Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
American Journal of Epidemiology
Copyright © 1998 by The Johns Hopkins University School of Hygiene and Public Health
All rights reserved
Vol. 148, No. 5
Printed in U.S.A.
ORIGINAL CONTRIBUTIONS
Attributable Fraction for Cardiac Malformations
P. David Wilson,1 Christopher A. Loffredo,1 Adolfo Correa-Villasefior,2 and Charlotte Ferencz1
To the authors' knowledge, attributable fractions for cardiac malformations have not been reported before.
The Baltimore-Washington Infant Study published factors associated with several major cardiac malformations in Maryland, the District of Columbia, and adjacent counties of northern Virginia in 1981-1989. For eight
of these malformations, the authors provide attributable fractions of those factors that are potentially causal.
Summary attributable fractions range from 13.6% (four factors) for hypoplastic left heart to 30.2% (seven
factors) for transposition of great arteries with intact ventricular septum. Extra attributable fraction for factor x,
defined as summary attributable fraction for all factors minus that for all but x, is largest for: 1) paternal
marijuana use in transposition of great arteries with intact ventricular septum, 7.8%; 2) paternal anesthesia in
tetralogy of Fallot, 3.6%; 3) painting in atrioventricular septal defect with Down syndrome, 5.1%; 4) solvent/
degreasing agent exposure in hypoplastic left heart, 4.6%; 5) sympathomimetics in coarctation of aorta, 5.8%;
6) pesticide exposure in isolated membranous ventricular septal defect, 5.5%; 7) hair dye in multiple/multiplex
membranous ventricular septal defect, 3.3%; and 8) urinary tract infection in atrial septal defect, 6.4%.
Percent-of-cases-exposed dominates relative risk in attributable fraction. If these factors are causal, the larger
extra attributable fractions suggest the potential for prevention by specific interventions before/during pregnancy. Am J Epidemiol 1998; 148:414-23.
congenital heart defects; epidemiologic methods; logistic regression; preventive health services; risk
factors
Congenital abnormalities of the heart and great vessels constitute a major cause of infant mortality and of
morbidity in childhood and adult life. The BaltimoreWashington Infant Study, a large population-based
case-control study of congenital heart disease, provided a comprehensive epidemiologic assessment of
familial and environmental factors which might contribute to the occurrence of developmental abnormalities of the heart (1,2). The design and analysis plan of
that study was built on evidence derived from human
and animal studies which indicated that a multiplicity
of intrinsic and extrinsic factors are responsible for
developmental disturbances (3, 4).
Epidemiologic studies, especially case-control studies, are appropriate for the identification of constellations of factors that might be associated with cardio-
vascular anomalies (5, 6). We use the terms "direct
association," "causal association," and "risk factor"
synonymously. Although some associations may be
causal, causal inferences and preventive recommendations from case-control studies must be formulated
with caution. Some associations will be indirect (noncausal) and interventions on such associated factors
are likely to be nonproductive. There may be other
associations that seem to be directly related, but for
which no adequate biologic explanation has yet been
found; that is, they are potential risk factors or potentially causal factors. However, there are many examples where epidemiologic findings have preceded
understanding of biologic causality. Preventive interventions for potentially causal factors may be implemented even when understanding of biologic causality
is limited, provided that the expected benefits outweigh the risks and costs of the interventions.
One measure of the potential benefit of an intervention is an estimate of the fraction of the cases of the
disease that might be prevented by eliminating a risk
factor or exposure. The "population attributable fraction" (sometimes called population attributable risk) is
used for this purpose. It is defined as the fraction of the
Received for publication April 29, 1997, and accepted for publication December 4, 1997.
1
Department of Epidemiology and Preventive Medicine, University of Maryland School of Medicine, Baltimore, MD.
2
Department of Epidemiology, Johns Hopkins University School
of Hygiene and Public Health, Baltimore, MD.
Reprint requests to P. David Wilson, Department of Epidemiology
and Preventive Medicine, University of Maryland School of Medicine, 660 W. Redwood Street - H #111, Baltimore, MD 21201.
414
Heart Defect Attributable Risk
total number of cases of the disease that would not
have occurred in the population if the causally related
factor had been absent.
To our knowledge, attributable fractions for cardiac
anomalies have not been reported before. In this paper,
we evaluate the attributable fraction of the potentially
causal factors among the malformation-associations
published by the Baltimore-Washington Infant Study
for eight major types of cardiac anomalies (1). The
population to which we refer is that of infants born
between April 1981 and December 1989 in Maryland,
the District of Columbia, and the adjacent counties of
northern Virginia.
MATERIALS AND METHODS
Except for the attributable fraction methods given
below, the Baltimore-Washington Infant Study methods have been previously reported in detail (1,2). The
relevant features of the study may be summarized as
follows.
Cases
The cases were 4,296 liveborn infants with structural congenital heart defects, born in the above time
and region. Premature infants with patent arterial duct
as an isolated defect and infants with arrhythmias in
the absence of cardiac malformations were not included. The primary source of cases was the network
of six pediatric cardiology centers serving the region.
We also conducted community searches, including
annual reviews of pathology logbooks in each participating hospital, state medical examiners' logbooks,
and death certificates, where available.
