Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
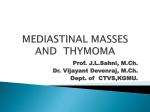
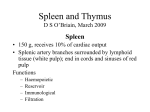
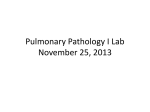
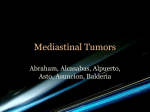
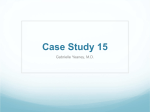
Anatomic Pathology / WHO Histologic Subtyping of Thymomas Thymomas I A Clinicopathologic Correlation of 250 Cases With Emphasis on the World Health Organization Schema Cesar A. Moran, MD,1 Annikka Weissferdt, MD,1 Neda Kalhor, MD,1 Luisa M. Solis, MD,1 Carmen Behrens, MD,1 Ivan I. Wistuba, MD,1 and Saul Suster, MD2 Key Words: Classification; Thymoma; Mediastinum; Tumor; Thymus DOI: 10.1309/AJCP76KEGWQKWOKA Abstract We describe 250 cases of thymoma with emphasis on World Health Organization (WHO) histologic subtyping. The patients were 120 males and 130 females between the ages of 13 and 92 years. Surgical resection was performed, and histologic material was evaluated in every case. Macroscopically, the tumors varied in size from 3 to 20 cm in greatest diameter; about 12% were encapsulated, and about 88% were invasive tumors. A minimum of 5 sections of tumor was evaluated. Histologically, following the schema proposed by the WHO, 21.6% of thymomas were type A, 1.23% type B1, 3.2% type B2, and 9.2% type B3. More than 50% of tumors after subtyping fell into the mixed categories, which, in essence, diminishes the clinical impact of histologic subtyping over staging. The study herein described highlights that all thymomas had the potential to become invasive tumors. During the last 2 decades, the issue of the classification of thymomas and the importance of their histologic subtype has been discussed, and different viewpoints have emerged. Some proponents consider that histologic subtyping has an important role in their clinical behavior,1,2 while others consider that staging at the time of diagnosis is more important.3-5 In the 1990s, as a consequence of the different classification systems, the World Health Organization (WHO) convened a panel of pathologists with the idea of shedding some light on this rather complicated subject. In 1999,6 a schema was produced with the main idea being to use it as a sort of translator/facilitator for 2 of the existing classifications.7,8 That system, as it still is today, was basically composed of letters and numbers with the corresponding meaning of 2 classification systems, the Bernatz classification7 and the so-called histogenetic classification of Marino and Müller-Hermelink.8 In the 2004 publication by the WHO,2 this schema of letters and numbers remained, and at this time, the authors added clinical behavior to the different types of thymoma. However, this particular issue of assigning specific clinical behavior to particular histologic types has generated controversy, which has been highlighted in different publications.9-11 Materials and Methods We identified 250 thymomas from the files of the Department of Pathology, M.D. Anderson Cancer Center, Houston, TX, during a period from 1980 to 2009. The material was carefully selected among more than 400 cases of thymic epithelial neoplasms. Specific requirements were established for inclusion. 444 444 Am J Clin Pathol 2012;137:444-450 DOI: 10.1309/AJCP76KEGWQKWOKA © American Society for Clinical Pathology Anatomic Pathology / Original Article Results Materials Minimum requirements were established for inclusion in the study: (1) histologic evaluation in every case; (2) at least 5 histologic sections of tumor for proper subtyping, as has been previously analyzed12; (3) surgical resection in every case (biopsy material not included in the study). The number of histologic sections in the evaluation of these cases varied from 5 to 30 per case. The clinical records of each case were reviewed and entered in a database for further analysis. Clinical Features Methods The tumors were divided into different subtypes following the WHO schema (type A, AB, B1, B2, and B3). A minimum of 5% of a particular subtype was required to further classify the tumor as having a mixed histologic type. This procedure was performed by light microscopy during the evaluation of