Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
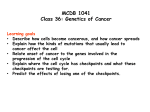
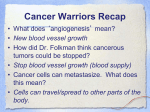
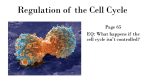
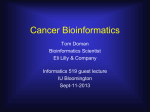
EPI242 CANCER EPIDEMIOLOGY STAGES IN NEOPLASTIC DEVELOPMENT Zuo-Feng Zhang, MD, PhD Fall, 2009 CONTENTS Carcinogenesis and stages for cancer development Molecular genetic alterations in cancer development Carcinogens Precursors CARCINOGENESIS The transformation of normal to neoplastic cells is caused by both endogenous and exogenous factors, including chemical and physical agents, viruses, activation of cancer-promoting genes, and inhibition of cancer-suppressing genes. LATENCY For infectious disease, the initial insult is the entrance of the infectious organism into the host and the latent period is the time during which the infectious organism multiplies and alters the host’s capacity for response, and manifested as the clinical apparent disease. For cancer, it refers a period of time between the initial etiologic insult and the clinical appearance of cancer, e.g., lack of parity (hormone, breast feeding) in Catholic nuns and high incidence of breast cancer; chimney sweeps (soot) as young boy and high incidence of cancer of the scrotum among adult males; and A-bomb survival and increased incidence of leukemia in Japan. MULTISTAGE CARCINOGENESIS Two stages: Initiation and Promotion. The initial two stage theory base don the natural history of epidermal carcinogenesis in the mouse has lasted for many years. The limitation of the theory is that it does not emphasize the latent period of the development of other types of neoplasms. STAGES OF CARCINOGENESIS Initiation is the first critical carcinogenic event and it is usually a reaction between a carcinogen and DNA. Two or more agents (chemicals, viruses, radiation) may act together as carcinogens. The process of initiation, the first stage in the natural history of neoplastic development, is permanent and irreversible. STAGES OF CARCINOGENESIS Promotion is induced by a stimulator of cell proliferation and enhances the carcinogenic process. A promoter, not carcinogenic in itself, enhances other agents’ carcinogenicity. The progression in promotion process is reversibility and instability. The stage of promotion can be continually modulated by a variety of environmental alterations. MULTISTAGE CARCINOGENESIS Three stages: Initiation, promotion, and progression. The two stage concept was modified and the original stage of promotion was then divided into two phases: promotion and progression. Progression phase is irreversible. Progression is a irreversible stage with demonstrated changes in the structure of the genome of the neoplastic cells. Such changes are directly related to increased growth rate, invasiveness, metastatic capability and biochemical changes of the neoplastic cell. TUMOR GROWTH In the normal proliferating tissue, a balance between cell renewal and cell death is strictly maintained In tumor growth, more cells are produced than die in a given time HUMAN CANCER-BASED TWO-HIT MODEL Two-hit model. Tumor suppressor gene such as RB gene. Knudson (1971) suggested that all types of retinoblastoma (RB) involve two separate mutations that are carried by all retinoblastoma tumor cells. In the case of sporadic retinoblastoma, he argued that both mutations occur somatically in the same retinal precursor cell. In heritable retonoblastoma, he suggested that one of the two mutations is already present at conception (germline mutation), and the second mutation occur as a somatic event (post conception). HUMAN COLON CANCER MULTIPLE STAGE MODEL Colon cancer model. The development of human cancer is a multistage process, involving a series of genetic molecular alterations. EARLY STAGE VERSUS LATE STAGE “Early stage” versus “late stage” carcinogens in epidemiologic stages. If an agent is “early stage” carcinogen, both the increase in incidence