Malformations were confirmed during the first year
of life by echocardiography, cardiac catheterization,
surgery, or autopsy. A hierarchical classification system was used to assign infants with multiple cardiac
anomalies to a single diagnostic group, giving the
highest priority to structural malformations of the earliest embryonic origin. A follow-up confirmation of
the diagnosis was obtained in 92.6 percent of cases by
a cardiologist's examination near the infant's first
birthday or by autopsy findings. Detailed definitions
of the cardiac malformations studied in this report
have been published (1). Brief definitions are given
below.
Transposition of the great arteries with intact ventricular septum. The great arteries arise abnormally
so that the aorta receives venous blood from the right
ventricle, and the pulmonary artery receives arterialized blood from the left ventricle. Of 115 enrolled case
families, 106 (92.2 percent) were interviewed.
Tetralogy of Fallot. Partial obstruction at and/or
Am J Epidemiol
Vol. .148, No. 5, 1998
415
below the pulmonary valve. The defect is associated
with a ventricular septal defect. Anatomic variations,
in the site and nature of the pulmonic stenosis and the
size of the ventricular septal defect, were not considered. Of the 236 enrolled case families, 204 (86.4
percent) were interviewed.
Atrioventricular septal defects with Down syndrome.
Defective formation of the atrioventricular valves and
adjacent septa; characteristic of abnormal hearts in
Down syndrome. Of the 210 enrolled case families,
190 (90.5 percent) were interviewed.
Hypoplastic left heart syndrome. Multiple leftsided obstructions involving the mitral and aortic
valves, leading to underdevelopment of the left ventricle and compromised aortic flow. Of the 162 enrolled case families, 138 (85.2 percent) were interviewed.
Coarctation of the aorta. An isolated defect defined as a narrowing of the thoracic aorta in the vicinity of the arterial duct. Of 126 enrolled case families,
120 (95.2 percent) were interviewed.
Ventricular septal defect, membranous type. A defect in the membranous area of the ventricular septum
at the base of the aorta. A total of 895 cases were
ascertained, but a random sample of mild cases was
excluded from interview. Of the remaining 748 case
families, 640 (85.6 percent) were interviewed. The
analysis was stratified by the following two subsets
because they show different potential risk factors.
Isolated/simplex (459 cases): the defect is the only
congenital abnormality; first-degree relatives of the
proband are free of congenital abnormalities. Multiple/
multiplex (181 cases): the cardiac defect occurs in
association with non-cardiac anomalies and/or in the
presence of cardiac or non-cardiac anomalies in the
family.
Atrial septal defect. A defect between the right and
left atria is located in the position of the embryonic
foramen ovale (ostium secundum defect). No other
cardiac abnormalities are present. Of 213 enrolled
cases with isolated atrial septal defect, free of noncardiac malformations, 187 case families (87.8 percent) were interviewed.
Overall in these malformations, 1,810 families were
eligible for interview, and we were successful in interviewing 1,585 or 87.6 percent of these families.
Controls
The controls were 3,572 liveborn infants free of
congenital heart defects and born to residents of the
region during the study period 1981-1989. Controls
were selected each year as a random sample of the area
births, stratified by hospital of birth. Selection was
independent of case enrollment. The proportion se-
416
Wilson et al.
lected from each hospital was the expected proportion
of the regional live births attributable to that hospital.
The targeted number of controls was achieved by
replacing nonrespondents with the births nearest in
time from the same hospital. Ninety-five percent of the
controls were the original selection or first alternate.
Because there were very few controls with a family
history of congenital abnormalities, and because family history of congenital abnormalities was used to
define the two membranous ventricular septal defect
subgroups (isolated/simplex and multiple/multiplex),
the controls included in analysis of these subgroups
were those that had no abnormalities in the proband or
family.
Data collection
After written consent, a questionnaire was administered to the parents of the cases and controls by trained
interviewers. The primary respondent was almost always the mother (98 percent in cases, 99 percent in
controls). The father participated with the mother in
about 20 percent of case interviews and 15 percent of
control interviews. The interview was completed
within one year of birth for over 90 percent of the
cases and of the controls. The questionnaire covered:
family history of cardiac and non-cardiac malformations; the mother's reproductive and medical history
and use of medications; family sociodemographic factors; occupational history of both parents; periconceptional exposure of both parents to: ionizing radiation,
smoking, alcohol, caffeine, recreational drugs, and
household and occupational chemicals, including pesticides, dyes, metals, and solvents. For each exposure,
the questionnaire obtained details on the place, frequency, and nature of the exposure. Exposure information was recorded for the period 3 months before
and after the last normal menstrual period. This
6-month period covers the critical period of cardiogenesis and allows for uncertainty in dating the time of
conception.
Identification of factors associated with
malformations
Analysis was based on the data from all interviewed
families. Our data set consisted of nearly 200 variables, a detailed description of which has been previously published (1, 2). Of these, a binary miscellaneous solvents variable indicated exposure to solvents
other than those used for dry cleaning, degreasing
motors, or cleaning guns. In addition, we defined a
binary "solvent/degreasing agent" variable which includes exposure to the above miscellaneous solvents
as well as exposure to degreasing solvents. From these
variables, for each given malformation, we used unadjusted case-control analysis to select the candidate
malformation-association factors for analysis. We
considered only variables with at least three cases
exposed.