all histologic sections available for review. A case was deemed to have mixed histologic type if the minimum of 5% would fulfill the requirement that by itself would be coded under that particular subtype. Once the subclassification was performed, further subtyping of the different combinations of histologic types was also documented. A subset of 41 cases of pure (single histologic type) invasive spindle cell thymomas from this series of cases has been reported.13 ❚Table 1❚ depicts some of the most relevant features of the 250 cases evaluated. The patients were 120 males and 130 females between the ages of 13 and 92 years, with the majority of tumors occurring in the fifth, sixth, and seventh decades of life (median age, 57 years). The most common symptoms were chest pain, cough, and dyspnea. Of the patients, 6 had a history of another malignancy: breast carcinoma, 2; prostatic carcinoma, 2; colonic adenocarcinoma, 2; and papillary carcinoma of the thyroid, 1. None of the patients in our study had associated myasthenia gravis. All patients had surgical resection of the tumor. Statistical analysis of age and sex compared with the histologic types of thymoma demonstrated that types A and A + B1 tumors seemed to be more common in older patients (older than the median of 57 years) compared with the same tumor types in younger patients (younger than the median age, 58/78 [74%] vs 20/78 [26%]). On the other hand, B1 and any B2/B3 thymomas seemed to be more common in younger people (younger than the median age) than in older patients (105/172 [61.0%] vs 67/172 [39.0%]; P < .0001; Fisher exact test). In addition, thymoma type B1 seemed to be more common in females than in males (24/33 [73%] vs 9/33 [27%]; P = .0144; Fisher exact, 2-tailed). We did not observe any differences among types A, A + B1, or any of the other type B thymomas. Statistical Analysis Analysis was performed by using Statistica software, version 6 (StatSoft, Tulsa, OK). Survival analysis was performed using the Kaplan-Meier method. Statistical significance was defined as a P value of less than .05. Macroscopic Features Grossly, the size of the tumors varied from 3 to 20 cm in greatest diameter (median, 7 cm). The tumors were described as round to ovoid tumor masses, which at the cut surface were white to light brown, had a solid consistency, and had a ❚Table 1❚ Correlation Between Clinicopathologic Features and Thymoma Type* Characteristic Age (median, 57 y) <Median ≥Median Sex Female Male Size (median, 7 cm)‡ <7 ≥7 Invasive No Yes Mean follow-up (y) * † ‡ Type A and A + B1 (n = 78) Type B1 and any B2/B3 (n = 172) Total (n = 250) 20 (26) 58 (74) 105 (61.0) 67 (39.0) 125 (50.0) 125 (50.0) 38 (49) 40 (51) 92 (53.5) 80 (46.5) 130 (52.0) 120 (48.0) 33/57 (58) 24/57 (42) 44/104 (42.3) 60/104 (57.7) 77/161 (47.8) 84/161 (52.2) 12 (15) 66 (85) 3.19 19 (11.0) 153 (89.0) 3.63 31 (12.4) 219 (87.6) 3.49 P† <.0001 .4954 .0702 .4074 — Data are given as number (percentage) or, when different from the number in the column heading, as number/total (percentage). Fisher exact test, 2-tailed. Information not available for 89 patients. © American Society for Clinical Pathology Am J Clin Pathol 2012;137:444-450 445 DOI: 10.1309/AJCP76KEGWQKWOKA 445 445 Moran et al / WHO Histologic Subtyping of Thymomas ❚Table 2❚ Thymomas by Histologic Type (n = 250) Histologic Type No. of Cases Percentage of Total A A+B A + B1 A + B1 + B2 A + B1 + B2 + B3 A + B2 A + B3 B B1 B2 B3 B1 + B2 B1 + B2 + B3 B2 + B3 B1 + B3 54 38 24 6 6 1 1 158 33 8 23 47 29 15 3 21.6 15.2 9.6 2.4 2.4 0.4 0.4 63.2 13.2 3.2 9.2 18.8 11.6 6.0 1.2 ❚Image 1❚ Thymoma showing dual histologic features of types A and B1 (H&E, ×10). homogeneous surface. In 7 cases, focal areas of necrosis and cystic changes were recorded. The size of the tumor did not correlate with any particular histologic growth pattern. Histologic Features ❚Table 2❚ and ❚Table 3❚ depict some of the most salient histologic features of the 250 thymomas. The tumors were divided following the schema of the WHO. A minimum of 5 histologic sections per tumor was evaluated, and a minimum of 5% histologic subtype was used to classify