Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
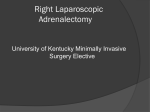
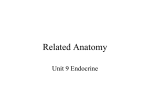
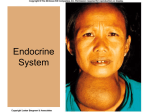
JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUES Volume 16, Number 5, 2006 © Mary Ann Liebert, Inc. Case Report Robot-Assisted Cortical-Sparing Adrenalectomy in a Patient with Von Hippel-Lindau Disease and Bilateral Pheochromocytomas Separated by 9 Years JAMII ST. JULIEN, MPH, DOUGLAS BALL, MD, and RICHARD SCHULICK, MD ABSTRACT Von Hippel-Lindau disease is a heritable syndrome that confers an increased risk of developing various benign and malignant tumors to those with a germline mutation of the tumor suppressor gene. We present a case of a male patient who initially presented at age 9 with headaches, fevers, and fatigue. He was found to have a left pheochromocytoma which was successfully managed with open total adrenalectomy. He presented again at age 18 with a second pheochromocytoma in the right adrenal gland. DNA analysis revealed a de novo Val84Leu mutation in the Von Hippel-Lindau gene, not seen in either parent. The challenge presented was that of balancing the obvious benefits of cortical-sparing adrenalectomy with the risk of tumor recurrence in spared tissue. Ultimately, management consisted of a robot-assisted laparoscopic partial right adrenalectomy with successful preservation of adrenocortical function. INTRODUCTION V HIPPEL-LINDAU (VHL) DISEASE is an autosomal dominant disorder characterized by benign and malignant tumors involving the central nervous system (CNS), kidneys, pancreas, adrenal glands, paraganglia, and reproductive adnexal organs (including epididymal and broad ligament cystadenomas). Inactivating mutations in the VHL gene lead to inappropriate accumulation of the hypoxia-inducible transcription factor (HIF1) and overabundance of a number of hypoxia-induced proteins involved in tumorigenesis.1 Pheochromocytomas, though rare, represent an important clinical manifestation of this syndrome that must be addressed promptly. We describe a patient with VHL who underwent two metachronous (separated by 9 years) procedures for ON adrenal pheochromocytomas involving both adrenal glands. The case is exceptional because it demonstrates the multidisciplinary approach necessary for the proper management of patients with VHL, the unique challenges presented by multiple adrenal tumors, and a novel approach to minimally invasive cortical-sparing adrenalectomy using the da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA). CASE REPORT A 9-year-old Caucasian male with a history of caféau-lait spots since birth, was referred to Johns Hopkins Hospital in 1993 for evaluation of a suspected pheochromocytoma. The patient reported four months of nighttime sweats, three weeks of fevers, bifrontal headaches, Department of Surgery, The Johns Hopkins University School of Medicine, Baltimore, Maryland. 473 474 ST. JULIEN ET AL. and fatigue. On admission the patient was hypertensive, tachycardic, and had an elevated 24-hour urine norepinephrine level of 1235 g (normal range, 11–86 g/24 hr). A magnetic resonance imaging (MRI) scan demonstrated a 3-cm left adrenal mass, and an I131 metaiodobenzylguanidine (MIBG) scintigraphy scan confirmed increased activity confined to the left adrenal gland (Figs. 1, 2). One month later, after being appropriately volume-resuscitated and premedicated with an alpha-blocker, the patient underwent an exploratory laparotomy and left adrenalectomy, with an uncomplicated postoperative course. The adrenalectomy was carried out using a left transverse incision, mobilizing the splenic flexure of the colon medially, and elevating the spleen and tail of the pancreas out of the retroperitoneum. The left adrenal gland was then resected in total by dividing the left adrenal vein and other structures attaching it to the kidney, aorta, and retroperitoneum. A 24-hour urine collection one month later revealed a norepinephrine level of 88 g, epinephrine of 18 g (normal range, 0–16 g/24 hr), and dopamine of 546 g (normal range, 100–440 g/24 hr)—all minimally elevated. The patient did well until 1997, when he again began to have bitemporal headaches, fatigue, and low-grade fevers. A 24-hour urine collection for catecholamines revealed an epinephrine level of 9 g, norepinephrine level of 57 g, and a total metanephrine level of 0.4 mg (normal range, 1.2 mg/24 hr). An abdominal MRI one month later did not reveal an obvious pheochromocytoma or paraganglioma. An MIBG scan at this time was also FIG. 1. Left adrenal pheochromocytoma in 1993. A: T1weighted axial magnetic resonance imaging (MRI) without contrast enhancement demonstrates a 3-cm mass in the