To the candidate factors, we added the following list
of a priori factors unless already present: family history of congenital heart disease, maternal diabetes
mellitus, maternal age, maternal smoking, maternal
alcohol consumption, maternal ionizing radiation exposure, race of infant, and socioeconomic score. The
resulting set of variables was studied by multiple logistic regression methods (7) to select the final set of
malformation-associated factors, to correct for effect
modification and confounding, and to include other
variables for increased precision. Our approach followed that of others (8, 9), and details of the logistic
modeling have been reported (1).
All candidate malformation-associated factors were
in the logistic model initially. For each given candidate in turn, all other candidates were considered as
potential effect modifiers; no effect modification was
found, and the other candidates were then considered
as potential confounders. We retained those candidate
factors that were significant at the 0.05 level after
adjustment for confounding. The criterion for confounding was a change of at least 30 percent in the
odds ratio of the candidate factor. Variables not found
to confound were retained if their presence in the
model increased the precision of the odds ratio estimate of the malformation-associated factor.
Of the final set of factors found to be significantly
associated with a given malformation, attributable
fraction analysis was performed on those considered to
be potentially causal. The others are listed separately
from the main results, with explanation, and the reported relative risks of the potentially causal factors
are adjusted for them.
Because formal multiple inference correction generally results in power loss (10, 11), and because its
use is controversial (12), we did not perform any
formal correction for the multiple inference on the
several variables in the logistic model for a given
malformation. Instead, in addition to presenting results
for potential risk factors that were significantly associated with malformation at the 0.05 level, we also
give results for those that were significant at the 0.01
level in the same model.
Variables used in the models for confounding adjustment or increased precision of the factors significant at the 0.05 level are mentioned in the results as
adjustment variables. Our data show changes in the
prevalence of some malformations over time (13). A
higher level was observed after 1986 compared with
Am J Epidemiol
Vol. 148, No. 5, 1998
Heart Defect Attributable Risk
before 1986, presumably due to increased detection by
echocardiography after that year. Thus, some of our
adjustments are for this "birth-time" factor.
Attributable fraction methods
We report "summary attributable fraction" and "extra attributable fraction." The summary attributable
fraction is the attributable fraction due to a set of risk
factors jointly. It is the fraction of the total number of
cases in the population that would not have occurred if
the causative effects associated with the set of risk
factors had been absent. We define the extra attributable fraction for factor x as the summary attributable
fraction for the entire set of risk factors minus the
summary attributable fraction for all factors in the set
except factor x. Thus, it is the fraction of the cases in
the population that would not have occurred if exposure to x were removed, but the exposures to the other
factors remain unchanged. If exposures to the individual risk factors are disjoint, the extra attributable fractions for the individual risk factors of a set will sum to
the summary attributable fraction. Otherwise the sum
of the individual extra attributable fractions will generally be less than the summary attributable fraction.
We do not report "marginal" attributable fractions,
which are computed ignoring all other risk factors.
The sum of the marginal attributable fractions is often
greater than the summary attributable fraction. Walter
(14, 15) has discussed bias in the use of marginal
attributable fraction.
Because congenital heart malformations are rare, we
used odds ratios from logistic regression to approximate the relative risks, which are required for attributable fraction analysis.
We calculated attributable fractions by the method
of Bruzzi et al. (16). (Also see Benichou (17).) We
developed standard errors of the attributable fractions
by the so-called "delta" method (18). In using this
method, we relied on the results from simulation studies of Greenland and Drescher (19), which showed
that one can ignore the variance of the estimates of the
proportions of the case population that were exposed.
The Appendix contains details and discussion of the
attributable fraction analysis.
RESULTS
For each of the eight malformation types studied,
the attributable fraction results for the potential risk
factors are shown in table 1. Some results for other
factors significantly associated with malformations are
given in table 2. Exposures are maternal unless stated
to be paternal. All of the potential risk factors are
dichotomous or categorical except the solvent expoAm J Epidemiol
Vol. 148, No. 5, 1998
417
sure score; its relative risk is defined in the table legend.
Attributable fractions are expressed as percents.
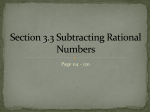
The first column of table 1 gives the malformation
type and potential risk factors. In the line with the
malformation type is the summary attributable fraction
and its 95 percent confidence interval. For each potential risk factor, the extra attributable fraction is
shown, along with the relative risk and the percent of
the cases that were exposed. The relative risks were
reported previously (1). In these malformations, the
number of potential risk factors identified at the 0.05
significance level ranged from three for atrioventricular septal defect with Down syndrome to seven for
transposition of the great arteries with intact ventricular septum, and the summary attributable fraction
based on potential risk factors significant at the 0.05
level ranged from 13.6 percent for hypoplastic left
heart to 30.2 percent for transposition of the great
arteries with intact ventricular septum.
Transposition of the great arteries with intact ventricular septum. The summary attributable fraction
for the seven potential risk factors identified was 30.2
percent. The largest extra attributable fractions were
for paternal use of marijuana (7.8 percent) and maternal influenza (5.2 percent). The relative risk for paternal use of marijuana was only 1.7, but 24.5 percent of
the fathers were exposed. No adjustment of the relative risks was needed. Influenza and miscellaneous
solvent exposures were also significantly associated
with the malformation at the 0.01 level, and their
summary attributable fraction was 12.1 percent.
Tetralogy of Fallot. The summary attributable fraction for the potential risk factors was 17.7 percent. The
relative risks were adjusted for previous miscarriage
(table 2) as well as number of previous pregnancies.