beginning with and during exposure and decrease in incidence after cessation of exposure will be delayed. If an agent is a “late stage” carcinogen, responses both to starting and ceasing of exposure will be much more rapid. The terms, “early” and “late”, are used to correlate multistage models with epidemiologic results. Those may not necessary relate directly to the stages of initiation, promotion, and progression. EARLY STAGE VERSUS LATE STAGE MOLECULAR GENETIC OF CANCER It is now recognized that the unregulated growth of cancer cells results from the sequential acquisition of somatic mutations in genes that control cell growth, differentiation, and apoptosis or that maintain the integrity of the genome Similar mutations may also be present in the germline of persons with hereditary predisposition to a variety of cancers MOLECULAR GENETIC OF CANCER Mutations can be produced by environmental mutagens such as chemical carcinogens or radiation Mutations can also arise during normal cellular metabolism, particularly from the formation of activated oxygen species DNA ENDOGENOUS DAMAGE AND REPAIR Approximately lesions/cell/day 20,000 DNA damage 1 billion DNA damage lesions/human body/second Lindahl T, Quart Biol 2000,65,127-33 GENETIC MUTATIONS AND TUMOR DEVELOPMENT Most of these mutations are of no consequence, because they either do not affect the function of the cell or are repaired by DNA repair genes, or are lost as a result of the death of the cell However, if the mutation involves genes that control growth or that protect the stability of the genome, it may give rise to a clone of cells that possess a growth advantage over their normal neighbors. Successive mutations in similar genes result in increasingly aberrant clones until a malignant phenotype eventually emerges. CELL TRANSFORMATION Malignant transformation involves somatic mutations that confer a set of common properties It is estimated that a minimum of 4-7 mutated genes are required for the transformation of a normal cell into a malignant phenotype TRANSFORMED CELLS SHARE COMMON ATTRIBUTES Autonomous generation of mitogenic signals Insensitivity to exogenous antigrowth signal Resistance to apoptosis Limitless replicative potential (immortalization) Blocked differentiation Ability to sustain angiogenesis Capacity to invade surrounding tissues Potential to metastasize ONCOGENES Oncogenes are altered version of normal genes, termed protooncogene, that regulate normal cell growth, differentiation, and survival Gain-of-function (dominant) mutations activate protooncogenes to become oncogenes and are positive effectors of the neoplastic phenotype MECHANISMS OF ONCOGENE ACTION Growth factors (IGF-1) Cell surface receptors Intracellular signal transduction pathways DNA-binding nuclear protein (transcription factors) Cell cycle proteins (cyclins and cyclin-dependent protein kinases) Inhibitors of apoptosis (bcl-2) TUMOR SUPPRESSOR GENES Tumor suppressor genes are normal genes whose products inhibit cellular proliferation. Loss-of – function (recessive) mutations inactivate the inhibitory activities of tumor suppressor genes, thereby permitting unregulated cell growth TUMOR SUPPRESSOR GENES A mutation that creates a deficiency of a normal gene product that exerts a negative regulatory control of cell growth and thereby suppresses tumor formation. Such genes encode negative transcriptional regulators of the cell cycle, signal-transduction molecules, and cell surface receptors. TUMOR SUPPRESSOR GENES Since both alleles of such tumor suppressor genes (“gatekeeper” genes) must be inactivated to produce the deficit that allows the development of a tuor, it is inferred that normal suppressor gene is dominant. The loss of heterozygosity in a tumor suppressor gene by deletion or somatic mutation of the remaining normal allele predisposes to tumor development EXAMPLE: RETINOBLASTOMA GENE (RB) AND P53 GENE The function of RB is the most critical