left adrenal gland. B: T2-weighted axial MRI shows the brightness of the same mass. C: T2-weighted coronal MRI. FIG. 2. An I131 metaiodobenzylguanidine (MIBG) scintigraphy scan in 1993 demonstrating increased activity in the area of the left adrenal gland. ROBOT-ASSISTED ADRENALECTOMY IN VON HIPPEL-LINDAU 475 FIG. 3. Right adrenal pheochromocytoma in 2002. A: A T1weighted axial magnetic resonance imaging (MRI) with contrast demonstrates a 1.7 1.6 2 cm right adrenal mass. B: A T2-weighted axial MRI shows the brightness of the same mass. C: A T2-weighted coronal MRI. negative. In 1998, the patient’s symptoms worsened, but notably there was no hypertension. A repeat MRI scan still did not reveal any obvious recurrence, and an In111 pentetreotide scintigraphy (OctreoScan,, Mallinckrodt Inc., Hazelwood, MO) scan was also negative. The patient did not have any subcutaneous manifestations of neurofibromatosis (NF), and an ophthalmology evaluation noted the absence of Lisch nodules. There was also an absence of retinal angiomas, which are a manifestation of VHL. A DNA analysis demonstrated a conservative alteration in codon 84 (val-84-leu) of the VHL gene. The VHL Val84Leu mutation has been associated with a risk of pheochromocytoma, but low risk of renal cell carcinoma or CNS disease.2 The mother’s and father’s DNA analyses were both negative for mutations in the VHL gene. The patient was intermittently placed on phenoxybenzamine and labetalol, with significant improvement of his symptoms. Several subsequent MRIs failed to reveal any possible foci of pheochromocytoma or paraganglioma. In 2002, a routine MRI revealed a 1.7 1.6 2 cm right adrenal mass (Fig. 3). A 24-hour urine collection for catecholamines revealed elevated norepinephrine of 160 g and normetanephrine level of 679 g (normal range, 44–540 g/24 hrs). The epinephrine and metanephrine levels were too low to detect. The patient was asymptomatic at this time and off all antihypertensive medications. An MIBG scan showed increased up- take in the right adrenal gland with no evidence of extra-adrenal disease (Fig. 4). The patient was started on phenoxybenzamine. At this point a discussion was held with the family about the risk of recurrent tumors as well as the risks and benefits of partial versus total adrenalectomy, and it was agreed that the best course of action would be a partial adrenalectomy, if possible, with the goal of postponing lifelong steroid replacement therapy in a young, athletically active individual. Laparascopic robot-assisted partial adrenalectomy Three months later, a laparoscopic robot-assisted partial right adrenalectomy was performed. The patient was placed in the left lateral decubitus position on a beanbag. A 12-mm trocar was placed midway between the umbilicus and the right costal margin using the open Hasson technique. The peritoneal cavity was insufflated to 15 mm Hg with carbon dioxide and a limited adhesiolysis was performed in the right upper quadrant. Two 7mm ports were placed along the right costal margin for the robotic arms, a 10-mm liver retraction port was placed in the midline epigastrium through which an expanding fan was placed, and a 10-mm energy port was placed between the camera and the most lateral 7-mm port through which the LigaSure device could be placed. The fan retractor was used to elevate the liver out of the right sub- 476 ST. JULIEN ET AL. mg hydrocortisone once a day for three days, followed by 20 mg once a day for three days, and finally switched to 10 mg once a day. He also started fludrocortisone 0.1 mg once a day. One month postoperatively, after his morning dose of hydrocortisone was withheld, the patient’s basal cortisol level was 13.5 g/dL (normal range, 6–26 g/dL). However, an adrenocorticotropic hormone (ACTH) stimulation test (using 1 g ACTH) demonstrated a 30-minute peak cortisol level of 14.4 g/dL (normal response 18 g/dL). This indicated impaired adrenocortical reserve, and the patient was therefore maintained on replacement glucocorticoids and mineralocorticoids with a planned slow taper. The patient was advised to increase his hydrocortisone to 40 mg in the morning and 10 mg in the afternoon in case of serious stress such as fever, and was also given a prescription for 100 mg hydrocortisone injection in case of acute stress in order to prevent adrenal crisis. Over the course of the next year the patient was weaned off steroids, temporarily restarting them as needed during times of illness. The patient is now undergoing annual surveillance with history, physical examination, urine catecholamines, plasma metanephrines, and bilateral renal ultrasound, as well as slit-lamp examination every two years. FIG. 4. An I131 metaiodobenzylguanidine (MIBG) scintigraphy scan in 2002 demonstrating increased activity in the area of the right adrenal gland. diaphragmatic space and retroperitoneum. The entire right lobe of the liver was then mobilized out of the retroperitoneum and off the diaphragm using the hook cautery device. At this point the da Vinci surgical system was engaged to perform the rest of the dissection. The peritoneum covering the vena cava and the adrenal gland was then dissected. The right adrenal gland was easily located and the mass clearly seen at the level of the right adrenal vein as it entered the vena cava. The vein was encircled, four clips were placed, and the vein was divided. The retroperitoneal and renal attachments of the superior-lateral limb were then divided with the harmonic scalpel and electrocautery device. The adrenal gland was then transected with the harmonic scalpel just caudal to the mass, leaving the inferior-medial limb of the gland intact with its attachments (Fig. 5). The argon beam was used for hemostasis. The mass was removed through the energy port in an endobag without incident and the incisions were closed. The patient tolerated the procedure well. DISCUSSION VHL disease is a heritable multisystem syndrome that predisposes to the development of tumors involving the CNS, kidneys, pancreas, adrenal glands, paraganglia, and reproductive adnexal organs.1 The incidence of VHL is roughly one in 36,000 live births.3 It is inherited as an autosomal dominant trait and exhibits greater than 90% penetrance.3 The most common manifestations are retinal angiomas and CNS hemangioblastomas, as well as Postoperative course The patient had an uncomplicated postoperative course. Immediately postoperatively he was placed on 30 FIG. 5. Robot-assisted partial right adrenalectomy: the adrenal gland is transected with the harmonic scalpel just caudal to the mass. ROBOT-ASSISTED ADRENALECTOMY IN VON HIPPEL-LINDAU renal cell carcinoma.4 The frequency of pheochromocytomas in patients with VHL ranges between 7% and 16%.4,5 Pheochromocytomas (and functional paragangliomas) are particularly concerning because of the rapid and unanticipated release of catecholamines—sudden death is a major concern. Patients with VHL and pheochromocytoma require lifetime biochemical and clinical follow-up, even following total bilateral adrenalectomy, because of a significant risk of paraganglioma in this disorder. The first report of the preservation of adrenocortical function during surgery for bilateral pheochromocytoma was in 1982.6 Prior to this, the procedure of choice for these patients was an open total bilateral adrenalectomy. However, this led to much more difficult recovery periods, necessitated a lifetime of adrenocortical steroid replacement, and increased the frequency of potentially fatal Addisonian crises.7 Experience has since shown partial adrenalectomy to be a technically feasible and effective procedure: reports have documented that 20% of well-perfused adrenal cortical tissue from a single gland is sufficient to maintain an adequate stress response.8 Partial adrenalectomy is currently specifically recommended for patients with a single adrenal gland, bilateral adrenal tumors, or hereditary adrenal tumors. One group recommended it as the procedure of choice for hereditary pheochromocytomas;9 however, the pros and cons of the procedure should be carefully considered for each individual patient. The risks and benefits, as well as alternative treatment approaches, should be discussed in detail with the patient and the decision reached together. Partial adrenalectomies can be considered in appropriate cases and, if successful, do not require corticosteroid supplementation. In this case we used the da Vinci surgical system because of its superior visualization and increased dexterity. Since its introduction, early experience has suggested that the safety and efficacy of the da Vinci system is comparable to that of conventional laparoscopy.10,11 The system provides the surgeon with enhanced laparoscopic degrees of motion while also restoring the three-dimensional view lost in conventional laparoscopic surgery. In our literature search, we found no reports describing the use of the da Vinci surgical system for laparoscopic cortical-sparing adrenalectomy. We have demonstrated that it is a feasible, safe, and effective alternative to conventional laparoscopy. In our experience, the robotic system allows precise dissection of affected tissue 477 from the adrenal gland, leaving enough functional tissue intact to maintain adrenocortical sufficiency. REFERENCES 1. Lonser RR, Glenn GM, Walther M, et al. Von Hippel-Lindau disease. Lancet 2003;361:2059–2067. 