Paternal anesthesia had the largest extra attributable
fraction of the two potential risk factors that were
significant at the 0.01 level.
Atrioventricular septal defect with Down syndrome.
The summary attributable fraction was 14 percent, due
to painting, paternal welding, and ibuprofen. The relative risks were adjusted for maternal age and frequent
use of fireplace (table 2).
Hypoplastic left heart syndrome. The largest extra
attributable fraction (4.6 percent) was due to solvents
(including degreasing agents). While maternal diabetes had a large relative risk (3.9), it had the smallest
extra attributable fraction (1.6 percent), because only
2.2 percent of the case mothers had diabetes mellitus.
No adjustment of the relative risks was needed. All of
the potential risk factors had disjoint exposures in our
data. Thus, the extra attributable fractions were equal
to the marginal attributable fractions and sum exactly
to the summary attributable fractions.
418
Wilson et al.
TABLE 1.
Attributable fraction results: Baltimore-Washington Infant Study, 1981-1989
Summary and extra AF* from
factors significant at
Malformation srwJ
IVICUJUI IlKLllwl 1 Cll IU
0.05 level
potential risk factors
Cases exposed
0.01 level
AF
95% Cl*
AF
Transposition of great arteries with
intact ventricular septum (n* = 106)
Paternal use of marijuana
Influenza
Ibuprofen
Benzodiazepines
Ionizing radiation
Miscellaneous solvents
Progesterone
30.2
7.8
5.2
3.0
2.2
2.2
2.0
1.8
24.2-36.1
2.8-12.7
2.6-7.9
1.4-4.5
1.1-3.3
1.0-3.3
1.0-3.1
0.8-2.9
12.1
8.5-15.8
7.0
3.6-10.3
4.8
3.0-6.6
Tetralogy of Fallot (n = 204)
Paternal anesthesia
Hair dye
Painting (both parents)
Diabetes mellitus
Clomiphene
Benzodiazepines
17.7
3.6
3.5
2.6
2.6
2.0
1.8
13.6-21.8
2.2-5.0
0.8-6.2
0.7-4.4
0.7-4.4
1.2-2.8
1.0-2.7
6.5
3.9
4.8-8.3
2.4-5.5
2.4
1.5-3.4
Atrioventricular septal defect with
Down syndrome (n = 190)
Painting
Paternal welding
Ibuprofen
14.0
5.1
4.1
3.6
9.2-18.7
1.2-8.9
1.4-6.9
2.0-5.2
4.6
4.6
2.7-6.5
Hypoplastic left heart (n = 138)
Sotvent/degreaslng agent
Family history of CHD*
Paternal anesthesia
Diabetes mellitus
13.6
4.6
4.0
3.4
1.6
10.9-16.3
3.2-6.0
3.1-4.9
1.5-5.2
0.9-2.3
8.6
4.6
4.0
6.9-10.3
3.2-6.0
3.1-4.9
Coarctation of the aorta (n = 120)
Sympathomimetics
Family history of CHD
Solvent exposure score
Macrodantln
Clomiphene
Epilepsy
19.5
5.8
3.7
3.0
1.7
1.5
0.9
15.2-23.8
2.0-9.7
2.8-4.7
1.6-4.5
1.2-2.1
1.0-2.1
0.6-1.3
9.4
8.1-10.8
4.6
3.5-5.7
2.3
2.0
1.8-2.8
1.4-2.7
Isolated/simplex membranous
ventricular septal defect {n = 459)
Pesticide exposure
Paternal use of marijuana
Anesthesia
Maternal use of cocaine
Paternal Ionizing radiation
Occupational heat
17.0
5.5
5.3
1.9
1.6
1.1
0.4
11.4-22.7
0.8-10.1
1.9-8.7
0.7-3.1
0.8-2.3
0.5-1.6
0.3-0.6
7.9
4.2-11.6
6.0
2.2-9.7
1.7
0.9-2.5
Multiple/multiplex membranous
ventricular septal defect (n = 181)
Hair dye
Paternal use of cocaine
Ibuprofen
Diabetes mellitus
Metronldazole
Auto body repair
14.9
3.3
2.9
2.2
1.5
1.4
0.6
11.9-17.8
0.9-5.8
1.3-4.4
0.7-3.7
0.9-2.1
1.1-1.7
0.4-0.9
8.3
6.0-10.5
4.8
2.6-6.9
2.1
1.4
1.4-2.8
1.1-1.7
Atrial septal defect (n = 187)
Urinary tract Infection
Gestational diabetes meilltus
Paternal use of cocaine
Family history of CHD
Corticosterolds
Paternal work with virus
21.4
6.4
4.3
3.3
3.1
2.1
0.7
16.5-26.4
2.2-10.7
2.5-6.1
1.7-5.0
2.2-3.9
1.5-2.7
0.4-1.1
14.1
11.3-17.0
4.4
3.7
3.4
2.6
2.5-6.2
1.9-5.4
2.4-4.3
1.9-3.2
95% Cl
No.
