Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Electrocardiography wikipedia , lookup
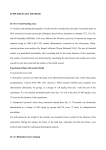
Rapid Communications Involvement of IsK-Associated K1 Channel in Heart Rate Control of Repolarization in a Murine Engineered Model of Jervell and Lange-Nielsen Syndrome Milou-Daniel Drici, Isabelle Arrighi, Christophe Chouabe, Jeffrey R. Mann, Michel Lazdunski, Georges Romey, Jacques Barhanin Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 Abstract—The Jervell and Lange-Nielsen (JLN) syndrome affects the human cardioauditory system, associating a profound bilateral deafness with an abnormally long QT interval on the ECG. It results from mutations in KVLQT1 and ISK genes that encode the 2 subunits forming the K1 channel responsible for the cardiac and inner ear slowly activating component of the delayed rectifier K1 current (IKs). A JLN mouse model that presents typical inner ear defects has been created by knocking out the isk gene (isk2/2). This study specifically reports on the cardiac phenotype counterpart, determined in the whole animal and at mRNAs and cellular levels. Surface ECG recordings of isk2/2 mice showed a longer QT interval at slow heart rates, a paradoxical shorter QT interval at fast heart rates, and an overall exacerbated QT– heart rate adaptation compared with wild-type (WT) mice. A 300-ms increase in the heart rate cycle length induces a 309621% increase in the QT duration of the WT mice versus a 500650% in isk2/2 mice (P,0.001). It is concluded that the isk gene product and/or IKs, when present, blunts the QT adaptation to heart rate variations and that steeper QT-RR relationships reflect a greater susceptibility to arrhythmias in patients lacking IKs. (Circ Res. 1998;83:95-102.) Key Words: long-QT syndrome n KCNE1 n MinK n electrocardiography n sex difference C function but also display a dominant-negative effect by partially inactivating the normal channel subunits encoded by the WT allele in heterozygous patients.16 –18 By contrast, mutations responsible for JLN syndrome have no pronounced dominant-negative effect but abolish the current in the homozygous state.16,17 Transgenic and gene-targeted mice have gained great importance as models for cardiovascular congenital affections.19,20 In order to analyze the in vivo function of the IsK protein (also referred as minK), null mutant mice with a targeted disruption of the isk gene have been engineered. At the homozygous state, these mice present the genotypic characteristics of the ISK gene–associated form of the human cardioauditory JLN syndrome. Notably, they suffer from inner ear defects strikingly similar to those observed in JLN syndrome.21–23 As in JLN patients, the mice bear a profound bilateral deafness from birth that is shown to be due to the absence of K1 secretion in the endolymph.21 However, the cardiac phenotype is still unexplored. The goal of the present study was to determine the cardiac role of IsK in this mouse model and to evaluate its putative inference in the different cardiac parameters (ie, QT duration, QT-RR adaptation, and T-wave alternans) classically associated with LQTS. The patient’s outcome is also known to be influenced by factors such as sex or bradycardia, which are explored in this model. ongenital LQTS and acquired LQTS are characterized by an abnormally prolonged ventricular repolarization, responsible for a polymorphic type of ventricular arrhythmia (known as torsades de pointes) that may lead to syncopes and sudden death. Two forms of congenital LQTS, RW and JLN, can be distinguished on the basis of the mode of transmission and specific symptoms. In the case of RW syndrome, the mode of transmission is dominant, with few clinical features, but cardiac.1,2 In the JLN syndrome, the disease is recessively transmitted and includes a profound bilateral deafness in addition to cardiac abnormalities.3 Recent information on the identity of the genes involved in both syndromes has permitted us to comprehend some of the complex gene interactions and mechanisms underlying the congenital LQTS. All the genes responsible for these syndromes identified so far are ion channel genes, including the voltage-sensitive Na1 channel gene SCN5A4 and the 3 K1 channel genes HERG,5 KVLQT1,6 and ISK (also called KCNE1).7 These latter have been shown to encode subunits of the same channel protein complex that is responsible for the slow component, IKs, of the cardiac delayed outward rectifier current, IK.8,9 Moreover, mutations in SCN5A or HERG are associated with RW syndrome only,4,5 whereas KVLQT1 and ISK can be implicated in both JLN and RW syndromes, depending on the mutation they carry.6,7,10 –15 Expression studies have shown that mutations found in RW syndrome abolish channel Received February 19, 1998; accepted May 14, 1998. From the Institut de Pharmacologie Moléculaire et Cellulaire (M.