious Symptoms of TB • Cough – Productive, lots of sputum – Persistent 3 weeks or longer – Coughing up blood or bloody sputum – Does not respond to other antibiotics Symptoms of TB • Fatigue • Weight loss (unexplained) • Loss of appetite • Night Sweats • Chest pain • (Constitutional symptoms) TB Disease in the Body Brain Eye Lymph node Throat Lung * (Most Common) Bone Spine Kidney Up to 40% of TB in children involves extrapulmonary sites (bones, LN, kidneys) Sputum Collection Sputum specimens essential to confirm TB • Sputum: mucus from within the lung, not saliva • 3 specimens on 3 different days • Spontaneous morning sputum • Positive (Acid-fast bacilli) – – – – Need at least 10,000 bacilli per ml Positive in about half those with TB disease Signal a very infectious person Others (mycobacterium avium) may produce “false positive” – Sputum culture (“Gold standard”) General Principles of TB Treatment • Always treat with multiple drugs • Never add a single drug to a failing regimen • Treatment course depends on drugs selected • Non-adherence • The single most important reason for tuberculosis treatment failure Anti TB Medications First-Line Second-Line • • • • • • Isoniazide INH Rifampin RIF Ethambutal EMB Rifabutin Pyrazinamide PZA Streptomycin • • • • • • • • Capreomycin Kanamycin Amikacin Ethionamide Para-aminosalicyclic Cycloserine Cipro Levofloxacin Resources for Health Care Providers • • • Centers for Disease Control and Prevention 1600 Clifton Rd. Atlanta, GA 30333 Telephone: 800-311-3435; 404-639-3311 Web site: http://www.cdc.gov National Jewish Medical and Research Center 1400 Jackson St. Denver, CO 80206 Telephone: 303-388-4461 Physician Consult Line (Monday - Friday, 8 a.m. to 5 p.m. MT): 800-652-9555 Web site: http://www.njc.org American Thoracic Society 1740 Broadway New York, NY 10019 Telephone: 212-315-8700 Fax: 212-315-6498 Web site: http://www.thoracic.org