o
risk
26
14
10
5
5
8
4
24.5
13.2
9.4
4.7
4.7
7.5
3.8
1.7
2.2
2.5
3.0
2.8
3.2
3.0
14
22
16
14
8
7
6.9
10.8
7.8
6.9
3.9
3.4
2.5
1.6
1.8
1.8
3.0
2.7
32
21
15
16.8
11.1
7.9
1.5
1.7
2.4
9
7
8
3
6.5
5.1
5.8
2.2
3.4
4.8
2.4
3.9
16
7
17
4
4
3
13.3
5.8
14.2
3.3
3.3
2.5
1.8
4.6
6.7
4.5
5.3
141
100
24
15
9
3
30.7
21.8
5.2
3.3
2.0
0.6
1.3
1.4
1.8
2.4
2.4
7.9
21
15
14
5
3
3
11.6
8.3
7.7
2.8
1.7
1.7
1.7
2.3
1.9
3.9
7.6
4.6
38
20.3
7.5
7.0
4.8
3.2
1.6
1.6
2.4
2.3
3.9
4.8
3.9
2.7-6.5
14
13
9
6
3
1.2t
* AF, attributable fraction as percent; Cl, confidence interval; n, number of cases; CHD, congenital heart defect,
t Relative risk for solvent exposure is for mean non-zero score (cases and controls) relative to 0.
Coarctation of the aorta. The summary attributable
fraction of 19.5 percent was due to six potential risk
factors. Sympathomimetics had the largest extra attributable fraction (5.8 percent), because 13.3 percent of
the case mothers used these drugs—usually pseudo-
ephedrine taken for "cold" symptoms. The relative
risks were adjusted for race of infant (table 2).
Isolated/simplex membranous ventricular septal defect. The summary attributable fraction was 17 percent, due to six potential risk factors. Pesticide expoAm J Epidemiol
Vol. 148, No. 5, 1998
Heart Defect Attributable Risk
419
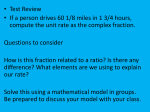
TABLE 2. Significant malformation-associations considered as probable markers:
Baltimore-Washington Infant Study, 1981-1989
Malformation and associated factors
Tetralogy of Fallot (nf= 204)
Previous marriage
Extra
AFt
if jointly
causal
Cases exposed
Relative
risk
No.
7.2
59
28.9
1.5*
30-34
35-39
7.7
28.4
15.8
£40
3.2
4.0
54
30
11
36
5.8
1.5*
2.2**
6.2**
19.0
1.5*
26.3
95
79.2
1.7*
8.2
188
41.0
1.3**
11.9
1.4
9.5
70
38.7
1.7**
4
72
2.2
3.6*
1.4*
10.2
4.2
3.0
0.7
81
39
21
Atrioventricular septal defect with Down
syndrome (n= 190)
Maternal age (years)
Frequent use of fireplace
Coarctation of the aorta (n = 120)
White race of infant
Isolated/simplex membranous
ventricular septal defect (n = 459)
Nonwhite race of infant
6.6
Multiple/multiplex membranous
ventricular septal defect (n= 181)
Maternal age (years)
30-39
£40
Nonwhite race of infant
Atrial septal defect (n = 187)
Nonwhite race of infant
Bleeding in pregnancy
Previous premature birth
Paternal work in cold
4
39.8
43.3
20.9
11.2
2.1
1.5**
1.5*
2.1**
8.0**
*p £ 0.05; **p <> 0.01, level of significance in final logistic model to identify malformation-associated factors,
t AF, attributable fraction as percent; n, number of cases.
sure and paternal use of marijuana both had extra
attributable fractions over 5 percent. The relative risks
were adjusted for race of the infant (table 2), as well as
birth-time and father-at-interview.
Multiple/multiplex membranous ventricular septal
defect. The summary attributable fraction was 14.9
percent due to six potential risk factors, of which hair
dye had the largest extra attributable fraction (3.3
percent). The relative risks were adjusted for race of
infant and maternal age (table 2), as well as birth-time
and father-at-interview. The exposures to the potential
risk factors with associations significant at the 0.01
level—paternal cocaine use, diabetes mellitus, and
metronidazole—were disjoint in our data; thus, their
extra attributable fractions were equal to their marginal attributable fractions and sum exactly to their
summary attributable fraction of 8.3 percent.
Atrial septal defect. The summary attributable
fraction was 21.4 percent due to six potential risk
factors. Urinary tract infection had a small relative risk
of 1.6, but the large percent exposed (20.3 percent)
Am J Epidemiol
Vol. 148, No. 5, 1998
resulted in an extra attributable fraction of 6.4 percent.
The relative risks were adjusted for race of infant,
bleeding in pregnancy, previous premature birth (table
2), as well as father-at-interview and maternal age
over 35 years.
General comments on results. Table 1 shows that,
for a given malformation, the extra attributable fractions based on factors significant at the 0.01 level are
not identical with those based on factors significant at
the 0.05 level except when the exposures of all the
factors are disjoint. This is because, as factors are
removed from the extra attributable fraction analysis,
the extra attributable fractions of the remaining factors
increase toward their marginal attributable fractions,
somewhat analogous with the "competing risks" phenomenon.
Table 2 gives the malformation-associations that
were considered probable markers for other associations and thus not included in table 1 (except as
adjustments for the relative risks). In addition to the
relative risks and number of cases exposed, table 2
420
Wilson et al.
shows the extra attributable fraction that would hold if
all of the associated factors for a given malformation
were considered jointly potentially causal with those
in table 1.