-D.D., I.A., C.C., M.L., G.R., J.B.), CNRS-UPR 411, Valbonne, France, and the Beckman Research Institute of the City of Hope (J.R.M.), Duarte, Calif. Correspondence to Jacques Barhanin, Institut de Pharmacologie Moléculaire et Cellulaire, CNRS-UPR 411, 660 route des Lucioles, Sophia Antipolis, 06560 Valbonne, France. E-mail [email protected] © 1998 American Heart Association, Inc. 95 96 QT–Heart Rate Adaptation in isk Knockout Mice Selected Abbreviations and Acronyms APD 5 action potential duration IK 5 delayed rectifier K1 current IKr 5 rapidly activating component of IK IKs 5 slowly activating component of IK JLN 5 Jervell and Lange-Nielsen LQTS 5 long-QT syndrome RW 5 Romano-Ward WT 5 wild-type Materials and Methods Animals Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 Knockout isk mice were generated by the gene-targeting methodology as previously described.21 The mutation has been maintained on the 129/Sv genetic background, and all the animals used in this study, isk2/2 and WT, are inbred 129/Sv. Mice were maintained on sterile regular rodent chow (R03, Usine d’Alimentation Rationnelle [France]) and allowed free access to food and water in a facility (at 2161°C with 12-hour light/dark cycles) monitored by the Institut de Pharmacologie Moléculaire et Cellulaire staff in full compliance with the French Government animal welfare policy. Northern Blot Analysis Total brain and heart RNAs were isolated from 3 to 6 days, 4 weeks, and 8 weeks in 129 Sv/J WT and isk2/2 mice.24 PolyA1 RNA (2 mg) was separated by electrophoresis on 1% agarose gel and transferred onto nylon membranes (Hybond N, Amersham). Blots were probed with 32P-labeled specific cDNA fragments of the different cardiac delayed rectifier K1 channel subunits in Express Hyb solution (Clontech) at 60°C for 16 hours and washed stepwise to a final stringency of 0.23 SSC and 0.3% SDS at 60°C and exposed to X OMAT AR film (Kodak). Each blot was reprobed with b-actin to control for variations in loading (not shown). Electrocardiography Animal Preparation Twelve 3-week-old (9 to 11 g each) and thirty-one 12-week-old (23 to 29 g each) male and female mice were studied. For each experiment, a mouse was anesthetized with sodium pentobarbital (10 mg/kg IP for the young ones, 45 mg/kg IP for the female adults, and 55 mg/kg IP for the male adults, SANOFI-France). Surface 3-lead ECGs (bipolar leads DI, DII, and DIII) were obtained by placement of dry electrodes carefully wrapped around each of the 4 mouse limbs. The ECG channels were amplified and filtered between 0.1 and 100 Hz, and a stable signal was reliably obtained before we proceeded. Respiratory and heart rates were continuously monitored during the procedure. A warming light was used to maintain body temperature within a range of 3661°C for prevention of hypothermia. Measurements of QT Interval Mice have a very fast heart rate, between 600 and 700 bpm. Bipolar electrodes were connected to an adjustable bandpass differential amplifier (ORTEC Inc). Signals were collected (bandwidth, 0.1 to 100 Hz), stored, and analyzed on a PC computer with PCLAMP software (Axon Instruments). The PR interval was measured from the beginning of the surface P wave to the beginning of the R-wave complex. The QRS was measured from the beginning of the Q wave, when it was present, or from the base of the R to the bottom of the S wave. The QT interval was calculated from the beginning of the Q wave (or from the base of the R wave if not possible) to the end of the T wave, defined as the point at which it returns to the isoelectric line. QT-Interval Prolongation Since the mouse heart rate is rapid, the QT intervals cannot reliably be corrected with Bazett’s formula, QTc (ms)5QT/RR (s)1/2, which is not applicable at short cycle lengths.25 For each mouse, a set of 10 to 20 RR cardiac cycle length–QT-interval pairs was obtained from their ECG recordings. The QT versus RR relation was analyzed during each experiment and was best fitted with the linear regression formula QT5A(RR)1B, where QT and RR are the observed data, and A and B are the regression parameters. This formula has been shown to be optimal for describing the QT versus RR relation at steady-state conditions. Those 2 regression parameters were used to calculate the QT interval of each mouse corresponding to predetermined RR intervals of 100 and 400 ms. QT and PR intervals were calculated in isk2/2 and in WT mice within a 150- to 600-bpm range of heart rates, which represents the RR-interval limits for which QT-interval measurement was actually feasible in our model. Cardiomyocyte Culture and Electrophysiological Recordings Primary cultures of ventricular cardiomyocytes from WT and isk2/2 mice were prepared as previously described26 with some modifications. Ventricles from 1- to 4-day-old mouse pups were dissected at 4°C and dissociated at room temperature for 15 minutes in 1.25 mg/mL trypsin in Joklik’s MEM (M0518, Sigma) with gentle agitation. Ventricles were then digested for 10 minutes with 0.5 mg/mL collagenase (type CLSII, Worthington) under gentle agitation. This was followed by mechanical dissociation using a Pasteur pipette. Cells released in the medium were centrifuged (1000 rpm for 5 minutes), collected, and washed in Joklik’s MEM. Cells obtained Figure 1. Northern blot analysis of the expression of major cardiac outward rectifier K1 channel subunits. Equal amounts (2 mg) of heart or brain polyA1 RNA from 1-, 4-, and 8-week-old animals were loaded in each lane. The expression of IsK and KvLQT1 was not detected in brain. Except for IsK, none of the intensities of the different bands in both tissues were influenced by the knockout. Drici et al July 13, 1998 97 Comparison of the QT-RR Adaptation Slopes in WT and Knockout Mice Slope of the QT-RR Adaptation isk2/2 WT Mice n Mean6SE n Mean6SE P Value Total 22 0.63760.03 21 0.79560.03 0.0006 Young 5 0.57160.06 7 0.81260.08 0.0431 Adult 17 0.65760.03 14 0.78660.04 0.0072 Male 8 0.58860.03 7 0.76260.05 