Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
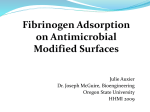
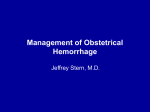
54 Fibrinogen and Factor VII in the Prediction of Coronary Risk Results From the PROCAM Study in Healthy Men Jurgen Heinrich, Leopold Balleisen, Helmut Schulte, Gerd Assmann, Jurgen van de Loo Downloaded from http://atvb.ahajournals.org/ by guest on June 11, 2017 Abstract Coronary thrombosis is regarded as the final occlusive event in the progress of coronary heart disease (CHD). Disturbances of the hemostatic system may favor this process and thus may indicate increased risk of myocardial infarction. Coagulation and lipid factors were measured in 2116 healthy male participants of the Prospective Cardiovascular Miinster (PROCAM) study. After 6 years of follow-up, 82 coronary events (9 sudden cardiac deaths and 14 fatal and 59 nonfatal myocardial infarctions) were observed. The mean plasma fibrinogen levels of the event and nonevent groups differed by 0.25 g/L (2.88 [SD, 0.68] versus 2.63 [SD, 0.63] g/L, respectively; P=.OO1). The incidence of coronary events in the upper tertile of the plasma fibrinogen distribution was 2.4-fold higher than in the lower tertile. By multiple logistic function analysis, plasma fibrinogen was found to be an independent risk indicator for CHD (P<.05). Individuals in the high serum low-density lipoprotein (LDL) cholesterol tertile who also showed high plasma fibrinogen concentrations had a 6.1-fold increase in coronary risk. Unexpectedly, individuals with low plasma fibrinogen had a low incidence of coronary events even when serum LDL cholesterol was high. The mean factor VIIc activities in the event and nonevent groups did not differ significantly (112.3% [SD, 19.9] versus 108.4% [SD, 21.6]; P=.O9). There was, however, a trend toward higher factor VIIc values when only fatal events were taken into account. Thus, higher levels of plasma fibrinogen markedly increased the predictive power of high serum LDL cholesterol. Low plasma fibrinogen is associated with low coronary risk even when LDL is raised. (Arterioscler Thromb. 1994;14:54-59.) Key Words • myocardial infarction • coronary heart disease • fibrinogen • factor VII • LDL cholesterol • smoking • prospective study M diovascular risk factors and were then kept under observation to record mortality, subsequent MI, and stroke.11 The examination at onset included each patient's history, physical examination, electrocardiogram (ECG) at rest, and a laboratory blood analysis. The study began in 1979. Two years later the determination of plasma fibrinogen and factor VIIc was included, and 10 581 individuals (7540 men and 3041 women) were recruited (Table 1). As expected, relevant numbers of MI or coronary heart disease (CHD) death occurred only in men aged 40 years and over. The analysis described below was therefore confined to the 2116 male participants between 40 and 65 years of age without a prior history of MI or stroke who had completed their 6-year follow-up. Diagnostic criteria and the definition of the end points have been published in detail.13 Two end points were considered: definite nonfatal MI and definite coronary death including sudden cardiac death and fatal MI. Sudden cardiac death was diagnosed if a subject was observed to have died within 1 hour from onset of symptoms. Fatal MI was diagnosed when a death certificate or hospital record described the cause of death accordingly or when an autopsy finding of acute MI was available. Definite nonfatal MI was diagnosed if one or more of the following conditions were fulfilled: (1) diagnostic ECG at the time of event; (2) ischemic cardiac pain plus diagnostic enzymes; (3) ischemic cardiac pain plus equivocal enzymes and equivocal ECG; or (4) an ECG that was diagnostic for MI while a previous one was not. The