Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
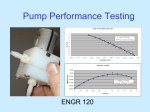
2010 American Control Conference Marriott Waterfront, Baltimore, MD, USA June 30-July 02, 2010 ThB13.3 Modeling and control of an implantable rotary blood pump for heart failure patients Abdul-Hakeem H. AlOmari, Andrey V. Savkin, Peter J. Ayre, Einly Lim, and Nigel H. Lovell Abstract—We propose a dynamical model for mean inlet pressure estimation in an implantable rotary blood pump (IRBP). Noninvasive measurements of pump impeller rotational speed, motor power, and pulse width modulation signal (PWM) to the motor controller were used as inputs to the model. Linear regression between estimated and measured inlet pressure resulted in a highly significant correlation (R2 = 0.9503) and small mean absolute error (e = 2.31 mmHg). The proposed model was also used to design a controller to regulate pump inlet pressure using noninvasively measured pump rotational speed and motor power. The control algorithm was tested using both constant and square wave reference inputs. In the presence of models uncertainties, the controller was able to track and settle to the desired input within a finite number of sampling periods with minimal error. I. INTRODUCTION H EART failure is an abnormal health condition in which the heart is unable to pump effectively and thus cannot supply sufficient blood to cope with the body’s physiological demands. The lack of donor organs for heart transplantation has led to a range of treatment options for heart failure patients. Implantable rotary blood pumps (IRBPs) are emerging as a viable long-term treatment alternative for heart failure patients. Small size and light weight are the most important design aspects which make the third generation of rotary blood pumps (RBPs) easily implanted inside the patient’s body. This increases the potential for the patients to leave the hospital and resume normal lives. The VentrAssist® (Ventracor Limited, Sydney, NSW, Australia) left ventricular assist device (LVAD) shown in Fig. 1 is a third generation RBP. The pump is to be integrated with a cardiac assist system primarily designed as a permanent option to heart transplant. Fig. 2 shows a diagram of the LVAD connection to the patient’s native heart and the controller. Non-invasive control of an IRBP is one of the most vital design goals in providing long-term alternative treatment for congestive heart failure patients. Implantation of sensors is not reliable as they result in thrombus formation and require regular calibration due to measurement drifts which makes Manuscript received September 22, 2009. Abdul-Hakeem H. AlOmari and Andrey V. Savkin are with the School of Electrical Engineering and Telecommunications, The University of New South Wales (UNSW), Sydney, NSW 2052, Australia (phone: +61 (2) 9385 4918; fax: +61 (2) 9385 5993; (e-mail: [email protected]; a. [email protected]). Nigel H. Lovell, Einly Lim and Peter J. Ayre are with the Graduate School of Biomedical Engineering, The University of New South Wales (UNSW), Sydney, NSW 2052, Australia (e-mail: [email protected]; [email protected]; [email protected]). 978-1-4244-7425-7/10/$26.00 ©2010 AACC long-term implantation of such devices problematic. Previously, we developed stable dynamical models to noninvasively estimate the pulsatile flow and differential pressure in a rotary blood pump [1]. The proposed models were successfully used to design control algorithms for continuous and pulsatile flow [2]. Non-invasive measurements of pump rotational speed, power, noninvasively estimated flow, and differential pressure were used as inputs to the controller. The control algorithm was evaluated using a lumped-parameter model of the cardiovascular system (CVS) previously designed and verified in our laboratory [3]. In the presence of model uncertainty, our results showed that the pulsatile flow controller was able to track the reference inputs with minimal error, finite number of sampling periods and minimum steady-state error. Fig. 1. VentrAssist® as an example of a third generation IRBP (Ventracor Limited, Sydney, NSW, Australia). The existing most popular control strategies of IRBPs are the pump differential pressure control [4, 5], pulsatility control [6-11], and target speed control [12, 13]. Choi et al. [8] developed a fuzzy logic controller for an axial blood pump based on the blood flow pulsatility which was estimated using a validated pump model. Using unrealistic assumptions which included no heart valves, continuous flow throughout the circulatory system, and linear correlation between pump differential pressure, voltage, current, and rotational speed, Waters et al. [13] developed a proportionalintegral (PI) controller to adjust the motor speed and maintain the system reference differential pressure when changes occurred in the natural heart. Zhou et al. [14] used a nonlinear static model of the pump to model the hemodynamic responses of the assisted circulatory system as a function of different constant speeds of the pump and concluded that the developed integrated circulatory system ventricular assisted device (VAD) model could be used to develop different VAD control algorithms. 