0.0095 14 0.67360.03 14 0.81160.05 0.0244 Female Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 from 3 sequential collagenase digestions were pooled and plated in gelatin-coated Falcon culture dishes (diameter535 mm). The culture medium was DMEM supplemented with 10% FCS, bovine insulin (10 mg/mL), bovine transferrin (10 mg/mL), 1% chick embryo extract, and 10 nmol/L dexamethasone. Cells were used after 4 days in culture. Whole-cell transmembrane currents under voltage-clamp conditions were recorded using the patch-clamp technique.27 The culture dish was placed on the stage of an inverted microscope (Axiovert 100, Zeiss). Experiments were conducted at room temperature (22°C to 25°C). Patch pipettes (2 to 6 MV) were connected to the head stage of the recording apparatus (RK400, Bio-Logic). Stimulation and data acquisition and analysis were performed using PCLAMP software. The pipette solution contained (mmol/L) KCl 140, MgCl2 4, EGTA 1, and Na2ATP 3. This solution was buffered at pH 7.3 with 10 mmol/L HEPES/KOH. The external solution contained (mmol/L) NaCl 30, trimethyl ammonium chloride 110, CaCl2 1, KCl 5, MgCl2 1, and glucose 2. This solution was buffered at pH 7.4 with 10 mmol/L HEPES/NaOH. Statistical Analysis Results are shown as mean6SEM. Continuous variables, such as slope of adaptation, QT values, and their increase from baseline, were analyzed by ANOVA (Statview 4.5 and SuperAnova 1.11, Abacus Corp) or a Mann-Whitney-Wilcoxon rank sum test, when applicable. The Bonferroni/Dunn correction was used to adjust for multiple comparisons. A value of P,0.05 was considered statistically significant. Results Northern Blot Analysis In order to check for an eventual compensation of the isk gene knockout by a modification of the expression of other K1 channel subunits, the level of mRNA corresponding to the major cardiac IKs was analyzed at different developmental stages (Figure 1). As expected from previous work,28 the level of IsK mRNA was high in neonatal hearts and decreased with age in WT hearts. At 8 weeks, the heart IsK message reached a low but still detectable level that did not change with aging (not shown). The IsK message was totally absent in null mutants for the isk gene (Figure 1). Conversely, the amount of mRNA for the other delayed rectifier subunits, including the IsK partner KvLQT1, Kv1.5 (encoding the sustained K1 current29), and merg, the mouse counterpart of HERG, were not influenced by the absence of IsK at any age. It is particularly noteworthy that only IsK presented a strong developmental regulation. KvLQT1 expression was totally independent of that of its IsK partner, both in WT and knockout mice. Figure 2. Representative lead I surface ECG recorded from a WT female mouse (A) and an isk2/2 female mouse (B) by PCLAMP Software (Axon). P, Q, R, S, and T describe the P wave (atrial depolarization), the PR interval (atrioventricular conduction), QRS wave (ventricular depolarization), and the biphasic T wave (ventricular repolarization), respectively. A, The cycle length (RR) on the upper trace is 147 ms, with a PR at 37 ms and QT at 78 ms. On the lower trace, the increase in the cycle length (RR5247 ms) is accompanied by an increase in PR (48 ms) and QT (123 ms) intervals. The end of the T wave is indicated by an arrow in each trace. B, The cycle length (RR) on the upper trace is 162 ms, with a PR at 35 ms and QT at 109 ms. On the lower trace, the increase in the cycle length (RR5394 ms) is accompanied by an increase in PR (59 ms) and QT (239 ms) intervals. C and D, RR/QT (F, C; E, D) and RR/PR (f, C; M, D) relationships in WT (C) and isk2/2 (D) mice. Each value of QT and PR interval was measured at different heart rates. The cycle lengths sampled during these experiments ranged from 110 to 400 ms. The linear regressions fitted best the relationship as follows: QT (ms)50.52RR125 (r 250.96) and PR50.10RR121 (r 250.97) for the WT mouse and QT50.75RR219 (r 250.99) and PR50.14RR122 (r 250.91) for the isk2/2 mouse. ECG Characteristics Forty-three animals allotted as indicated in the Table were analyzed. Three bipolar lead ECGs (DI, DII, and DIII) were recorded under anesthesia, with a good stability of the signal from all 43 mice studied. Representative traces are shown in Figure 2A and 2B. The P wave as well as the PR, QRS, and QT intervals could be reliably measured in all animals. The first recordings were performed within 10 minutes of the induction of anesthesia. At this time, considered as the initial condition, the average cycle length (RR interval) was 121614 ms (95 to 150 ms, n543), the P wave duration was 2062 ms, the PR interval was 3662 ms, and the QRS interval was 1261 ms. The T wave was biphasic, with a rapid component and a slower one, and was more frequently positive than negative to the isoelectric line. The average QT duration on the first recording of the experiment was 7563 ms (44 to 130 ms, n543). During anesthesia, all animals 98 QT–Heart Rate Adaptation in isk Knockout Mice Figure 3. Left, Mean QT values (6SEM) determined from the regression line at RR intervals of 100 and 400 ms. Respective WT values were 6967 and 260610 ms (n522) compared with respective isk2/2 values of 5263 and 29169 ms (n521, P,0.05 between strains in both cases). Right, Increase of the QT interval over a 300-ms range in cycle length is 309621% in WT mice and 500650% in isk2/2 mice. *P,0.05; ***P,0.001. Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 progressively lengthened their RR intervals to an average of 247611 ms (range, 134 to 445 ms) over a 45-minute period. PR and QT intervals also increased with a similar pattern (Figure 2A and 2B). The average QT-interval duration at the end of the experiment was of 16069 ms (range, 63 to 303 ms). In our model, a linear relationship, QT (ms) or PR (ms)5A3RR (ms)1B, fitted best the QT-RR and the PR-RR interval relationships in 40 of 43 mice (average r250.9460.06, Figure 2C and 2D), with A being the slope of the QT-RR regression and B being the QT or PR intercepts for a theoretical RR value of 0. Gene-Related Modifications of the QT-RR Relationship The lengthening of the QT subsequent to bradycardia was different according to the genotype of the mouse. The isk2/2 mice had a greater adaptation of their QT interval to the lengthening of the RR interval than did the WT mice. The slope of the QT-RR adaptation was 0.63760.03 in the WT mice (n522) versus 0.79560.03 in the isk2/2 mice (n521) (P,0.001, Table). The average QT values, determined from the regression line, were longer for WT mice (6967 ms) compared with isk2/2 mice (5263 ms) (P,0.05) at an RR interval of 100 ms, corresponding to the normal heart mouse frequency of 600 bpm. At an RR interval of 400 ms (150 bpm), the QT value was greater in isk2/2 mice (29169 ms) than in WT mice (260610 ms ) (P,0.05). The resulting increase of the QT interval over a 300-ms range in cycle length was 309621% in WT mice and was significantly greater (500650% increase) in isk2/2 mice (P,0.001, Figure 3). Absence of Gene-Related Modifications of the PR Interval The PR interval lengthened progressively according to the increase in the cycle length (Figure 2). The relationship was best fitted with a linear regression. No statistical difference was seen in the RR-induced adaptation of the PR interval according to the presence or absence of the isk gene (PR50.1560.01RR11763 in isk2/2 mice [n56] and PR50.1660.03RR11664 in WT mice [n58], P50.8). At Figure 4. A, QT-RR adaptation relationships in young (n55) and adult (n517) WT mice. Young WT mice have a more blunted adaptation than their older counterparts, with an overall shorter QT. B, Overlapping QT-RR adaptation relationships in young and adult isk2/2 mice , still presenting shorter QT intervals at fast heart rates and longer ones at slow heart rates. C, Slope mean6SEM of the QT-RR adaptation of young and adult male and female mice. The difference observed between adults (0.75560.027 in females vs 0.63260.043 in males, *P,0.05) is not present before puberty (0.70360.098 in females vs 0.72360.065 in males, P50.68). an average measured cycle length of 24963 ms, where the RR-QT relationships are diverging, the average PR interval was 5561 and 5462 ms in the isk2/2 and WT mice, respectively. Influence of Age on Gene-Related Differences in the QT-RR Relationship The adaptation of the QT to RR intervals differed in WT and isk2/2 mice. Since the level of IsK mRNA drastically decreases during development, it was important to analyze the influence of age of the animals on these parameters. The QT intervals differed with aging in WT mice (Figure 4A and 4B). Although the slopes of the QT-RR relationships were only moderately changed from young to adult stages (0.57160.06 [n55] versus 0.65760.03 [n517], P,0.15; Table), the absolute QT values were significantly shorter in young mice in the whole range of heart rates (Figure 4A). The influence of age observed in WT mice was almost abolished in the isk2/2 mice, with overlapping QT-RR relationships in young and adult mice (Figure 4B; QT50.81260.08RR234612 and QT50.78660.035RR22565, respectively). This resulted in accentuated differences in the gene-dependent QT-RR adaptation in young compared with adult animals. Sex Differences The QT-RR relationship presented a higher slope in females than in males, regardless of the presence or absence of the isk gene (0.75560.027 in females versus 0.63260.043 in males, Drici et al Figure 5. Lead III surface ECG, recorded from one isk2/2 (upper trace) and one WT (lower trace) mouse, 5 minutes after an intraperitoneal injection of 200 nmol isoproterenol. The T waves become prominent in both cases, as isoproterenol induces a T-wave alternans phenomenon in both strains. Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 P,0.05; Figure 4C, left). This difference is related to the sexual maturity of the animals, since the slope of the QT-RR relationship was sex independent before puberty (0.72360.065 in males versus 0.70360.098 in females, P50.88; Figure 4C, right). There was no statistically significant interaction between gene and sex (P50.80), whereas both factors significantly influenced adaptability (gene, P,0.01; sex, P50.02). Isoproterenol Challenge In order to increase their heart rate, isk2/2 and WT mice were injected intraperitoneally with increasing doses of isoproterenol (20 and 200 nmol, n55). The shortest RR intervals attained in sinus rhythm were 9563 ms (range, 88 to 101 ms). The QT interval decreased accordingly to an average value of 5462 ms (range, 44 to 57 ms), with no noticeable difference between groups. In both groups the T wave increased significantly in amplitude (Figure 5), and at the highest dose, a T-wave alternans phenomenon developed regardless of the gene status of the mice (2 of 3 WT mice and 1 of 2 isk2/2 mice, Figure 5). K1 Current Recordings in Cultured Cardiomyocytes