blinded members of the Critical Event Committee (see "Appendix") verified diagnoses and causes of death of all event cases. ost cases of acute myocardial infarction (MI) and cardiac death appear to be associated with the occurrence of occlusive coronary thrombi.1-3 One reason favoring or even precipitating thrombus formation might be a thrombogenic state in the patient's blood. Long-term epidemiological studies 4 1 0 in healthy persons report increased levels of plasma fibrinogen and factor VIIc in those individuals who develop a coronary event. This might suggest an increase in coagulation activity. To evaluate the possible role of the hemostatic system, plasma fibrinogen and factor VIIc were measured in the Prospective Cardiovascular Miinster (PROCAM) study. 1112 Since that time, plasma fibrinogen and factor VIIc have been determined in more than 10 000 persons who had not suffered from MI or stroke at the time of entry. The results from 2116 men who completed an observation period of 6 years are reported here. Methods Study Design In the PROCAM study, apparently healthy employees of Westphalian companies were examined deliberately for carReceived April 2, 1993; revision accepted September 27, 1993. From the Institute of Clinical Chemistry and Laboratory Medicine (J.H., G.A.); the Department of Internal Medicine (LB., J. van de L.); and the Institute of Arteriosclerosis Research (H.S., G.A.), University of Munster, Miinster, FRG. Correspondence to Dr J. Heinrich, Institute of Clinical Chemistry and Laboratory Medicine, A. Schweitzer-Str 33, 48149 Miinster, FRG. Blood Sample Collection Blood samples for the coagulation tests were collected in 1/10 of 3.13% trisodium citrate from 7 to 9 AM in a fasting Heinrich et al TABLE 1. Overall PROCAM Study Population and the Selection Process of the Subset Studied No. of persons Invtted to participate 33 000 No. of persons screened (total PROCAM population*) 20 060 No. of persons with complete data records 19698 No. of persons with plasma flbrlnogen and factor Vile measurements! 10 581 Male 7540 40-65 4548 Hemostasis, Llpids, and Coronary Risk 55 TABLE 2. Population Characteristics and Incidences of CHD and Other Events No. of patients studied 2116 Observation period, m 72 Mean age, y 48.9 (SD, 6.2) Age range at entry, y Annual Incidence 40-65 rate No. of CHD events 0.65% 82 Sudden cardiac deaths 9 Complete follow-up records 4084 Fatal infarctions 6-Y follow-up completed 2116 Nonfatal infarctions 59 Deaths from causes other than CHD 61 PROCAM indicates the Prospective Cardiovascular Munster study. •Recruitment period from 1979 through 1985. tFibrinogen and factor Vile were measured in all persons entering the study between 1981 and 1985. Downloaded from http://atvb.ahajournals.org/ by guest on June 11, 2017 state. Within 60 minutes plasma was separated by centrifugation of blood samples at room temperature for 15 minutes at 2500g. Serum for clinical chemistry was prepared from blood samples without additives by centrifugation for 10 minutes at 3000g. Serum and plasma, transferred in aliquots into plastic tubes, were kept in liquid nitrogen until they were stored in the laboratory at -70°C. Fibrinogen Clottable plasma fibrinogen was determined according to Gauss 14 by using thrombin and control plasma from Behringwerke, Marburg, FRG, and a plasma pool. Factor Vile Plasma factor VIIc was determined by a one-step assay13 using thromboplastin (Thromborel), factor VH-deficient plasma, and control plasma from Behringwerke and a plasma pool. Total, HDL, and LDL Cholesterol and Trigtycerides Triglycerides and total and high-density lipoprotein cholesterol (HDL-C) were measured in serum by using en2ymatic assays and (for the latter) a precipitation method from Boehringer Mannheim, FRG, on a Hitachi 737 autoanalyzer. Lowdensity lipoprotein cholesterol (LDL-C) was calculated by the Friedewald formula. Statistics An explorative analysis of data was performed. Continuous variables were compared by t test (triglycerides after logarithmic transformation), and discrete parameters were compared by the x2 t e s t - 1° a " analyses, except where age was included as an independent variable in the multiple logistic regression, results are age adjusted using regressions derived from the entry data. For additional description of the relation between a specific variable and the probability of suffering a cardiovascular event, the numbers in tertiles of the variable are given. In addition, a multiple logistic analysis was performed; variables included were age, body mass index, systolic blood pressure, cholesterol, HDL-C, triglycerides, uric acid, fasting blood glucose, diabetes mellitus, angina pectoris, smoking, and a family history of MI. The level of significance was fixed at P<.05. The statistical analysis was done with the software packages SPSS" and SAS. 14 Other diseases of the circulatory system Malignant neoplasms 8 27 Accidents and violence 15 Other diseases 11 Nonfatal strokes 11 No events In 6 y 1962 CHD indicates coronary heart disease. Results The 2116 subjects were observed for 72 months. Their mean age at entry was 48.9 (SD, 6.2; range, 40 through 65) years. In this group 82 coronary events were observed (9 sudden cardiac deaths and 14 fatal and 59 nonfatal Mis), which corresponds to an annual incidence rate of 0.65% (Table 2). Causes other than CHD accounted for 61 deaths (8 from other diseases of the circulatory system, 27 from malignant neoplasms, 15 from accidents or violence, and 11 from other diseases). Additionally, 11 nonfatal strokes were observed. A total of 1962 subjects did not experience a stroke or MI during the 6 years after examination. Table 3, which compares the event and nonevent groups, shows significantly higher levels of fibrinogen, total cholesterol, LDL-C, triglycerides, and systolic blood pressure in men who suffered a coronary event. Their HDL-C was significantly lower. The mean fibrinogen concentration was 0.25 g/L higher in the event group than in the healthy, asymptomatic population (F=.001). Factor VIIc activity did not differ significantly (112.3% [SD, 19.9] versus 108.4% [SD, 21.6], respectively; P=.09). However, when only fatal events were considered, this difference was more pronounced (117.0% [SD, 11.7] versus 108.4% [SD, 21.6], respectively; P=.O6). The number of coronary events in tertiles of variables is shown in Table 4. It confirms the information of Table 3 except for the body mass index. Body mass index, diastolic blood pressure, and factor VIIc were associated with an approximately 1.5-fold higher number of events when comparing the lower with the upper tertile. In the event group, 45.1% of the individuals were active cigarette smokers compared with 27.8% in the nonevent group. A total of 1089 nonsmokers had low or medium fibrinogen levels (<2.77 g/L); only 29 (2.7%) of 56 Arteriosclerosis and Thrombosis Vol 14, No 1 January 1994 TABLE 3. Age-Adjusted Mean Values of Coagulation, LJpId, and Other Variables In the Groups With and Without Coronary Events Variable No Event (n=1962) Fibrinogen, g/L 2.63 (0.63) Event (n=82) P .001 2.88 (0.68) Factor Vile, % 108.4 (21.6) 112.3 (19.9) .086 Cholesterol, mg/dL 225.0 (40.6) 251.6 (48.1) <.001 HDL-C, mg/dL 45.6 (11.6) 40.2 (10.9) <.001 LDL-C, mg/dL 148.5 (35.6) 175.0 (38.3) <.0O1 Triglycerides, mg/dL* 136.4 163.4 .003 Systolic BP, mm Hg 132.5 (18.3) 137.9 (21.5) .03 Dlastollc BP, mm Hg 87.2 (11.0) 89.8 (12.3) .06 BMI, kg/m 2 26.1 (3.0) 26.4 (3.0) .44 HDL-C indicates high-density lipoprotein cholesterol; LDL-C, low-density llpoprotein cholesterol; BP, blood pressure; and BMI, body mass index. Numbers in parentheses are standard deviations. *Geometric