checkpoint in the cell cycle, the inactivating mutations in RB permits unregulated cell proliferation. The mutations of p53 seem to be the most common genetic changes in human cancer. EXAMPLE: RETINOBLASTOMA GENE (RB) AND P53 GENE The p53 molecule is a negative regulator of cell division. In response to DNA damage, oncogenetic activation of other proteins, or other stresses, p53 levels rise and prevent cells from entering S phase of the cell cycle, thereby allowing time for DNA repair to take place. Inactivating mutations of p53 allow cells with damaged DNA to progress through the cell cycle. • DNA methylation—The covalent addition of a methyl group to the 5th position of cytosine within CpG dinucleotides, which are frequently located in the promoter regions of genes. Methylation can also occur in other parts of genes. DNA methylation play a key role in a number processes, including DNA repair, genome stability, and regulation of chromatin structure. (Laird PW. Molecular Medicine Today. 1997:223-229) DNA methylation and Cancer— tumor suppressor gene (Laird PW..Molecular Medicine Today. 1997:223-229) CARCINOGENS An agent that can cause cancer. The International Agency for Research on Cancer (IARC) classifies carcinogens as follows: 1) Sufficient evidence. A positive causal relationship has been established between exposure and occurrence of cancer. CARCINOGENS 2) Limited evidence. A positive causal association has been observed between exposure to the agent, for which a causal interpretation is credible, but chance, bias, confounding cannot be rolled out. CARCINOGENS 3) Inadequate evidence. Available studies are of insufficient quality, consistency or statistical power to permit a conclusion regarding the presence or absence of a causal relationship. CARCINOGENS 4) Evidence suggesting lack of carcinogenicity. Several adequate studies covering the full range of doses to which humans are known to be exposed are mutually consistent in not showing a positive association between exposure to the agent and any studied cancer at any level of exposure. OVERALL EVALUATION OF CARCINOGEN Taking all the evidence into account, the agent is assigned to one of the following categories: Group 1. The agent is carcinogenic to humans. Group 2. 2A. The evidence for human carcinogenicity is almost sufficient (probably carcinogenic). 2B. There are no human data but there is experimental evidence of carcinogenicity (possibly carcinogenic). Group 3. The agent is not classifiable as to its human carcinogenicity. Group 4. The agent is probably not carcinogenic to humans. CLASSIFICATION OF CARCINOGENIC AGENTS IN RELATION TO THEIR ACTION ON ONE OR MORE STAGES OF CARCINOGENESIS CARCINOGENS IN TOBACCO SMOKE (According to International Agency for Research on Cancer, unless otherwise noted) GROUP 1: CARCINOGENIC TO HUMANS Tobacco Smoking Tobacco Products, Smokeless 4-Aminobiphenyl (4-ABP) Benzene Cadmium Chromium 2-Naphthylamine (2-NA) Nickel Polonium-210 (Radon) Vinyl Chloride GROUP 2A: PROBABLY CARCINOGENIC TO HUMANS Acrylonitrile Benzo[a]pyrene Benzo[a]anthracene 1,3-Butadiene Dibenz(a,h)anthracene Formaldehyde N-Nitrosodiethylamine N-Nitrosodimethylamine GROUP 2B: POSSIBLY CARCINOGENIC TO HUMANS Acetaldehyde Benzo[b]fluoranthene Benzo[j]fluoranthene Benzo[k] fluoranthene Dibenz[a,h]acridine Dibenz[a,j]acridine 7H-Dibenz[c,g]carbazole GROUP 2B: POSSIBLY CARCINOGENIC TO HUMANS Dibenzo(a,i)pyrene Dibenzo(a,l)pyrene 1,1-Dimethylhydrazine Hydrazine Indeno[1,2,3-cd]pyrene Lead 5-methylchrysene GROUP 2B: POSSIBLY CARCINOGENIC TO HUMANS 4-(Methylnitrosamino)-1-(3-pyridyl)-1- butanone (NNK) 2-Nitropopane N-Nitrosodiethanolamine N-Nitrosomethylethylamine N-Nitrosomorpholine N-Nitrosonornicotine (NNN) N-Nitrosopyrrolidine GROUP 2B: POSSIBLY CARCINOGENIC TO HUMANS Quinoline ortho-Toluidine Urethane (Ethyl Carbamate) GROUP 3: UNCLASSIFIABLE AS TO CARCINOGENICITY HUMANS (LIMITED EVIDENCE) Chrysene Crotonaldehyde N-Nitrosoanabasine (NAB) N-Nitrosoanatabine (NAT) TO 2-1. Background: Theoretical model of gene-gene/environmental interaction pathway Tobacco consumption Occupational Exposures Environmental Carcinogens / Procarcinogens Exposures Ile105Val Ala114Val Environmental Exposure Null GSTP1 GSTM1 CYP1A1 MspI Ile462Val Tyr113His His139Arg PAHs, Xenobiotics, Arene, Alkine, etc Detoxified carcinogens Active carcinogens Pro187Ser mEH mEH NQO1 DNA damage repaired DNA Damage Tyr113His His139Arg Normal cell Defected DNA repair gene If DNA damage not repaired XRCC1 Arg194Trp, Arg399Gln, Arg280His M G G2 P53 P16 Arg72Pro Ala146Thr S G870A Cyclin D1 If loose cell cycle control Carcinogenesis Programmed cell death CHEMICAL/ENVIRONMENTAL CARCINOGENS Smoking and lung cancer Sun exposure and squamous cell carcinoma of skin Asbestos exposure and lung cancer Smoke food risk with nitrosamines and adenocarcinoma of the stomach Alcohol drinking and squamous cell carcinoma of esophagus Aflatoxin B1 and liver cancer Low fiber diet and adenocarcinoma of colon RADIATION Exposure to ultraviolet radiation (in the form of sunlight) and squamous cell carcinoma of skin Ionizing radiation is related to skin cancer and leukemia in radiologist VIRAL FACTORS HPV (human papilloma virus) and Cervix cancer EBV(Epstein-Barr virus) and Nasopharyngeal cancer, Burkitt’s lymphoma HBV (hepatitis B virus) and hepatocellular carcinoma HIV (human immunodeficiency virus) and Kaposi’s sarcoma PRECURSORS Is a condition which be associated with the development of cancer (Stout, 1932) Visible steps in a dynamic process of neoplasia that may or may not undergo progression to a more advanced stage of neoplasia (Foulds, 1958) All morphologic lesions on the pathway from normal tissue to cancer, up to but not including invasive cancer PRECURSORS Two groups: less advanced lesions, which do not include abnormal clones more advanced lesions or dysplasia, which include abnormal clones and are considered dangerous if untreated SIGNIFICANCE Elucidation of the etiology of precursors provides insight into etiology of the corresponding cancer Identification of etiology of precursors may provide opportunity for primary prevention for both precursors and invasive cancer If precursors are defined, they can provide targets for screening and early detection and chemoprevention of these at an increased risk of cancer They can provide functional inside into the nature of carcinogenesis ORAL LESIONS Incidence rates of leukoplakia (/1000) are 3.3-5.5 for men and 1.9-3.6 for women. 11-43% of individuals with leukoplakia may have histologically defiend dysplasia. Incidence rates for erythroplakis have not clearly defined yet. More than two thirds of cases with histologically defined dysplasia or carcinoma Incidence rates for oral submucous fibrosis (OSF) (/1,000) are 8-21 in men and 29-46 in women Oral Lesions Oral Leukoplakia 2. Invasive Head & Neck Cancer Oral submucous fibrosis Erythroplakia 3. Second Primary Cancers following a first primary oral cancer Esophageal Cancer Oral Cancer Lung Cancer PRECANCEROUS LESIONS OF CERVIX RESEARCH OPPORTUNITIES FOR PRECURSOR Precursor cellular changes hold the clue to an understanding of the mechanisms of multistep carcinogenesis Abnormal proteins formed by precursor lesions can help in the exploration of the neoplastic process as well as in the identification of high risk individuals The precursor lesions can be employed to study genetic susceptibility and environmental exposure. RESEARCH OPPORTUNITIES FOR PRECURSOR Study of progression of precursor lesions can help to determine if the etiological factors under study influence the initiation or the promotion of the neoplastic process Precursor lesions have a shorter latency period to develop as cancer. Study of precursor lesions will give researcher shorter follow-up time. The identification of precursor lesions changes offers hope of inducing the regression of lesions. This is explored in chemoprevention trials.