In order to apprehend which cellular events could be involved in the ECG changes observed in isk2/2 mice, K1 currents in cultured ventricular myocytes from both WT and isk2/2 mutant mice were analyzed. Under voltage-clamp conditions, IKs were present in both types of cells. Figure 6 (panels A and B, upper traces) shows representative K1 currents in response to depolarizing voltage pulses from a holding potential of 280 mV. Typical slow tail currents were elicited on repolarizations to 240 mV. IKr was the dominant component of IK that was present in both WT and isk2/2 mutant cells. This current was identified by its sensitivity to the specific blocker E-403130 (Figure 6, panels A and B, lower traces) and by its bell-shaped current-voltage relationship (Figure 6C). The IKs component of IK could be detected after IKr blockade by E-4031, essentially by its remaining slow tail current and its noninactivating time-dependent current at membrane poten- July 13, 1998 99 Figure 6. IK present in cultured ventricular heart cells. Representative recordings were obtained in a WT cell (A) and in an isk2/2 cell (B) in control conditions (upper traces) and after superfusion with 5 mmol/L E-4031(lower traces). IKs were superimposed in response to voltage pulses from 240 to 140 mV in 20-mV steps from a holding potential of 280 mV. Tail currents were elicited on repolarization to 240 mV. In panel C, f and M indicate the current-voltage (I-V) relationships of the E-4031– sensitive currents (obtained after subtraction) generated by experiments in panels A (f) and B (M). F and E indicate corresponding I-V curves of the current remaining at the end of the depolarizing pulse, after E-4031. Ten percent of the WT cells expressed an E-4031–insensitive IKs-like current with slow deactivating tails as in panel A. None of the isk2/2 cells displayed such a current. tials positive to 0 mV (Figure 6C). However, even if the cells analyzed originated from neonates, IKs could only be recorded in a mere 10% of the WT cells (7 of 60). Conversely, none of the mutant cells (0 of 55) exhibited this current. The E-4031–sensitive current was not significantly different according to the gene status. Because of numerous studies that implicate a contributing role for IsK to IKs8,9 and IKr,31,32 the present study was limited to these currents. Discussion The cardiac phenotype of the mice has been thoroughly investigated. In contrast to what has been previously stated,33,34 we found that the QT duration in mice not only varies with heart rate but that it does so with a strict linearity over a wide range of heart rates. Such a linearity has been reported in humans when the heart rate tends to a steady state,35 contrasting with the usual nonlinear QT-RR relationship observed in humans, rabbits, and guinea pigs under non– steady-state conditions.25,33 This is the case in the present study, with a steady anesthesia-induced lengthening of the RR interval and a beat-to-beat variability rarely exceeding a few milliseconds (not shown). Therefore, no correction of the QT values for RR intervals was necessary, avoiding correction bias.25,36 The most important result is that when IsK is present, the QT adaptation to heart rate variations is blunted in WT mice compared with isk2/2 mice. The knockout mice showed a larger lengthening of their cardiac repolarization on the decrease of the heart beat frequency. In fact, compared with WT mice, isk2/2 mice have a longer QT interval in bradycardic conditions (by 31 ms at 150 bpm, P,0.05) and a 100 QT–Heart Rate Adaptation in isk Knockout Mice Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 shorter QT interval at fast heart rates (Figure 2). Such results raise several hypotheses. In bradycardic conditions, it is likely that IKs slowly develops during the time course of the action potential in WT mice.28,37 At slow heart rates, the action potential gets longer, allowing IKs to reach a higher level, thus limiting the increase of the APD.38 As in patients suffering from LQTS resulting from ISK mutation,7,14,15,39 the absence of IKs in isk2/2 mice may result in a longer QT interval at slow heart rates. At fast heart rates, the shorter QT intervals observed in isk2/2 mice are more intriguing. The classic role attributed to IKs in shortening the APD (due to its open state accumulation at fast rates)40 does not seem to hold in our model. This finding may be relevant to the following: (1) The gene invalidated in the present mouse model is isk, which encodes the regulatory subunit, and not kvlqt1, which is responsible for the pore-forming subunit of the channel complex. When these conditions are reproduced in COS cells transfected with KvLQT1 alone, a rapidly activating smallamplitude K1 current is obtained. The presence of such a current in the isk2/2 mice could shorten the APD at fast heart rates. The fact that no KvLQT1 current was detected in either cultivated cardiomyocytes (Figure 6) or in the inner ear stria vascularis epithelium21 still does not invalidate such a hypothesis. The membrane resistance during the plateau phase of the action potential is rather high, and it is conceivable that a very small outward current (not detectable under our experimental conditions) could have a marked effect on the APD. Creation of mice with a knockout of the kvlqt1 gene instead of isk could help to verify this hypothesis. However, the human JLN syndrome was recently shown