mean. Downloaded from http://atvb.ahajournals.org/ by guest on June 11, 2017 them suffered a coronary event. In contrast, 24 (7.9%) of 304 smokers with fibrinogen levels >2.77 g/L belonged to the event group (Table 5). To elucidate the interdependence of different variables to an increased coronary risk, the multiple logistic function (MLF) was applied. The standardized coefficient of logistic regression for fibrinogen was .00465 ± .00134 (P<.001). Applying the MLF analysis, this coefficient remained greater than zero (.00352±.00140, P=.O2) after taking into account age, systolic blood pressure, smoking, diabetes mellitus, angina pectoris, and family history of MI. Allowing in addition for total cholesterol and HDL-C, significance was still reached (.00299±.00147, P=.O5). The distribution of coronary events among quintiles of the estimated risk by MLF resulted in only 26.9 CHD cases/1000 in 6 years in the three lowest quintiles, taking into account the following factors: age, systolic blood pressure, total cholesterol, HDL-C, diabetes mellitus, angina pectoris, smoking, a family history of MI, and fibrinogen (Fig 1). Thus, in 60% of all participants only 13% of all events occurred. However, not taking into account fibrinogen, 59% of all TABLE 4. events were found in the highest quintile of the MLF. The addition of fibrinogen resulted in 129.6 events/1000 in 6 years, ie, 65% of all cases. Three-dimensional analysis of event rate, fibrinogen, and LDL-C, with the latter two depicted in their tertiles, revealed a 6.1-fold higher coronary risk for individuals with high LDL-C and high fibrinogen compared with those with high LDL-C but low fibrinogen (103.1 versus 16.9 events/1000 in 6 years, respectively; Fig 2). Individuals with high fibrinogen values had a more than twofold risk even if LDL-C was low (48.4 versus 19.0 events, respectively). However, low fibrinogen was still associated with a lower event rate even if the LDL values were high. Discussion Several prospective studies 49 report an association of plasma fibrinogen with the risk of cardiovascular disease. Differences between the annual incidence rates in these studies are mainly dependent on the age at entry. This could account for minor differences in the results. The sample studied here had a comparatively low mean Number of Coronary Events by Tertlles of Coagulation and LJpId and Other Variables No. of Events In Tertlles Variable Rbrinogen, g/L Factor Vile, % TertJIe Cutting Points Low Middle High 2.36 and 2.77 17 25 40 99and115 23 26 33 207 and 242 15 20 47 HDL-C, mg/dL 39 and 49 46 20 16 LDL-C, mg/dL 132 and 163 13 17 50 Triglycerides, mg/dL 106 and 169 20 24 38 Systolic BP, mm Hg 123 and 138 21 23 38 Diastolic BP, mm Hg 81 and 91 23 24 35 24.7 and 27.0 24 25 33 Cholesterol, mg/dL BMI, kg/m 2 HDL-C indicates high-density llpoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; BP, blood pressure; and BMI, body mass Index. Heinrich et al Hemostasis, Lipids, and Coronary Risk 57 TABLE 5. Absolute and Relative Numbers of Smokers and Nonsmokers Distributed by Coronary Events and Tertiles of Fibrinogen Level Fibrinogen Smoker Nonsmoker Low Without event With event Individuals with event, % High Low 484 357 90 182 280 11 18 16 6 7 24 6.3 3.7 1.9 Middle Middle High 576 3.6 4.3 7.9 Cutting points for tertiles of fibrinogen level were 2.36 and 2.77 g/L Downloaded from http://atvb.ahajournals.org/ by guest on June 11, 2017 age at entry of 48.9 years and a low annual incidence rate of 0.65%, whereas the corresponding figures for the Northwick Park Heart (NPH) study were 52.4 years and 0.8%, respectively.7 The distribution of events to tertiles of plasma fibrinogen was similar in the NPH and PROCAM studies; the odds ratio of incidences in the lower and upper tertiles was 2.4 in our study. In the NPH study the odds ratio was 