3574 Others [15] have used a model-based estimation method to estimate the differential pressure across the pump which was used as an input to a control system of the IRBP. Using a state-space model of the circulatory system together with measurements of pump differential pressure, Wu et al. [16] developed their control algorithms to control the aortic pressure. On the other hand, Bullister et al. [17] have designed hierarchical control algorithms to control the speed of the pump based on feedback from pressure sensors measuring pump inlet and outlet pressures. stroke volume depends on left ventricle end diastolic volume (Frank-Starling mechanism). Therefore, one design requirement of an IRBP is to simulate the Frank-Starling law. In patients with a left ventricle assisted by an IRBP, when the volume in left ventricle is low, inlet pressure will automatically decrease. This may cause suction if the same target speed was maintained. By applying inlet pressure control, target speed will be reduced to increase the inlet pressure to avoid suction. This shows one example that makes the problem of non-invasive estimation and control of inlet pressure during the diastolic period of considerable benefit. The primary objective of the proposed deadbeat controller is to avoid undesired pumping states such as suction by regulating the inlet pressure within a predefined physiologically reasonable limit. II. MATERIALS AND METHODS Fig. 2. Illustration of how VentrAssist® is implanted and connected. As shown, a short inflow cannula is attached to left ventricle. The outflow cannula returns the blood to the ascending aorta and the percutaneous lead connects the IRBP to the external controller and batteries (Ventracor Limited, Sydney, NSW, Australia). One limitation of the majority of the previously designed control algorithms was that the estimation of differential pressure and flow were performed using steady state models without data relating to the transient response of the pump. Furthermore, they required the implantation of additional sensors to provide measurements of parameters used as inputs to their corresponding control algorithms. For the first time, in the present study, we used noninvasive measurements of rotational pump speed, motor power, together with the pulse width modulation (PWM) signal as inputs to a new dynamical autoregressive with exogenous inputs (ARX) model to estimate average inlet pressure during the diastolic period. The resulting model is stable and simple, thus offering a tractable control design problem. The average inlet pressure estimation model was validated using in vivo animal data obtained from acute implantation of a VentrAssist® (Ventracor Limited, Sydney, Australia) LVAD in dogs under heart failure conditions. Also, the model developed herein was used to design a deadbeat controller that non-invasively controls and regulates the inlet pressure of the pump. In the VentrAssist®, during ventricular collapse state, the inlet pressure during the diastolic period may be as low as 160 mmHg, and varies between + 10 mmHg during normal pump operation. During diastole, the inlet pressure and left ventricular end diastolic pressure (preload to the left ventricle) are closely related. In normal human hearts, the A. In vivo acute dog experiments The VentrAssist® centrifugal heart pump was acutely implanted in four healthy dogs. In each dog, the inflow pump cannula was inserted into the apex of the left ventricle while the outflow cannula was anastomosed to the ascending aorta as shown in Fig. 3. The dogs were instrumented with indwelling catheters (DwellCath, Tuta Labs, Lane Cave, NSW, Australia) to measure the left ventricular (LVP), left atrial (LAP), aortic (AoP), pulmonary arterial (PAP) , central venous (CVP), pump inlet (Pin) and outlet pressures (Pout). Pump (Qp) and aortic valve (Qao) flows were measured by ultrasonic flow probes (Transonic Systems Inc., Ithaca, NY, USA). Qp, Pin, and Pout were obtained near the inlet and outlet of the pump. Furthermore, the instantaneous pump impeller rotational speed (), motor current (I), supply voltage (V), and pulse-width modulation signal (PWM) were continuously monitored