to result from mutations in either the ISK or the KVLQT1 gene, with no distinguishable clinical difference so far.14,15,39 (2) A modification of other currents involved in cardiac repolarization, such as IKur, the rapid sustained outward current, Ito, the transient outward current, or IKr, some of which having been previously linked to the isk gene,31,32 could occur. However, according to this hypothesis, the lack of IsK would diminish IKr even further or any other current that has a possible positive interaction with IsK, therefore tending to a longer QT at fast heart rates. (3) Compensation by overexpression of rapidly activating channels like IKr secondary to the isk gene knockout could contribute to a shortening of the QT at fast heart rates. (4) A dysregulation of the autonomic nervous system leading to an excessive QT shortening cannot be eliminated, given the beneficial effects of b-blockers or left stellectomy in human patients with LQTS.41,42 When cardiac parameters are compared at different developmental stages, it is found that young WT mice have shorter QT intervals than do the adults. This makes sense, considering that the amplitude of IKs is related to the amount of IsK40 and that IsK is more heavily expressed in young hearts (Figure 1). The lack of difference between the 2 ages observed in isk2/2 mice is in good agreement with this interpretation. In a way, young isk2/2 hearts look like adult ones with regard to the QT-RR relationship. A sex difference affects the outcome of both acquired and congenital LQTS, with more cardiac events in women than in men, especially after puberty.43– 45 In fact, females are known to have longer QT interval values than males in several mammalian species.46,47 The mouse complies with this rule. An obvious sex difference has been observed in adult mice in the present study (Figure 4C). Moreover, this difference is lacking in sexually immature young mice. It was of interest to investigate the inference of the isk gene on the sex difference. Although sex difference has been attributed to differences in K1 currents through genomic and nongenomic effects of sex steroid hormones,47,48 no significant interaction between gene and sex could be supported by the present study. Among several abnormalities in membrane ion currents accounting for the T-wave alternans phenomenon, IKs was a relevant candidate at fast heart rates, because of its peculiar slow deactivation.49 The fact that T-wave alternans occurs regardless of the gene status renders the involvement of the KvLQT1/IsK current unlikely. The present study clearly shows that the invalidation of the isk gene does cause alterations of the functional properties of the heart. In this study, IKs could be recorded only in cells originating from WT mice and in a small proportion of the cells analyzed. Conversely, the E- 4031–sensitive current was consistently recorded in all cells, regardless of the isk gene status. This first study was limited to IKr and IKs, since too extensive an analysis would be required to assess changes in other currents or at other developmental stages, possibly accounting for the ECG changes. However, no compensatory process resulting from the isk gene invalidation could be assessed by Northern blot analysis of heart transcripts of major K1 channel subunits. Which lessons do we gain from this mouse model? Although one must remain cautious, it appears that the change in QT-RR adaptability, which has drawn much less attention than the QT duration itself, is cardinal to the disease. Torsades de pointes ventricular arrhythmias are favored by a slow heart rate in humans. The proposed underlying mechanism is the triggering of oscillations known as early afterdepolarizations that interrupt the normal repolarizing time course of the APD, especially at slow heart rates.49,50 The lack of IKs may facilitate the occurrence of early afterdepolarizations in 2 ways: (1) by delaying the repolarization phase and lengthening the action potential first, enabling inward currents to reactivate,51 and (2) by opposing weakened outward conductances on the emergence of such depolarizations. Furthermore, the onset of torsades de pointes is constantly preceded by a sudden increase in the RR interval with an abnormally prolonged QT interval.41,50 Therefore, it is likely that LQTS patients are prone to the occurrence of such arrhythmias through an instantaneous greater adaptability of their QT interval to their heart rate. Indeed, LQTS patients have previously been shown to have a greater adaptability of both monophasic APD and QT intervals to their heart rate, at rest and during exercise.35,52–54 The isk2/2 mouse clearly is a relevant model for the JLN syndrome. The enhanced adaptability of the QT interval to the heart rate appears therefore to be a valuable criterion identifying patients at risk in an otherwise asymptomatic population of mutation carriers among relatives in RW families. Acknowledgments This study was supported by the Center National de la Recherche Scientifique (CNRS) and the Association Française contre les Drici et al Myopathies (AFM). We gratefully thank Dr André Varenne for helpful discussions. Thanks are due to Franck Aguila, Jean-Daniel Barde, Martine Jodar, Maud Larroque, and Dahvya Doume for technical assistance. References Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 1. Romano C. Congenital cardiac arrhythmia [letter]. Lancet. 1965;1: 658 – 659. 