3.2 for ischemic heart disease events within 5 years of entry and 2.1 for events in the whole observation period, respectively.7 In a recent meta-analysis of six prospective studies by Ernst and Resch10 surveying more than 90 000 personyears, plasma fibrinogen was confirmed as an independent risk factor for CHD. However, the studies surveyed differed in design. Most did not take HDL-C and family history of CHD into account. The latter variables have an important effect on the risk of MI and may also be related to plasma fibrinogen. In particular, factors affecting fibrinogen (eg, smoking and body weight) also alter HDL-C values.11 Moreover, fibrinogen concentrations may have a strong genetic component, identified by Humphries et al16 by using restriction fragment length polymorphism markers of the fibrinogen locus. In the PROCAM study the independent association of fibrinogen with the risk of CHD was demonstrated even after the addition of HDL-C and family history of CHD to the risk factors in the MLF analysis. In the 21-year follow-up of the Gothenburg study,5 plasma fibrinogen was found to be an independent risk factor for stroke but not for CHD if smoking was included in the multivariate analysis. This is not confirmed by our findings; even after addition of smoking to the MLF, plasma fibrinogen remained significant. The simultaneous consideration of event rate, serum LDL-C, and plasma fibrinogen confirmed the independent risk association of the two plasma factors (see the MLF analysis). High fibrinogen added markedly to the predictive power of high LDL. Unexpectedly, however, low fibrinogen appeared to counterbalance the clear-cut risk association of high LDL-C. This latter observation is so far unexplained and needs further analysis. It is of further interest to consider the CHD frequency in nonsmokers and smokers in relation to fibrinogen (Table 5). A smoker with a high fibrinogen level had a fourfold elevated risk of CHD compared with a nonsmoker with low fibrinogen. This accords with other reports.1718 The precise pathophysiological relation of fibrinogen and risk of CHD is currently unknown. Increased fibrinogen concentrations could adversely affect plasma viscosity and platelet aggregability. On the other hand, atherosclerosis could secondarily cause increases of fibrinogen as an acute-phase protein. In support of the latter hypothesis are observations of higher leukocyte counts in the event groups of other studies919-20 and significantly higher levels of C-reactive protein in angina pectoris patients who develop a coronary event within 2 years.21 In 1987, preliminary follow-up data from the coagulation part of the PROCAM study22 showed that the CHD-incidences in 6 years/1000 160 129-6 140 120 Fra 1. Bar graph showing coronary Incidences according to quintiles of estimated risk by multiple logistic function (MLF) analysis. A, Independent variables are age, systolic blood pressure, total and high-density llpoprotein cholesterol, diabetes mellitus, angina pectoris, smoking, and a family history of myocardial infarction. B, Same as A plus fibrinogen. CHD indicates coronary heart disease. 100 80 60 40 20 4,9 4,9 o• II III IV Quintiles of estimated risk by MLF 58 Arteriosclerosis and Thrombosis Vol 14, No 1 January 1994 CHD-incidenoes in 6 years/1000 FIG 2. Three-dimensional bar graph showing number of coronary heart disease (CHD) incidences/1000 in 6 years broken down by fibrinogen and low-density lipoprotein (LDL) cholesterol (n=1983; 80 events). The numbers in parentheses are the number of CHD events per number of individuals in the specified subgroup. Fibrinogen: low, <2.36 g/L; middle, 2.36-2.77 g/L; high, >2.77 g/L; LDL cholesterol: low, <132 mg/dL; middle, 132-163 mg/dL; high, >163 mg/dL. low low middle high LDL c h o l e s t e r o l (tertile) fibrinogen (tertile) Downloaded