from the pump controller and recorded for further analysis. All the aforementioned signals were recorded using a Powerlab data acquisition system (ADInstruments, Castle Hill, NSW, Australia). To mimic acute heart failure conditions and reduce the cardiac contractility, the beta blocker metoprolol was administrated until the total cardiac output fell to approximately 50% of its baseline. Responses to three different blood volume levels: low, medium, and high, were studied by varying the rate of the cardiotomy suction machine. For each volume level, each dog underwent several speed ramp tests in which impeller speed was increased from 1250 rpm to 3000 rpm in a stepwise increment of 100 rpm with each step lasting for 30 seconds. Blood samples were taken regularly during the experiments for measurements of the hematocrit (HCT) values. The sampling rate was set at 4 kHz for data recordings, but, in further analysis, the data were down-sampled to 50 Hz. B. Dynamical modeling In another study performed by our research group [1], we 3575 developed stable dynamical models for pulsatile flow and differential pressure estimation in an IRBP. The main requirement for the pulsatile flow model was that any steadystate solution of the model can be described by a previously designed and verified static model. Also, any steady-state solution for the dynamical model should be stable. Both models were validated and verified using data obtained from ex vivo pig experiments and pulsatile mock loop. To summarize, a non-invasive, steady-state average flow (Qss) estimator was designed in a non-pulsatile environment for the IRBP. The estimator was based on the input power (P) and rotational speed (). u1 (kh) P(kh), (5) u2 (kh) (kh) , (6) u3 (kh) f (kh), (7) u4 (kh) PWM (kh) f (kh). (8) Here, P(kh) is the motor power, (kh) is the rotational speed, f(kh) is the steady-state average flow estimator, and PWM(kh) is the pulse-width modulation signal. The block diagram of the system with an ARX model is illustrated in Fig. 4. All input signals were averaged during the diastolic period shown in Fig. 5. ARX P(kh) f (kh) g ( P(kh), (kh)) (kh) yest (kh) Model PWM (kh) Fig. 4. Input/ output block diagram for the dynamical system model used to estimate the mean inlet pressure (yest(kh)) using as inputs the non-invasive measurements of mean rotational speed, mean power, and mean PWM signal during diastolic period. 120 The static equation for the flow estimator is based on the work of Malagutti et al. [18] and Ayre et al. [19] and is of the following form: Qss a1 a 2 P a3 P 2 a 4 P 3 a5 a 6 2 , (1) where P = VI is the product of supply voltage (V) and motor current (I), and a1-a6 are functions of viscosity levels [18]. We introduced a variable f(kh) as follows [1]: f (kh) g ( P(kh), (kh)), (2) where g ( P(kh), (kh)) a1 a 2 P(kh) a3 P 2 (kh) a 4 P 3 (kh) a5( kh) a6 2 (kh). (3) Here, h > 0 is the sampling interval equals to 0.02s, P(kh) = V(kh)I(kh) is the product of supply voltage (V(kh)) and motor current (I(kh)), and (kh) is the pump rotational speed. Now, we introduce a multi-input dynamical ARX model of the form: n 4 m y est ( kh) bi y est ([k i ]h ) cij u j ([k i 1]h ) (4) i 1 j 1 i 1 e1 ( kh), where yest(kh) is the output of the system which represents the estimated mean inlet pressure during the diastolic phase of the cardiac cycle, n is the model output order, m is the model inputs order, bi and cij are the output and input parameters of the model respectively, e1(kh) represents the model error, and uj(kh) are four exogenous inputs defined as follows: Inlet Pressure (mmHg) Fig. 3. Schematic diagram showing the LVAD connected to the native heart. The inlet cannula was inserted into the left ventricle and the outlet cannula was connected to the aorta. Arrows show the flow direction. 100 80 60 T Dias T Dias T Dias T Dias T Dias 40 20 0 2.73 2.74 2.75 Time (Samples) 2.76 2.77 4 x 10 Fig. 5. Example of extracted diastolic period (TDias) where “x” and “o” represent the starting and the end of TDias respectively. Average values for all signals were calculated during the diastolic period. C. System identification and data analysis Inlet pressure (Pin), motor power (P), rotational speed (), PWM, and f signals obtained from each animal data were averaged during the diastolic phase (T Dias) of the heart. Average values of all signals were stored for further analysis and system identification. Data were divided into two sets: one set was used for system identification while another set was used to validate the model. The first set of data consisted of one animal experiment corresponding to the three blood volume levels changes: low, medium, and high, while the other set contained