2. Clifford SC, Cockman ME, Smallwood AC, et al. Contrasting effects on HIF-1 alpha regulation by disease-causing VHL mutations correlate with patterns of tumourigenesis in von Hippel-Lindau disease. Hum Mol Genet 2001;10:1029–1038. 3. Maher ER, Iselius L, Yates JR, et al. Von Hippel-Lindau disease: a genetic study. J Med Genet 1991;28:443–447. 4. Maher ER, Yates JR, Harries R, et al. Clinical features and natural history of von Hippel-Lindau disease. Q J Med 1990;77:1151–1163. 5. Baghai M, Thompson GB, Young WF Jr., Grant CS, Michels VV, van Heerden JA. Pheochromocytomas and paragangliomas in von Hippel-Lindau disease: a role for laparoscopic and cortical-sparing surgery. Arch Surg 2002;137:682–689. 6. Giordano WC. Preservation of adrenocortical function during surgery for bilateral pheochromocytoma. J Urol 1982;127:100–102. 7. Lairmore TC, Ball DW, Baylin SB, Wells SA Jr. Management of pheochromocytomas in patients with multiple endocrine neoplasia type 2 syndromes. Ann Surg 1993; 217:595–601. 8. Cedermark BJ, Sjoberg HE. The clinical significance of metastases to the adrenal glands. Surg Gynecol Obstet 1981;152:607–610. 9. Pavlovich CP, Linehan WM, Walther MM. Partial adrenalectomy in patients with multiple adrenal tumors. Curr Urol Rep 2001;2:19–23. 10. Horgan S, Vanuno D. Robots in laparoscopic surgery. J Laparoendosc Adv Surg Tech A 2001;11:415–419. 11. Undre S, Munz Y, Moorthy K, et al. Robot-assisted laparoscopic adrenalectomy: preliminary UK results. BJU Int 2004;93:357–359. Address reprint requests to: Richard Schulick, MD Department of Surgery The Johns Hopkins University School of Medicine 1650 Orleans Street CRB BLDG Room 442 Baltimore, MD 21231 E-mail: [email protected] This article has been cited by: 1. John J. Meehan. 2013. Robotic Surgery for Pediatric Tumors. The Cancer Journal 19:2, 183-188. [CrossRef] 2. Halit Eren Taskin, Eren Berber. 2013. Robotic Adrenalectomy. The Cancer Journal 19:2, 162-166. [CrossRef] 3. Giovanni Cochetti, Francesco D'Amico, Emanuele Cottini, Alberto Pansadoro, Francesco Barillaro, Emanuele Lepri, Ettore Mearini. 2012. Robotic Partial Adrenalectomy for 10-cm Angiomyolipoma. Journal of Laparoendoscopic & Advanced Surgical Techniques Part B, Videoscopy 22:6. . [Abstract] [Full Text HTML] 4. Halit Eren Taskin, Eren Berber. 2012. Robotic adrenalectomy. Journal of Surgical Oncology 106:5, 622-625. [CrossRef] 5. L. Brunaud, N. Reibel, A. Ayav. 2011. Chirurgie pancréatique, endocrinienne et de l’obésité : place de la chirurgie robotique. Journal de Chirurgie Viscérale . [CrossRef] 6. L. Brunaud, N. Reibel, A. Ayav. 2011. Pancreatic, endocrine and bariatric surgery: The role of robot-assisted approaches. Journal of Visceral Surgery . [CrossRef] 7. Laurent Brunaud, Adeline Germain, Rasa Zarnegar, Thomas Cuny, Ahmet Ayav, Laurent Bresler. 2011. Robot-assisted Adrenalectomy. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 21:4, 248-254. [CrossRef] 8. Volkan Genc, Orhan Agcaoglu, Eren Berber. 2011. Robotic endocrine surgery: technical details and review of the literature. Journal of Robotic Surgery . [CrossRef] 9. P. C. Giulianotti, N. C. Buchs, P. Addeo, F. M. Bianco, S. M. Ayloo, G. Caravaglios, A. Coratti. 2011. Robot-assisted adrenalectomy: a technical option for the surgeon?. The International Journal of Medical Robotics and Computer Assisted Surgery 7:1, 27-32. [CrossRef] 10. Sang-Wook Kang, Woong Youn Chung. 2011. Robotic techniques for adrenal surgery. Journal of Robotic Surgery 5:1, 73-77. [CrossRef] 11. Jennifer Yates, Jayant Uberoi, Ravi Munver. 2010. Robot-assisted laparoscopic partial adrenalectomy: a case report and review of the literature. Journal of Robotic Surgery 4:3, 149-154. [CrossRef] 12. James S. Rosoff, Brandon J. Otto, Joseph J. Pizzo. 2010. The Emerging Role of Robotics in Adrenal Surgery. Current Urology Reports 11:1, 38-43. [CrossRef] 13. Angelish Kumar, Elias S. Hyams, Michael D. Stifelman. 2009. Robot-Assisted Partial Adrenalectomy for Isolated Adrenal Metastasis. Journal of Endourology 23:4, 651-654. [Abstract] [Full Text PDF] [Full Text PDF with Links] 14. M.K. Walz. 2009. Nebennierenresektion zum Erhalt der adrenokortikalen Funktion. Der Chirurg 80:2, 99-104. [CrossRef] 15. Craig G. Rogers, Adam M. Blatt, George E. Miles, W. Marston Linehan, Peter A. Pinto. 2008. Concurrent Robotic Partial Adrenalectomy and Extra-Adrenal Pheochromocytoma Resection in a Pediatric Patient with Von Hippel-Lindau Disease. Journal of Endourology 22:7, 1501-1504. [Abstract] [Full Text PDF] [Full Text PDF with Links] 16. Grant I. S. Disick, Ravi Munver. 2008. Adrenal-preserving minimally invasive surgery: Update on the current status of laparoscopic partial adrenalectomy. Current Urology Reports 9:1, 67-72. [CrossRef]