from http://atvb.ahajournals.org/ by guest on June 11, 2017 mean factor VIIc activity in the coronary event group (n=15) was 10% higher compared with the group without an event (n = 1659; P=.O7). This trend toward higher factor VIIc activity for all CHD events was confirmed in the present study as well as having been shown after 5 years of observation in the NPH study (117.4% in event versus 107.0% in nonevent cases; /><.OO1).7 When only fatal events were taken into account, the difference was more pronounced in both studies: 123.9% (SD, 27.7) versus 107.0% (SD, 25.1), P<.001, in the NPH study and 117.0% (SD, 11.7) versus 108.4% (SD, 21.6), P=.O6, in the PROCAM study. To evaluate possible differences of methodology, a laboratory comparison has been performed23 that includes the factor VII assays of the NPH, Atherosclerosis Risk in Communities,24 and PROCAM studies. Plasma samples enriched with activated factor VII (factor Vila) expressed a proportionately greater factor VIIc in the NPH assay using mixed human and bovine thromboplastin than in the Munster pure human system. It could also be shown that the converse held in samples that were relatively deficient in factor Vila. These differences in test results may be important if part of the clear association of the risk of CHD with factor VII activity, as found in the NPH study, is due to the presence of increased circulating levels of factor Vila. Based on our results, fibrinogen should be considered as a powerful independent risk factor of CHD and should be taken into account in CHD risk algorithms. In other words, the individual prediction of coronary risk may be markedly improved by applying risk scores that include plasma fibrinogen. Acknowledgments This study was supported by Bundesministerium fur Forschung und Technologies Ministerium fur Wissenschaft und Forschung NRW; Deutsche Forschungsgemeinschaft; and Landesversicherungsanstalten Westfalen und Rheinprovinz. The excellent technical cooperation of M. Kase, J. Bailey, and C. Sandau is gratefully acknowledged. Appendix Members of the Critical Event Committee included K. Kochsiek, MD, Wurzburg; B.E. Strauer, MD, Dusseldorf; U. Gleichmann, MD, Bad Oeynhausen; and R. Uebis, MD, Aachen, FRG. References 1. Schwartz CJ. Thrombosis in the pathogenesis of sudden cardiac death and myocardiaJ infarction. In: Oates JA, ed. Prostaglandins and the Cardiovascular System. New York, NY: Raven Press, Publishers; 1982:1-14. 2. Davies MJ, Woolf N, Robertson WB. Pathology of acute myocardial infarction with particular reference to occlusive coronary thrombi. Br Heart J. 1976;38:659-664. 3. Davies MJ, Thomas A. Thrombosis and acute coronary-artery lesions in sudden cardiac ischemic death. N EnglJMed. 1984^310: 1137-1140. 4. Wilhelmsen L, SvSrdsudd K, Korsan-Bengtsen K, Larsson B, Welin L, Tibblin G. Fibrinogen as a risk factor for stroke and myocardial infarction. N EnglJ Med. 1984;311:501-505. 5. Eriksson H, Korsan-Bengtsen K, Welin L, SvSrdsudd K, Larsson B, Tibblin G, Wilhelmsen L. 21-year follow up of CHD and total mortality among men born in 1913. In: Ernst E, Koenig W, Lowe GDO, Meade TW, eds. Fibrinogen; A "New" Cardiovascular Risk Factor. Vienna, Austria: Blackwell; 1992:115-119. 6. Stone MC, Thorp JM. Plasma fibrinogen: a major coronary risk factor. J RCoUGen Pract (Occas Pap). 1985^5:565-569. 7. Meade TW, Brozovic M, Chakrabarti RR, Haines AP, Imeson JD, Mellows S, Miller GJ, North WRS, Stirling Y, Thompson SG. Haemostatic function and ischaemic heart disease: principal results of the Northwick Park Heart Study. Lancet 1986;2:533-537. 8. Kannel WB, Wolf PA Castelli WP, D'Agostino RB. Fibrinogen and risk of cardiovascular disease: the Framingham Study. JAMA. 1987;258:1183-1186. 9. Yarnell JWG, Baker IA, Sweetnam PM, Bainton D, O'Brien JR, Wnitehead PJ, Ehvood PC. Fibrinogen, viscosity, and white blood cell count are risk factors for ischemic heart disease. Circulation. 