data from the other three dog experiments. The transient response of the pump inlet pressure was identified and validated using data obtained during changes in the pump target speed. In the system identification process, an off-line least squares method [20] was used to estimate the parameter coefficients of the mean inlet pressure estimation model. Values of parameter coefficients of the inlet pressure estimation model described in (4) were chosen to minimize the error between estimated (yest(k)) and measured (ymeas(k)) mean inlet pressure. The output model order (n) together with the model inputs orders (m) were chosen across a range of 1 to 10. The delay 3576 value was determined by estimating the impulse response of the system using cross-correlation analysis between the inputs and output signals. The mean absolute error (e) and correlation coefficient (R) between yest(kh) and ymeas(kh) were used to evaluate the accuracy of the estimation models. Values of e and R were evaluated as follows: 1 N e ( ymeas (kh) yest (kh)) 2 , (9) N i 1 N R ( y i 1 meas ( kh) y meas )( y est ( kh) y est ) N N i 1 i 1 ( ( y meas ( kh) y meas ) 2 ( y est ( kh) y est ) 2 )1 / 2 Here, N is the length of data. . (10) y est and ymeas are the mean values of the estimated and measured signal respectively. To reduce the contributions of external sources in the identification process of the system, all sets of data were explicitly pre-treated to remove trends and offsets by direct subtraction. All simulations and algorithms were performed in MATLAB R2007b® (The Mathworks, Inc., Natick, MA, USA). D. Control algorithm In order to design a control algorithm for mean inlet pressure in an IRBP, two new ARX models were developed in the present study. The first one describes the relationship between the control input signal, i.e. the PWM signal u(.)), the steady-state pump flow (f(.)), pump rotational speed ((.)), mean inlet pressure (Pin(.)), and motor power (P(.)) during the diastolic period. The resulting system model is described by the following difference equation: chosen so that the mean absolute error (e), obtained from (9), between the estimated and measured values were minimized with high correlation coefficient (R). In the control algorithm represented in this paper, models described in equation (11) and (12) were used to estimate the mean pump power (P(kh)) and mean pump rotational speed (kh) respectively. The high variability in the preload and afterload encountered by patients during their daily activities place a restriction on the control design problem for an IRBP as it is required that the controller should react fast to these changes in order to avoid undesired pumping states such as ventricular collapse. In order to track the desired input signal within minimum possible sampling periods and minimum steady-state error, we derived our control input, u(.) based on (4), as follows: u( kh) 1 (l2 P ( kh) l3 P ([k 1]h ) l4 P ([k 2]h ) l1 f ( kh) l5 ( kh) l6 ([k 1]h ) l7 ([k 2]h ) l8 f ( kh) l9 f ([k 1]h ) l10 f ([k 2]h ) l11u ([k 1]h ) f ([k 1]h ) l12u([k 2]h ) f ([k 2]h ) r ([k 2]h )), (13) Where r(kh) is the desired input signal, l1- l12 are constants with values of 0.000665, 0.926, 0.4683, 0.462, 0.1517, 0.3625, 0.2097, 0.1096, 0.5384, 0.4774, 0.01216, and 0.00987 respectively. In all simulations, we added uniformly distributed noise to model error terms, e1- e3, in equations (4), (11), and (12) respectively to represent model uncertainty. III. RESULTS P( kh) d1u([k 1]h ) d 2 u([k 2]h ) d 3 ([k 1]h ) d 4 ([k 2]h ) d 5 f ([k 1]h ) d 6 f ([k 2]h ) d 7 Pin ([k 1]h ) d 8 Pin ([k 2]h ) d 9 P([k 1]h ) d10P([k 2]h ) d11P([k 3]h ) e2 ( kh).(11) Here, d1, d2, d3, d4, d5, d6, d7, d8, d9, d10, and d11 are constants with values of 0.107, 0.0925, 0.0006232, 0.00044, 0.0365, 0.02183, 0.00306, 0.00202, 1.369, 0.6751, and 0.283 respectively and e2(kh) is the model error. Also, the second ARX model relates u(.), f(.), (.), Pin(.), and P(.). The resulting model is as follows: The performance of the model for mean inlet pressure estimation given in equation (4) was evaluated based on the mean absolute error e, equation (9), and correlation coefficient R, equation (10), for different combinations of model inputs orders m and model output order n. System model orders of n = 3, m = 3, and delay value = 2 gave the best results, i.e. with the minimal e and highest R value between the estimated and measured inlet pressure. The resulting system model is described by the following difference equation: 4 m n yest ( kh) cij u j ([k i 1]h ) bi yest ([k i ]h ) ( kh) g1u([k 3]h ) g 2 u([k 4]h ) g 3 P([k 3]h ) j 1 i 1 g 4 P([k 4]h ) g 5 f ([k 3]h ) g 6 f ([k 4]h ) g 7 Pin ([k 3]h ) g8 Pin ([k 4]h ) g 9 ([k 3]h ) g10 ([k 4]h ) e3 ( kh), (12) where g1 - g10 are constants with values of 2.865, 3.026, 20.74, 26.66, 12.89, 8.616, 1.182, 1.21, 1.593, and 0.7055 respectively, and e3(kh) is the model error. Parameter coefficients, orders, and time delays for models (11) and (12) were obtained using the system identification procedure described in subsection C. Orders and parameters were i 1 e1 (kh).