the tumor as of mixed histologic type. The highest concordance of thymomas with a single histologic subtype was observed in type A (spindle cell–medullary thymoma) in 54 cases, equivalent to 21.6%. Types B1, B2, and B3 represented 13.2%, 3.2%, and 9.2%, respectively, of the total number of cases with a single histologic type. Based on these results, the percentage of cases using strict criteria of 5 histologic sections and at least 5% of a different histologic subtype accounted for approximately 47.2% of the cases. Approximately 52.8% of the tumors showed mixed histologic types ❚Image 1❚, ❚Image 2❚, and ❚Image 3❚. However, it is important to highlight that the majority of cases (158 cases) were of the B-type thymoma, 54 cases showed single histologic type A thymoma, and 38 cases showed a combination of type A and any type B thymoma. Therefore, based on these results, the possibilities of placing a particular tumor with a single subtype into any of the categories established by WHO is not higher than 21% for type A thymomas, while those of placing a tumor with a single histologic type into the B subtypes is not higher than 25%. In addition, the minimum requirement of 5 sections of tumors seems to hold true because the more sections available for evaluation, the more likely the tumor will show mixed histologic types. ❚Figure 1❚ and ❚Table 4❚ show the analysis of ❚Table 3❚ Clinicopathologic Analysis of 250 Thymomas With Histologic Type Detail Characteristic A Sex Female Male Total Age <Median ≥Median Total Invasive No Yes Total Size (cm) <7 ≥7 Total Not available 446 446 B1 and B2 B1 B1, B2, and B3 AB1 B3 B2 and B3 B2 A, B1, B2, B1 and A, B1 A and and B3 B3 and B2 B2 A and B3 Total 26 (48) 24 (51) 24 (73) 12 (41) 12 (50) 11 (48) 8 (53) 3 (37) 4 (67) 28 (52) 23 (49) 9 (27) 17 (59) 12 (50) 12 (52) 7 (47) 5 (63) 2 (33) 54 (100) 47 (100) 33 (100) 29 (100) 24 (100) 23 (100) 15 (100) 8 (100) 6 (100) 1 (33) 4 (67) 0 (0) 1 (100) 130 (52.0) 2 (67) 2 (33) 1 (100) 0 (0) 120 (48.0) 3 (100) 6 (100) 1 (100) 1 (100) 250 (100.0) 15 (28) 33 (70) 20 (61) 18 (62) 5 (21) 13 (57) 8 (53) 5 (63) 2 (33) 39 (72) 14 (30) 13 (39) 11 (38) 19 (79) 10 (43) 7 (47) 3 (37) 4 (67) 54 (100) 47 (100) 33 (100) 29 (100) 24 (100) 23 (100) 15 (100) 8 (100) 6 (100) 2 (67) 3 (50) 0 (0) 1 (100) 125 (50.0) 1 (33) 3 (50) 1 (100) 0 (0) 125 (50.0) 3 (100) 6 (100) 1 (100) 1 (100) 250 (100.0) 9 (17) 11 (23) 3 (9) 2 (7) 3 (13) 0 (0) 1 (7) 0 (0) 0 (0) 45 (83) 36 (77) 30 (91) 27 (93) 21 (88) 23 (100) 14 (93) 8 (100) 6 (100) 54 (100) 47 (100) 33 (100) 29 (100) 24 (100) 23 (100) 15 (100) 8 (100) 6 (100) 1 (33) 1 (17) 0 (0) 0 (0) 31 (12.4) 2 (67) 5 (83) 1 (100) 1 (100) 219 (87.6) 3 (100) 6 (100) 1 (100) 1 (100) 250 (100.0) 23 (61) 15 (39) 38 (100) 16 1 (100) 0 (0) 1 (100) 2 12 (44) 15 (56) 27 (100) 20 10 (45) 12 (55) 22 (100) 11 Am J Clin Pathol 2012;137:444-450 DOI: 10.1309/AJCP76KEGWQKWOKA 13 (62) 8 (38) 21 (100) 8 10 (53) 9 (47) 19 (100) 5 1 (9) 10 (91) 11 (100) 12 2 (25) 6 (75) 8 (100) 7 3 (60) 2 (40) 5 (100) 3 0 (0) 4 (100) 4 (100) 2 1 (33) 2 (67) 3 (100) 3 1 (100) 0 (0) 1 (100) 0 0 (0) 1 (100) 1 (100) 0 77 (47.8) 84 (52.2) 161 (100.0) 89 © American Society for Clinical Pathology Anatomic Pathology / Original Article ❚Image 2❚ Thymoma showing dual histologic features of types B1 and B3 (H&E, ×10). ❚Image 3❚ Thymoma showing dual histologic features of types B2 and B3 (H&E, ×10). histologic sections compared with the histologic subtyping of thymoma and the mean number of sections examined. recurrent or metastatic disease. Of the remaining patients, 46 died in the same period, 4 of them with documented recurrent or metastatic disease. Clinical follow-up was not obtained for 19 patients. Kaplan-Meier curves were developed to correlate the histologic type of the thymoma with the survival rate in 231 cases, with follow-up information giving a P value of .452, which is not statistically significant. Also not statistically significant was the P value of .226 obtained when comparing types A and A + B1 with any B type ❚Figure 2❚ and ❚Figure 3❚. A possible significant trend with a P value of .056 was obtained when comparing types A and A + B1 with