2. Ward OC. A new familial cardiac syndrome in children. J Irish Med Assoc. 1964;54:103–106. 3. Jervell A, Lange-Nielsen F. Congenital deaf-mutism, functional heart disease with prolongation of Q-T interval and sudden death. Am Heart J. 1957;54:59 – 68. 4. Wang Q, Shen JX, Splawski I, Atkinson D, Li ZZ, Robinson JL, Moss AJ, Towbin JA, Keating MT. SCN5A mutations associated with an inherited cardiac arrhythmia, long QT syndrome. Cell. 1995;80:805– 811. 5. Curran ME, Splawski I, Timothy KW, Vincent GM, Green ED, Keating MT. A molecular basis for cardiac arrhythmia: HERG mutations cause long QT syndrome. Cell. 1995;80:795– 803. 6. Wang Q, Curran ME, Splawski I, Burn TC, Millholland JM, Vanraay TJ, Shen J, Timothy KW, Vincent GM, Dejager T, Schwartz PJ, Towbin JA, Moss AJ, Atkinson D L, Landes GM, Connors TD, Keating MT. Positional cloning of a novel potassium channel gene: KVLQT1 mutations cause cardiac arrhythmias. Nat Genet. 1996;12:17–23. 7. Splawski I, Tristani-Firouzi M, Lehmannn MH, Sanguinetti MC, Keating MT. Mutations in hminK gene cause long-QT syndrome and suppress IKs function. Nat Genet. 1997;17:338 –340. 8. Barhanin J, Lesage F, Guillemare E, Fink M, Lazdunski M, Romey G. K(v)LQT1 and IsK (minK) proteins associate to form the I-Ks cardiac potassium current. Nature. 1996;384:78 – 80. 9. Sanguinetti MC, Curran ME, Zou A, Shen J, Spector PS, Atkinson DL, Keating MT. Coassembly of K(v)LQT1 and MinK (IsK) proteins to form cardiac I-Ks potassium channel. Nature. 1996;384:80 – 83. 10. Neyroud N, Tesson F, Denjoy I, Leibovici M, Donger C, Barhanin J, Faure S, Gary F, Coumel P, Petit C, Schwartz K, Guicheney P. A novel mutation in the potassium channel gene KVLQT1 causes the Jervell and Lange-Nielsen cardioauditory syndrome. Nat Genet. 1997;15:186 –189. 11. Donger C, Denjoy I, Berthet M, Neyroud N, Cruaud C, Bennaceur M, Chivoret G, Schwartz K, Coumel P, Guicheney P. KVLQT1 C-terminal missense mutation causes a forme fruste long-QT syndrome. Circulation. 1997;96:2778 –2781. 12. Neyroud N, Denjoy I, Donger C, Gary F, Villain E, Leenhardt A, Benali K, Schwartz K, Coumel P, Guicheney P. A heterozygous mutation in the pore of the potassium channel gene KvLQT1 causes an apparently normal phenotype in long QT syndrome. Eur J Hum Genet. 1998;6:129 –133. 13. Splawski I, Timothy KW, Vincent GM, Atkinson DL, Keating MT. Molecular basis of the long-QT syndrome associated with deafness. N Engl J Med. 1997;336:1562–1567. 14. Schulze-Bahr E, Wang Q, Wedekind H, Haverkamp W, Chen Q, Sun Y. KCNE1 mutations cause Jervell and Lange-Nielsen syndrome. Nat Genet. 1997;17:267–268. 15. Duggal P, Vesely MR, Wattanasirichaigoon D, Villafane J, Kaushik V, Beggs AH. Mutation of the gene for IsK associated with both Jervell and Lange-Nielsen and Romano-Ward forms of long-QT syndrome. Circulation. 1998;97:142–146. 16. Chouabe C, Neyroud N, Guicheney P, Lazdunski M, Romey G, Barhanin J. Properties of KvLQT1 K1 channel mutations in Romano-Ward and Jervell and Lange-Nielsen inherited cardiac arrhythmias. EMBO J. 1997; 16:5472–5479. 17. Wollnik B, Schroeder BC, Kubisch C, Esperer HD, Wieacker P, Jentsch TJ. Pathophysiological mechanisms of dominant and recessive KVLQT1 K1 channel mutations found in inherited cardiac arrhythmias. Hum Mol Genet. 1997;6:1943–1949. 18. Shalaby FY, Levesque PC, Yang W-P, Little WA, Conder ML, Jenkins-West T, Blanar MA. Dominant-negative KvLQT1 mutations underlie the LQT1 form of long QT syndrome. Circulation. 1997;96: 1733–1736. 19. Paigen K. A miracle enough: the power of mice. Nat Med. 1995;1: 215–220. 20. Lin MC, Rockman HA, Chien KR. Heart and lung disease in engineered mice. Nat Med. 1995;1:749 –751. 21. Vetter DE, Mann JR, Wangemann P, Liu JZ, McLaughlin KJ, Lesage F, Marcus D C, Lazdunski M, Heinemann SF, Barhanin J. Inner ear defects induced by null mutation of the IsK gene. Neuron. 1996;17:1251–1264. July 13, 1998 101 22. Friedmann I, Fraser GR, Froggatt P. Pathology of the ear in the cardioauditory syndrome of Jervell and Lange-Nielsen (recessive deafness with electrocardiographic abnormalities). J Laryngol Otol. 1966;80:451– 470. 23. Friedmann I, Fraser GR, Froggatt P. Pathology of the ear in the cardioauditory syndrome of Jervell and Lange-Nielsen: report of a third case with an appendix on possible linkage with the Rh blood group locus. J Laryngol Otol. 1968;82:883– 896. 24. Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal Biochem. 1987;162:156 –159. 25. Funck-Brentano C, Jaillon P. Rate-corrected QT interval: techniques and limitations. Am J Cardiol. 1993;72: 17B–22B. 26. Steinhelper ME, Lanson N Jr, Dresdner KP, Delcarpio JB, Wit AL, Claycomb WC, Field LJ. Proliferation in vivo and in culture of differentiated adult atrial cardiomyocytes from transgenic mice. Am J Physiol. 1990;259:H1826 –H1834. 27. Hamill OP, Marty A, Neher E, Sakmann B, Sigworth FJ. Improved patch-clamp techniques for high resolution current recording from cells and cell-free membranes patches. Pflugers Arch. 1981;391:85–100. 28. Honoré E, Attali B, Romey G, Heurteaux C, Ricard P, Lesage F, Lazdunski M, Barhanin J. Cloning, expression, pharmacology and regulation of a delayed rectifier K1 channel in mouse heart. EMBO J. 1991; 10:2805–2811. 29. Deal KK, England SK, Tamkun MM. Molecular physiology of cardiac potassium channels. Physiol Rev. 1996;76:49 – 67. 