(14) Here, b1= -1.119, b2= 0.5803, b3= -0.4472, c11= -0.926, c12= -0.51517, c13= 0.1096, c14= -0.000665, c21= 0.4683, c22= 0.3625, c23= 0.5384, c24= -0.01216, c31= 0.462, c32= -0.2097, c33= -0.4774, c34= 0.00987, and uj represents the four exogenous inputs described previously in equations (5) – (8). The dashed line in Fig. 6 shows the estimated and measured mean inlet pressures. Note that the model was able to accurately track the changes in mean inlet pressure with 3577 25 12 Measured P in 20 Inlet Pressure (mmHg) of inlet pressure. The resulting output is plotted against the desired reference input and shown in Fig. 10. It was shown that the simulated inlet pressure accurately tracked the reference input signal within an error of + 0.92 mmHg. Estimated pump power (Watt) stable transient response at each volume change. Linear regression analysis between measured and estimated mean inlet pressure obtained from three dog experiments is illustrated in Fig. 7. The analysis resulted in a high R2 = 0.9503 between the estimated and measured with small e = 2.31 mmHg. Also, the mean slope of the linear regression line was very close to unity (1.174) with offset value of 0.9605. Linear regression analysis between estimated and measured pump power resulted in a high R2 = 0.969 with small e = 0.451 W. The mean slope of the linear regression line is also close to unity (0.9439) (Fig. 8). P 10 8 est 2 = 0.9439 * P meas 6 4 2 0 0 Estimated P 2 4 6 Measured pump power (Watt) in 15 +0.658 R = 0.969 e = 0.451 8 10 Fig. 8. Linear regression plot between estimated versus measured pump power obtained from animal data (N = 3). 10 Estimated rotational speed (rpm) 5 0 -5 -10 0 500 1000 1500 2000 2500 Time (s) 3000 3500 4000 Fig. 6. Estimated mean inlet pressure compared with the measured pressure obtained in one animal experiment where target rotational speed was varied from = 1250 to 3000 rpm in each period of blood volume changes. In this dog, blood volume was changed from low to medium at t = 970s, then to high at ts. The solid line shows the measured extracted mean inlet pressure, while the dashed line shows the estimated mean inlet pressure. Estimated Inlet Pressure (mmHg) 30 Pin est = 1.174 *Pin meas+0.9605 25 R2 = 0.9503 e = 2.31 mmHg 20 15 10 5 0 -5 -5 0 5 10 15 Measured Inlet Pressure (mmHg) 20 25 Fig. 7. Linear regression plot between estimated versus measured inlet pressure obtained from animal data (N = 3). A square wave signal was used as the desired input signal, r(kh), to the control algorithm to mimic the variability nature w est 2 = 0.9914 * w meas + 26.39 3000 R = 0.975 e = 14.79 rpm 2500 2000 1500 1500 2000 2500 3000 Measured rotational speed (rpm) 3500 Fig. 9. Linear regression plot between estimated versus measured pump rotational speed obtained from animal data (N = 3). 20 r P in 10 0 in P / r (mmHg) The proposed pump rotational speed estimation model, represented by equation (12), was accurately able to track target speed changes. Furthermore, linear regression analysis between estimated and measured pump rotational speeds resulted in a high R2 = 0.975 and small e = 14.79 rpm. The slope of the regression line was very close to unity (0.9914) with an offset value of 26.39 rpm (Fig. 9). In this study, the models developed for estimation of mean inlet pressure (shown in equations (14)), mean pump power (11), and mean pump rotational speed (12) together with control signal (11) were used to design a control algorithm to control mean inlet pressure. In practical situations, pump speed and power are measured, not estimated. In this study, we used estimated pump values in order to complete the controller design. 