DISCUSSION
Until recent years, cardiac defects were considered
an unfortunate occurrence with little chance for prevention (20), but a growing body of research findings
now recognizes genetic and environmental factors that
influence the occurrence of specific cardiac anomalies
in liveborn infants (1, 21-23). Using epidemiologic
methods similar to those of the Baltimore-Washington
Infant Study, other researchers have conducted casecontrol studies of infants with cardiac defects (21-23),
but none have published attributable fractions for the
genetic and environmental factors studied.
The extra attributable fraction for a given risk factor
indicates the proportion of the cases of the given
disease that might be prevented if exposure to the
factor were eliminated in the population. The concept
of attributable fraction assumes that the factor to
which it refers is causally related to the disease. That
is, the association between the factor and the disease is
not due to chance, bias, or confounding. To allow a
more cautious interpretation aimed at reducing the
possibility that the reported attributable fractions reflect chance associations, we also provided results
based on associations that were significant at the 0.01
level. Nonetheless, additional studies corroborating
the associations are required.
Spurious associations in a case-control study can
arise from selection bias. In the Baltimore-Washington
Infant Study, selection bias is not a likely explanation
for the observed associations because the study cases
represent essentially all of the cases in the study population, and the controls are a representative sample of
nondiseased infants in that population.
In the Baltimore-Washington Infant Study, data collection was conducted using standardized interview
procedures with a standardized questionnaire. One indication of adherence to standardized procedures is the
age distribution of the study infants at interview, and
we found that the distribution of age at interview was
similar for cases and controls (1, 2).
Interview data are subject to recall error, and spurious associations can result if such error differs
strongly by case-control status. Thus, in a case-control
study of birth defects based on interview data, a positive association with a given exposure may simply
reflect that control parents recalled exposure with
more error (i.e., less sensitivity) than did case parents,
even though exposure frequencies may have been the
same. This possibility should be strongly suspected
when an excess in exposure frequency is found for a
wide range of factors, including factors not likely to be
associated with disease. In the Baltimore-Washington
Infant Study, the frequencies of parental reports of
exposure for most of the nearly 200 factors examined
were similar between all malformations as a group and
controls. Furthermore, we found that case-control differences for a given factor in a given malformation
remained even when other malformation groups were
used as the control. The use of "affected" controls is
not recommended as a way to deal with recall bias (24,
25), because this approach can miss associations with
factors that have a wide range of effects. However,
when the use of affected controls has no effect on an
association observed with unaffected controls, recall
bias becomes a less tenable explanation for the association. Furthermore, it has been shown (25) that recall
bias can lead to spurious inferences only under extremely low sensitivity and specificity of recall. Thus,
it appears that recall bias is not a likely explanation for
the associations in this report. On the other hand, we
cannot rule out nondifferential misclassification of
exposure status, and this would attenuate the estimated
relative risks toward unity.
Evaluation of malformation-associations took into
account potential confounding factors. The attributable fraction results are presented only for malformation groups for which we made a thorough search for
potential effect modifying and confounding factors
available in our data set. However, we cannot exclude
the possibility of unmeasured confounders and/or residual confounding as a possible explanation for some
of the observed associations.
The known "causes" of birth defects encompass the
same spectrum of prenatal etiology as do those for
postnatal diseases: genetic, metabolic, and nutritional
disorders, infections, and environmental exposures to
chemical and physical agents, including ionizing radiation and heat (26-28). All of these etiologic categories were targets of the Baltimore-Washington Infant
Study interviews (29), and the variables shown in table
1 are potentially causal in the sense that they fall into
these recognized categories. Research on human birth
defects is not now sufficient to establish the causality
of each of these potential risk factors. In particular,
mechanisms underlying male-mediated teratogenesis
are not yet fully understood. However, animal studies
lend plausibility, and such studies have shown that
paternal exposures to chemical agents and ionizing
radiation can result in malformations in offspring (3035). In addition, human studies suggesting transmission of toxic chemicals by seminal fluid (36) and
genetic damage to male germ cells (37) have been
supported by animal studies (38-40). (See CorreaAm J Epidemiol
Vol. 148, No. 5, 1998
Heart Defect Attributable Risk
Villasenor et al. (41) for a report of paternallymediated malformation-associations in the BaltimoreWashington Infant Study.)
We must exercise caution in inferring causality of
any of the potential risk factors in table 1. However,
because of the increasing concern regarding paternally- as well as maternally-mediated teratogenesis, we
believe it can be useful to consider the attributable
fractions that would hold if these potential risk factors
are in fact causally related to the malformations.
In this context, the largest extra attributable fractions point out areas where prevention efforts could
have had the greatest impact in the years 1981-1989 in
our study area of Maryland, the District of Columbia,
and Northern Virginia by intensified attention to the
clinical recognition and treatment of illness in expectant
mothers and restriction of exposures to xenobiotic agents
before and during pregnancy. If the potential risk factors
are causal, the population impact would depend on the
frequency of occurrence of the targeted exposures.
The attributable fraction results reported here
complement our previously reported findings of
malformation-associations (1, 2), and they illustrate
the dominance of percent-of-cases-exposed over relative risk in determining attributable fraction. Often we
see that the potential risk factors with the largest extra
attributable fractions are those with a very large percent of cases exposed and only a modest relative risk.
Isolated/simplex membranous ventricular septal defect
is a striking example of this: The extra attributable
fractions are ordered directly with the ordering of the
percent exposed and inversely with the ordering of the
relative risks. (Also see maternal age in table 2.) This
has implications for prevention with important public
health consequences by focusing attention on the most
prevalent potential risk factors.