30. Spector PS, Curran ME, Keating MT, Sanguinetti MC. Class III antiarrhythmic drugs block HERG, a human cardiac delayed rectifier K1 channel: open-channel block by methanesulfonanilides. Circ Res. 1996; 78:499 –503. 31. McDonald TV, Yu ZH, Ming Z, Palma E, Meyers MB, Wang KW, Goldstein SA N, Fishman GI. A minK-HERG complex regulates the cardiac potassium current I-Kr. Nature. 1997;388:289 –292. 32. Yang T, Kupershmidt S, Roden DM. Anti-minK antisense decreases the amplitude of the rapidly activating cardiac delayed rectifier K1 current. Circ Res. 1995;77:1246 –1253. 33. Hayes E, Pugsley MK, Penz WP, Adaikan G, Walker MJ. Relationship between QaT and RR intervals in rats, guinea pigs, rabbits, and primates. J Pharmacol Toxicol Methods. 1994;32:201–207. 34. Manoach M, Fein A, Hecht Z, Varon D. A cellular basis for the prolonged QT interval in mammals. Ann N Y Acad Sci. 1992;644:84 –92. 35. Neyroud N, Maison-Blanche P, Denjoy I, Chevret S, Donger C, Dausse E, Fayn J, Badilini F, Menhabi N, Schwartz K, Guicheney P, Coumel P. Diagnostic performance of QT interval variables from 24-h electrocardiography in the long QT syndrome. Eur Heart J. 1998;19:158 –165. 36. Franz MR. Time for yet another QT correction algorithm?: Bazett and beyond [editorial comment]. J Am Coll Cardiol. 1994;23:1554 –1556. 37. Sanguinetti MC, Jurkiewicz NK. Two components of cardiac delayed rectifier K1 current: differential sensitivity to block by class-III antiarrhythmic agents. J Gen Physiol. 1990;96:195–215. 38. Hauswirth O, Noble D, Tsien RW. Separation of the pace-maker and plateau components of delayed rectification in cardiac Purkinje fibres. J Physiol (Lond). 1972;225:211–235. 39. Tyson J, Tranebjærg L, Bellman S, Wren C, Taylor J, Bathen J, Aslaksen B, Sørland SJ, Lund O, Malcolm S, Pembrey M, Bhattacharya S, BitnerGlindzicz M. IsK and KvLQT1: mutation in either of the two subunits of the slow component of the delayed rectifier potassium channel can cause Jervell and Lange-Nielsen syndrome. Hum Mol Genet. 1997;6:2179 – 2185. 40. Romey G, Attali B, Chouabe C, Abitbol I, Guillemare E, Barhanin J, Lazdunski M. Molecular mechanism and functional significance of the MinK control of the KvLQT1 channel activity. J Biol Chem. 1997;272: 16713–16716. 41. Napolitano C, Priori SG, Schwartz PJ. Torsade de pointes: mechanisms and management. Drugs. 1994;47:51– 65. 42. Schwartz PJ, Locati EH, Moss AJ, Crampton RS, Trazzi R, Ruberti U. Left cardiac sympathetic denervation in the therapy of congenital long QT syndrome: a worldwide report [comments]. Circulation. 1991;84:503–511. 43. Hashiba K. Sex differences in phenotypic manifestation and gene transmission in the Romano-Ward syndrome. Ann N Y Acad Sci. 1992;644: 142–156. 44. Makkar RR, Fromm BS, Steinman RT, Meissner MD, Lehmann MH. Female gender as a risk factor for torsades de pointes associated with cardiovascular drugs. JAMA. 1993;270:2590 –2597. 102 QT–Heart Rate Adaptation in isk Knockout Mice 45. Lehmann MH, Timothy KW, Frankovich D, Fromm BS, Keating M, Locati EH, Taggart RT, Towbin JA, Moss AJ, Schwartz PJ, Vincent GM. Age-gender influence on the rate-corrected QT interval and the QT-heart rate relation in families with genotypically characterized long QT syndrome. J Am Coll Cardiol. 1997;29:93–99. 46. Bazett H. An analysis of the time relationship of electrocardiograms. Heart. 1920;7:353–370. 47. Drici MD, Burklow TR, Haridasse V, Glazer RI, Woosley RL. Sex hormones prolong the QT interval and downregulate potassium channel expression in the rabbit heart. Circulation. 1996;94:1471–1474. 48. Busch AE, Busch GL, Ford E, Suessbrich H, Lang HJ, Greger R, Kunzelmann K, Attali B, Stuhmer W. The role of the I-sK protein in the specific pharmacological properties of the I-Ks channel complex. Br J Pharmacol. 1997;122:187–189. 49. Roden DM, Lazzara R, Rosen M, Schwartz PJ, Towbin J, Vincent GM. Multiple mechanisms in the long-QT syndrome: current knowledge, gaps, 50. 51. 52. 53. 54. and future directions: the SADS Foundation Task Force on LQTS. Circulation. 1996;94:1996 –2012. el-Sherif N, Bekheit SS, Henkin R. Quinidine-induced long QTU interval and torsade de pointes: role of bradycardia-dependent early afterdepolarizations. J Am Coll Cardiol. 1989;14:252–257. Zeng J, Rudy Y. Early afterdepolarizations in cardiac myocytes: mechanism and rate dependence. Biophys J. 1995;68:949 –964. Hirao H, Shimizu W, Kurita T, Suyama K, Aihara N, Kamakura S, Shimomura K. Frequency-dependent electrophysiologic properties of ventricular repolarization in patients with congenital long QT syndrome. J Am Coll Cardiol. 1996;28:1269 –1277. Krahn AD, Klein GJ, Yee R. Hysteresis of the RT interval with exercise: a new marker for the long- QT syndrome? Circulation. 1997;96:1551–1556. Vincent GM, Jaiswal D, Timothy KW. Effects of exercise on heart rate, QT, QTc and QT/QS2 in the Romano-Ward inherited long QT syndrome. Am J Cardiol. 1991;68:498 –503. Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 Downloaded from http://circres.ahajournals.org/ by guest on June 11, 2017 Involvement of IsK-Associated K+ Channel in Heart Rate Control of Repolarization in a Murine Engineered Model of Jervell and Lange-Nielsen Syndrome Milou-Daniel Drici, Isabelle Arrighi, Christophe Chouabe, Jeffrey R. Mann, Michel Lazdunski, Georges Romey and Jacques Barhanin Circ Res. 1998;83:95-102 doi: 10.1161/01.RES.83.1.95 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1998 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/83/1/95 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/