B1 and any B2-B3 thymomas for recurrence-free survival ❚Figure 4❚. Staging Of the 250 cases evaluated, 31 were encapsulated tumors (Masaoka stage I), and 219 cases corresponded to invasive thymomas, most of them in Masaoka stages II and III and only a few cases in stage IV. Follow-up Clinical follow-up information was obtained for 231 patients, ranging from 1 to 16 years (mean follow-up, 3.49 years). Of the patients, 185 were alive, of whom 22 had ❚Table 4❚ Histologic Subtyping in 250 Thymomas Compared With the Mean Number of Sections Examined* 140 120 No. of Slides 100 80 Slides per tumor analyzed >20 16-20 11-15 6-10 5 60 40 20 0 A B1 B2 B3 Mixed Histologic Subtype ❚Figure 1❚ The number of sections analyzed and the likely outcome of thymoma subtyping. Histologic Type No. of Cases Percentage of Total Mean No. of Slides per Tumor A A+B A + B1 A + B1 + B2 A + B1 + B2 + B3 A + B2 A + B3 B B1 B2 B3 B1 + B2 B1 + B2 + B3 B2 + B3 B1 + B3 54 38 24 6 6 1 1 158 33 8 23 47 29 15 3 21.6 15.2 9.6 2.4 2.4 0.4 0.4 63.2 13.2 3.2 9.2 18.8 11.6 6.0 1.2 10 11 9 14 14 14 14 12 12 16 12 13 13 13 10 * We examined at least 5 H&E-stained slides per tumor (range, 5-30; mean, 12). © American Society for Clinical Pathology Am J Clin Pathol 2012;137:444-450 447 DOI: 10.1309/AJCP76KEGWQKWOKA 447 447 Moran et al / WHO Histologic Subtyping of Thymomas 1.0 0.9 Complete Censored A, AB1 0.8 Overall Survival 0.7 0.6 B1, any B2-B3 0.5 0.4 0.3 0.2 0.1 0.0 –0.1 0 2 4 6 8 10 12 14 16 18 20 Time (y) ❚Figure 2❚ Comparison of histologic subtyping for types A and AB1 vs B1, B2, and B3 and overall survival (Kaplan-Meier analysis; cumulative proportion surviving, n = 231). P = .226 (statistically not significant). Discussion The knowledge that thymomas represent a heterogeneous group of tumors and that their histologic classification is difficult has been previously emphasized in the literature.14,15 As a matter of fact, Rosai and Levine15 stated: “…once the term thymoma is restricted to the tumor of epithelial thymic cells, with or without a lymphocytic component, all further subdivisions are artificial.” Also of common knowledge are the different features that have been evaluated in thymomas to predict clinical outcome. In that regard, parameters such as histologic type, grading, and 1.0 Overall Survival 0.7 0.6 0.5 Any B2-B3 B1 0.3 0.2 0.1 0 2 4 6 8 10 12 14 16 18 20 Time (y) ❚Figure 3❚ Different overall survival curve separating types A and AB1 from B1 and other B2-B3 thymomas (Kaplan-Meier analysis; cumulative proportion surviving, n = 231). P = .452 (statistically not significant). 448 448 0.8 B1 0.7 Any B2-B3 0.6 0.5 0.4 0.3 0.2 0.0 –0.1 Complete Censored 0.9 0.8 0.4 A, AB1 1.0 Complete Censored A, AB1 Recurrence-Free Survival 0.9 staging have been previously analyzed. More recently, the issue of histologic subtyping has gained popularity in the evaluation of thymomas with certain histologic types being associated with more or less aggressive clinical behavior.2 Needless to say, owing to the rarity of these tumors, it is difficult to obtain a sizable number of cases to be able to produce important and meaningful conclusions. Thus, one is left to attempt to obtain information from various studies, which might not have addressed the same issues, and then to draw conclusions from those studies. Based on some of those studies, one can determine that, for the most part, sex, age, clinical manifestations, size of the tumor, and even the association of myasthenia gravis have not produced enough statistically significant information to properly correlate any of those features with tumor behavior.16-26 Nevertheless, the 2 most important parameters that have been mentioned in the literature for clinical outcome of thymomas are staging and histologic type. Of those two, let us concentrate on the histologic features and subtyping of thymomas. Type A thymoma (spindle cell–medullary thymoma) is considered by the WHO to be a benign tumor. However, 21% of the cases herein presented belong to that histologic type (invasive tumors previously reported), and the tumors were observed to be in different stages of invasion,13 thereby casting