We do not know the degree to which the potential
risk factors we have identified are in fact causally
related to the malformations, or whether adjustment
for unmeasured confounding variables would alter the
relative risks. Furthermore, the largest summary attributable fraction in our results was only 30 percent,
indicating that the risk factors that account for the bulk
of the malformations are not yet identified. We present
these results to stimulate further epidemiologic research to establish the causality or non-causality of the
factors we have reported, and to identify the risk
factors that are still unknown. Our findings and such
research should engage the interest of public health
planners who could use the product of the attributable
fraction and the prevalence of specific cardiac defects
to crudely predict the number of such defects that
could be prevented if exposure to certain risks were
removed.
Am J Epidemiol Vol. 148, No. 5, 1998
421
ACKNOWLEDGMENTS
This research was supported by NHLBI grant no. R37HL25629.
The authors acknowledge the cooperation of the Baltimore-Washington Infant Study Group: Drs. Joann A.
Boughman, Joel I. Brenner, John W. Downing, Seymour
Hepner, Mohammed Mardini, Gerard R. Martin, Catherine
A. Neill, Lowell W. Perry, and Judith Rubin.
REFERENCES
1. Ferencz C, Loffredo CA, Correa-Villasenor A, et al. Genetic
and environmental risk factors of major cardiovascular
malformations: the Baltimore-Washington Infant Study:
1981-1989. Armonk, NY: Futura Publishing Co, Inc, 1997.
2. Ferencz C, Rubin JD, Loffredo CA, et al. Epidemiology of
congenital heart disease: the Baltimore-Washington Infant
Study, 1981-1989. Mount Kisco, NY: Futura Publishing Co,
Inc, 1993.
3. Wilson JG. The evolution of teratologic testing. Teratology
1979;20:205-12.
4. Kalter H. Teratology and pharmacogenetics. Ann NY Acad
Sci 1968;151:997-1000.
5. Ferencz C. A case-control study of cardiovascular malformations in live-born infants: the morphogenetic relevance of
epidemiological findings. In: Clark EB, Takao A, eds. Developmental cardiology: morphogenesis and function. Mount
Kisco, NY: Futura Publishing Co, Inc, 1990:523-39.
6. Ferencz C, Correa-Villasenor A. Overview: the epidemiologic
approach to the study of congenital cardiovascular malformations. In: Clark EB, Markwald RR, Takao A, eds. Developmental mechanisms of heart disease. Armonk, NY: Futura
Publishing Co, Inc, 1995:629-38.
7. Hosmer DW, Lemeshow S. Applied logistic regression. New
York: John Wiley & Sons, 1989.
8. Kleinbaum D, Kupper L, Morgenstern H. Epidemiological
research: principles and quantitative methods. New York: Van
Nostrand Reinhold, 1982.
9. Kleinbaum D, Kupper L, Muller K. Applied regression analysis and other multivariable methods. 2nd ed. Boston, MA:
Duxbury Press, 1987.
10. Wright SP. Adjusted p-values for simultaneous inference.
Biometrics 1992;48:1005-13.
11. Westfall PH. Testing of general contrasts using logical constraints and correlations. J Am Stat Assoc 1997;92:299-306.
12. Rothman K. No adjustments are needed for multiple comparisons. Epidemiology 1990; 1:43-6.
13. Wilson PD, Correa-Villasenor A, Loffredo CA, et al. Temporal trends in prevalence of cardiovascular malformations in
Maryland and the District of Columbia, 1981-1988. Epidemiology 1993;4:259-65.
14. Walter SD. Prevention for multifactorial diseases. Am J Epidemiol 1980;l 12:409-16.
15. Walter SD. Effects of interaction, confounding, and observational error on attributable risk estimation. Am J Epidemiol
1983;117:598-604.
16. Bruzzi P, Green SB, Byar DP, et al. Estimating the population
attributable risk for multiple risk factors using case-control
data. Am J Epidemiol 1985; 122:904-14.
17. Benichou J. Methods of adjustment for estimating the attributable risk in case-control studies: a review. Stat Med 1991;
10:1753-73.
18. Tanner MA. Tools for statistical inference. In: Berger J,
Fienberg S, Gani J, et al, eds. Lecture notes in statistics, vol
67. New York: Springer-Verlag, 1992.
19. Greenland S, Drescher K. Maximum likelihood estimation of
the attributable fraction from logistic models. Biometrics
1993;49:865-72.
422
Wilson et al.
20. Hoffman JIE. Reflections on the past, present, and future of
pediatric cardiology. Cardiol Young 1994;4:208-23.
21. Adams MM, Mulinare J, Dooley K. Risk factors for conotruncal cardiac defects in Atlanta. JACC 1989;14:432-42.
22. Shaw GM, Malcoe LH, Katz E. Maternal workplace exposures to organic solvents and congenital cardiac anomalies. J
Occup Med Toxicol 1992; 1:371-6.
23. Tikkanen J, Heinonen OP. Risk factors for conal malformations of the heart. Eur Heart J 1992;8:48-57.
24. Drews C, Greenland S, Flanders WD. The use of restricted
controls to prevent recall bias in case-control studies of reproductive outcomes. Ann Epidemiol 1993;3:86-92.