1991;83:836-844. 10. Ernst E, Resch KL. Fibrinogen as a cardiovascular risk factor a meta-analysis and review of the literature. Ann Int Med. 1993;118: 956-963. 11. Balleisen L, Bailey J, Epping P-H, Schulte H, van de Loo J. Epidemiological study on factor VII, factor VIII and fibrinogen in an industrial population, I: baseline data on the relation to age, gender, body-weight, smoking, alcohol, pill-using, and menopause. Thromb Haemost. 1985^4:475-479. 12. Balleisen L, Bailey J, Epping P-H, Schulte H, van de Loo J. Epidemiological study on factor VII, factor VIII and fibrinogen in an industrial population, II: baseline data on the relation to blood Heinrich et al 13. 14. 15. 16. 17. 18. pressure, blood glucose, uric acid, and lipid fractions. Thromb Haemost. 1985^4:721-723. Assmann G, Schulte H. Relation of high density lipoprotein cholesterol and triglycerides to incidence of atherosclerotic coronary artery disease: the PROCAM experience. Am J Cardiol 1992;7(h 733-737. Clauss A, Gerinnungsphysiologische Schnelhnethode zur Bestimraung des Fibrinogens. Acta Haematol 1957;17:237-246. Lechner K. Blutgerinnungsstdrungen: Bestimmung von Faktor VH1. Berlin and Heidelberg, FRG, and New York, NY: SpringerVerlag; 1982:185-186. Humphries SE, Cook M, Dubowitz M, Stirling Y, Meade TW. Role of genetic variation at the fibrinogen locus in determination of plasma fibrinogen concentrations. Lancet. 1987;1:1452-1455. Meade TW, Imeson J, Stirling Y. Effects of changes in smoking and other characteristics on clotting factors and the risk of ischemic heart disease. Lancet. 1987;2:986-988. Kannel WB, D'Agostino RB, Belanger AJ. Fibrinogen, cigarette smoking and risk of cardiovascular disease: insights from the Framingham study. Am Heart J. 1987;113:10O6-1010. Hemostasis, LJpids, and Coronary Risk 59 19. Friedmann GD, Klatsky AL, Siegelaub AB. The leucocyte count as a predictor of myocardial infarction. N EnglJMed. 1974^90:1275-1278. 20. Phillips AN, Neaton JD, Cook DG, Grimm RH, Shaper AG. Leukocyte count and risk of major heart disease events. Am J Epidemiol 1992;136:59-70. 21. Haverkate F. Is the increase of fibrinogen as a cardiovascular risk factor associated with acute-phase reaction? In: Ernst E, Kocnig W, Lowe GDO, Meade TW, eds. Fibrinogen: A "New" Cardiovascular Risk Factor. Vienna, Austria: Blackwell; 1992:298-300. 22. BaUeisen L, Schulte H, Assmann G, Epping PH, van de Loo J. Coagulation factors and the progress of coronary heart disease. Lancet. 1987;2:461. Letter. 23. Miller GJ, Stirling Y, Heinrich J, van de Loo J, Kienast J, Wu KK, Morrissey JH, Esnouf MP, Meade TW, Martin JC, Imeson JD, Cooper JA, Finch A. Factor Vll-deficient substrate plasma depleted of protein C raises the sensitivity of the factor VII bio-assay to activated factor VII in test samples: results of an international collaborative study. Thromb Haemost. In press. 24. The ARIC Investigators. The atherosclerosis in communities (ARIC) study: design and objectives. Am J Epidemiol 1989;129: 687-702. Downloaded from http://atvb.ahajournals.org/ by guest on June 11, 2017 Downloaded from http://atvb.ahajournals.org/ by guest on June 11, 2017 Fibrinogen and factor VII in the prediction of coronary risk. Results from the PROCAM study in healthy men. J Heinrich, L Balleisen, H Schulte, G Assmann and J van de Loo Arterioscler Thromb Vasc Biol. 1994;14:54-59 doi: 10.1161/01.ATV.14.1.54 Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1994 American Heart Association, Inc. All rights reserved. Print ISSN: 1079-5642. Online ISSN: 1524-4636 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://atvb.ahajournals.org/content/14/1/54 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online at: http://atvb.ahajournals.org//subscriptions/