serious doubt as to the validity of such a clinical designation. Important to note is the fact that the definition of thymoma AB by the WHO is that of a spindle cell thymoma (type A) with lymphocytes. In practice, those tumors most likely are grouped under type A as the association of type A and B1 thymoma can occur, as documented in the cases herein presented. Am J Clin Pathol 2012;137:444-450 DOI: 10.1309/AJCP76KEGWQKWOKA 0.1 0 2 4 6 8 10 12 14 16 18 20 Time (y) ❚Figure 4❚ There is a possible trend in the recurrence-free survival for types A, AB1 vs the other types of thymoma. However, the value is not statistically significant (P = .056). Kaplan-Meier analysis; cumulative proportion surviving, n = 231. © American Society for Clinical Pathology Anatomic Pathology / Original Article On the other hand, when proper sampling is done, the type B1 and B2 thymomas in the WHO classification, in their pure form, become uncommon tumors, as one is most likely to find a mixture of histologic types in these particular tumors. In our experience, such histologic categorization can be accomplished in no more than 14% of these tumors. Furthermore, one of the most important parameters that has not been taken into account when dealing with the WHO schema or any other classification system is the issue of sampling. Based on our experience, when these tumors are amply sampled, the most likely outcome is that the majority will show mixed histologic types, which in turn raises the question of the validity of any subtyping. However, that is not surprising, as previous studies have analyzed such features. The sampling issue can actually be viewed in 2 ways: 1, for proper histologic subtyping, and 2, probably even more important, to rule out the possibility of tumors showing thymoma and thymic carcinoma.27 The fact that fewer than 50% of thymomas will show a single histologic type speaks in favor of the artificial and arbitrary nature of any schema or classification system. On the other hand, the WHO schema was not intended as an official classification system but rather as a “translator” of 2 already existing classification systems. The designation of letters and numbers themselves has no meaning other than the specific designation of a particular tumor for a particular classification. Therefore, the use of this schema, without proper designations as to what it means, is meaningless. One additional feature that we have been able to introduce in this study is the amount of tumor that one needs to have present to be able to diagnose a thymoma as of mixed histologic type. In our experience, there has to be at least 5% of a tumor that unequivocally will, by itself, be diagnosed using any other classification system. However, more important is the fact that regardless of the histologic subtype of thymoma, histologic type alone cannot be correlated with clinical outcome, as statistically demonstrated in this study. We have presented a study of 250 thymomas in which we have documented, regardless of the histologic subtype, that all are capable of invasion and aggressive behavior. We consider that sampling is an important issue in the subtyping of these tumors and recommend that a minimum of 5 sections of tumor (when feasible) is needed to assign a specific subtype. Also important is to properly assess at least 5% of a different histologic growth pattern to determine that a tumor is of mixed histologic type. We believe that the subclassification of thymomas should not be done on biopsy material. Furthermore, we judge that a decision on treatment should not be based on the histologic subtype of these tumors, as we have clearly demonstrated that not only are all histologic types capable of invasion, but also that the majority of these tumors show mixed histologic types. From the Departments of Pathology, 1M.D. Anderson Cancer Center, Houston, TX, and 2Medical College of Wisconsin, Milwaukee. Address reprint requests to Dr Moran: Dept of Pathology, M.D. Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030. References 1. Quintanilla-Martinez L, Wilkins EW Jr, Choi N, et al. Thymoma: histologic subclassification is an independent prognostic factor. Cancer. 