25. Khoury MJ, James LM, Erickson JD. On the use of affected
controls to address recall bias in case-control studies of birth
defects. Teratology 1994;49:273-81.
26. Shepard TH. Catalog of teratogenic agents, 8th ed. Baltimore,
MD: Johns Hopkins University Press, 1995.
27. Warkany J. Prevention of congenital malformations. Teratology 1981;23:175-89.
28. Milunsky A, Ulcickas M, Rothman KJ, et al. Maternal heat
exposure and neural tube defects. JAMA 1992;268:882-5.
29. Ferencz C. Congenital heart disease: an epidemiological and
teratological challenge. In: Ferencz C, Rubin JD, Loffredo
CA, et al. Epidemiology of congenital heart disease: the
Baltimore-Washington Infant Study, 1981-1989. Mount
Kisco, NY: Futura Publishing Co, Inc, 1993:1-15.
30. Nomura T. Parental exposure to X rays and chemicals induces
heritable tumors and anomalies in mice. Nature 1982;296:
575-7.
31. Kirk KM, Lyon MF. Induction of congenital malformations in
the offspring of male mice treated with X-rays at the premeiotic and post-meiotic stages. Mutat Res 1984,125:75-85.
32. Trasler JM, Hales BF, Robaire B. Paternal cyclophosphamide
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
treatment of rats causes fetal loss and malformations without
affecting male fertility. Nature 1985;316:144-6.
Jenkinson PC, Anderson D, Gangolli SD. Increased incidence
of abnormal fetuses in the offspring of cyclophosphamidetreated male mice. Mutat Res 1987;188:57-62.
Nagao T. Frequency of congenital defects and dominant lethals in the offspring of male mice treated with methylnitrosourea. Mutat Res 1987;177:171-8.
Nagao T. Congenital defects in the offspring of male mice
treated with ethylnitrosourea. Mutat Res 1988;202:25-33.
Hales BF, Smith S, Robaire B. Cyclophosphamide in the
seminal fluid of treated males: transmission to females by
mating and effect on pregnancy. Toxicol Appl Pharmacol
1986;27:602-ll.
Fabro S. Paternally-induced adverse pregnancy effects. Reprod Toxicol 1984;3:13-16.
Kelly SM, Robaire B, Hales BF. Paternal cyclophosphamide
treatment causes postimplantation loss via inner cell massspecific cell death. Teratology 1992;45:313-18.
Robaire B, Hales BH. Post-testicular mechanisms of malemediated developmental toxicity. In: Mattison DR, Olshan
AF, eds. Male-mediated developmental toxicity. New York:
Plenum Press, 1994:93-103.
Gandley R, Silbergeld EK. Male-mediated reproductive
toxicity: effects on the nervous system of offspring. In:
Mattison DR, Olshan AF, eds. Male-mediated developmental
toxicity. New York: Plenum Press, 1994:141-51.
Correa-Villasenor A, Ferencz C, Loffredo C, et al. Paternal
exposures and cardiovascular malformations. J Expo Anal
Environ Epidemiol 1993;3:173-85.
Benichou J, Gail MH. Variance calculations and confidence
intervals for estimates of the attributable risk based on logistic
models. Biometrics 1990;46:991-1003.
APPENDIX
Attributable fraction analysis
We computed the summary attributable fraction estimate by the second form of equation 1, which is given in
two forms to define and clarify the role of py
AF = 1 - 2 p , e x p ( - x j 0 ) = 1 - 2 exp(-xf
(1)
m
1=1
In the first form, j indexes the J risk factor patterns in the data, p7 is the proportion of cases in the study with
the jth risk factor pattern, Xj, and $ is the vector of adjusted estimates of the corresponding logistic regression
coefficients. In the second form, i indexes the m cases in the study, and x, is the vector of the risk factor values
for the ith case. Adjustment variables are not included. We used the delta method (18) on the second form of
equation 1 to obtain
var(AFp) — [2,- xf exp(-xf 0)] cov(/3) [2,- x,- exp(-xf
2
(2)
in which the subscript p on AFp indicates that the probability, Pj, of the jth risk factor pattern in the case
population is assumed to be given by pj. This assumption is justified by simulation studies of Greenland and
Drescher (19), which show that: 1) The Bruzzi et al. (16) attributable fraction estimates are not importantly
different from the full maximum likelihood estimates developed by Greenland and Drescher. 2) The attributable
fraction variance estimates developed by Benichou and Gail (42) for the Bruzzi et al. attributable fraction
estimator do not differ importantly from those of the Greenland and Drescher maximum likelihood estimates. 3)
The full maximum likelihood attributable fraction variance estimates that include the variance of the estimated
Pj's and the covariance of these estimates with those of the relative risks do not differ importantly from the
attributable fraction variance estimates that ignore these variances and the covariance.
Am J Epidemiol Vol. 148, No. 5, 1998
Heart Defect Attributable Risk
423
We computed confidence intervals based directly on attributable fraction, AF ± 1.96 standard error (AF),
rather than those based on log (1 - AF) and then transformed. Although Greenland and Drescher's simulation
studies found significant undercoverage by the "direct" intervals, they reported that the undercoverage was
unimportant. We computed both intervals and found that the log(l - AF)-based intervals were not only wider
(as noted by Greenland and Drescher) but were also shifted importantly downward relative to the direct intervals
and the point estimates.
Am J Epidemiol
Vol. 148, No. 5, 1998