1994;74:606-617. 2. Travis WD, Brambilla E, Müller-Hermelink HK, et al, eds. WHO Classification of Tumours: Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. Lyon, France: IARC Press; 2004. 3. Bernatz PE, Khonsari S, Harrison EG, et al. Thymoma: factors influencing prognosis. Surg Clin North Am. 1973;53:885-892. 4. Verley JM, Hollman KK. Thymoma: a comparative clinical study of clinical stages, histologic features, and survival in 200 cases. Cancer. 1985;55:1074-1086. 5. Wick MR. Prognostic factors for thymic epithelial neoplasms, with emphasis on tumor staging. Hematol Oncol Clin North Am. 2008;22:527-542. 6. Rosai J. Histological Typing of Tumours of the Thymus. 2nd ed. Berlin, Germany: Springer; 1999. 7. Bernatz PE, Harrison EG, Clagett OT. Thymoma: a clinicopathologic study. J Thorac Cardiovasc Surg. 1961;42:424-444. 8. Marino M, Müller-Hermelink HK. Thymoma and thymic carcinoma: relation of thymoma epithelial cells to the cortical and medullary differentiation of thymus. Virchows Arch A Pathol Anat Histopathol. 1985;407:119-149. 9. Moran CA, Suster S. The World Health Organization (WHO) histologic classification of thymomas: a reanalysis. Curr Treat Options Oncol. 2008;9:288-299. 10. Suster S, Moran CA. Problem areas and inconsistencies in the WHO classification of thymoma. Semin Diagn Pathol. 2005;22:189-197. 11. Suster S, Moran CA. Thymoma classification: current status and future trends. Am J Clin Pathol. 2006;125:542-554. 12. Moran CA, Suster S. On the histologic heterogeneity of thymic epithelial neoplasms: impact of sampling in subtyping and classification of thymoma. Am J Clin Pathol. 2000;114:760-766. 13. Moran CA, Kalhor N, Suster S. Invasive spindle cell thymoma (WHO type A): a clinicopathologic correlation of 41 cases. Am J Clin Pathol. 2010;134:793-798. 14. Castleman B. Tumors of the Thymus Gland. Washington, DC: Armed Forces Institute of Pathology; 1955. Atlas of Tumor Pathology; First Series, Fascicle 19. 15. Rosai J, Levine GD. Tumors of the Thymus. Washington, DC: Armed Forces Institute of Pathology; 1976. Atlas of Tumor Pathology; Second Series, Fascicle 13. 16. Salyer WR, Eggleston JC. Thymoma: a clinical and pathological study of 65 cases. Cancer. 1976;37:229-249. 17. Lewis JE, Wick MR, Bernatz PE, et al. Thymoma: a clinicopathologic review. Cancer. 1987;60:2727-2743. © American Society for Clinical Pathology Am J Clin Pathol 2012;137:444-450 449 DOI: 10.1309/AJCP76KEGWQKWOKA 449 449 Moran et al / WHO Histologic Subtyping of Thymomas 18. Nahahara A, Ohno K, Hashimoto J, et al. Thymoma: results with complete resection and adjuvant postoperative irradiation in 141 consecutive patients. J Thorac Cardiovasc Surg. 1988;95:1041-1047. 19. Pescarmona E, Rendina EA, Venuta F, et al. Analysis of prognostic factors and clinicopathologic staging of thymoma. Ann Thorac Surg. 1990;50:534-538. 20. Maggi G, Casadio C, Cavallo A, et al. Thymoma: results of 241 operative cases. Ann Thorac Surg. 1991;51:152-156. 21. Wilkins EW, Grillo HC, Scannell JG, et al. Role of staging in prognosis and management of thymoma. Ann Thorac Surg. 1991;51:888-892. 22. Park HS, Shin DM, Lee JS, et al. Thymoma: a retrospective study of 87 cases. Cancer. 1994;73:2491-2494. 23. Pan CC, Wu HP, Yang CF, et al. The clinicopathologic correlation of epithelial subtyping in thymoma: a study of 112 consecutive cases. Hum Pathol. 1994;25:893-899. 450 450 Am J Clin Pathol 2012;137:444-450 DOI: 10.1309/AJCP76KEGWQKWOKA 24. Blumberg D, Port JL, Weksler B, et al. Thymoma: a multivariate analysis of factors predicting survival. Ann Thorac Surg. 1995;60:908-914. 25. Regnard JF, Magdeleinat P, Drower C, et al. Prognostic factors and long-term results after thymoma resection: a series of 307 patients. J Thorac Cardiovasc Surg. 1996;112:376-384. 26. Lattes R. Thymoma and other tumors of the thymus: an analysis of 107 cases. Cancer. 1962;15:1224-1260. 27. Suster S, Moran CA. Primary thymic epithelial neoplasms with combined features of thymoma and thymic carcinoma: a clinicopathologic study of 22 cases. Am J Surg Pathol. 1996;20:1469-1480. © American Society for Clinical Pathology