3500 -10 -20 0 0.5 1 1.5 2 2.5 Time (s) 3 3.5 4 4.5 Fig. 10. Reference input (r) versus inlet pressure (Pin). IV. DISCUSSION The problem of non-invasive estimation and control of inlet pressure in an IRBP has not been frequently studied. This may be due to the highly variable nature of the inlet pressure, especially during abnormal pumping states of the pump such as ventricular collapse. In the present study, a dynamical model for mean inlet pressure estimation during the diastolic period was successfully designed and verified. Also, the model was used to design a controller for the control of mean inlet pressure during diastolic period. The inlet pressure estimation model used as inputs the noninvasive measurements of pump motor power (P), rotational speed (), steady-state flow (f), and the pulse-width modulation signal. One limitation of the current study is that in a 3578 VentrAssist® LVAD, the power coefficient values used in the static flow estimator equation as well as our estimation models were highly affected by the HCT values. This required routine measurement of the HCT during the experiment and adjustment of the model as described in [18]. Previously, Bullister et al. [17], developed a control algorithm for pump speed using the pump inlet and output pressures measured using pressure sensors as inputs. In their study, while they were able to build a stable pressure-based controller using pressure sensors on a standard mock-loop, they required the use of these invasive additional sensors. Giridharan et. al. [21] designed a control system which was able to maintain the average pressure difference between the left ventricle and the aorta at a desired reference differential pressure. Although they were able to show that maintaining a reference differential pressure between the left ventricle and aorta leads to adequate blood supply for different pathologic and physical activity situations, their proposed approach required the implantation of two pressure sensors. In comparison with the aforementioned studies, the present paper proposed an inlet pressure estimation and controller using non-invasive measurements of pump power and rotational speed. [5] [6] [7] [8] [9] [10] [11] [12] [13] V. CONCLUSIONS A stable and novel dynamical model was proposed for mean inlet pressure estimation during diastolic period in an IRBP. In the proposed model, non-invasive measurements of motor power and impeller rotational speed were used as inputs. Furthermore, in this paper, we developed a noninvasive controller that controls the mean inlet pressure during the diastolic period. The performance of the controller was tested in the presence of model uncertainty. Simulation results showed that the controller was able to track the reference input with minimal error and minimum sampling periods. The model will help in the design of robust control algorithm that control the operation of IRBP, detect and avoid undesired abnormal pumping states. [14] [15] [16] [17] [18] ACKNOWLEDGMENT This work was supported in part by the Australian Research Council. [19] REFERENCES [20] [1] [2] [3] [4] A. H. AlOmari, A. V. Savkin, D. M. Karantonis, E. Lim, and N. H. Lovell, “Non-invasive estimation of pulsatile flow and differential pressure in an implantable rotary blood pump for heart failure patients,” Physiological Measurement, vol. 30, pp. 371- 386, 2009. E. Lim, A. H. AlOmari, A. V. Savkin, and N. H. Lovell, “Noninvasive deadbeat control of an implantable rotary blood pump: A simulation study,” in Proc. 31st Annu. Int. Conf. of the IEEE Engineering in Medicine and Biology Society, Minneapolis, pp. 2855- 2858, 2009. E. Lim, S. Dokos, S. L. Cloherty, R. F. Salamonsen, D. G. Mason, J A. Reizes, and N. H. Lovell, “Parameter-optimized model of cardiovascular-rotary blood pump interactions," IEEE Transactions on Biomedical Engineering, vol. 57, no. 2, pp. 254- 266, 2010. G. A. Giridharan and M. Skliar, “Nonlinear controller for ventricular assist devices” Artificial Organs, vol. 26, pp. 980- 984, 2002. [21] 3579 Y. Wu, P. Allaire, G. Tao, H. Wood, D. Olsen, and C. Tribble, ”An advanced physiological controller design for a left ventricular assist device to prevent left ventricular collapse, ” Artificial Organs, vol. 27, pp. 926- 930, 2003. A. Arndt, P. Nüsser, K. Graichen, J. Müller, and B. Lampe,” Physiological control of a rotary blood pump with selectable therapeutic options: control of pulsatility gradient,” Artificial Organs, vol. 32, pp. 761- 771, 2008. M. Fu and L. Xu,”Computer simulation of Sensorless fuzzy control of a rotary blood pump to assure normal physiology,” American Society of Artificial Internal Organs, vol. 46, pp. 273- 278, 2000. S. Choi, J. Antaki, R. Boston and D. Thomas, “A Sensorless approach to control of a turbodynamic left ventricular assist system,” IEEE Transactions on Control Systems Technology, vol. 9, pp. 473- 482, 2001. G. Endo, K. Araki, K. Kojima, K. Nakamura, Y. Matsuzaki, and T. Onitsuka, ”The index of motor current amplitude has feasibility in control for continuous flow pumps and evaluation of left ventricular function,” Artificial Organs, vol. 25, pp. 697- 702, 2001. S. Choi, and J. R. Boston, “An investigation of the pump operating characteristics as a novel control index for LVAD control,” International Journal of Control, Automation, and Systems, vol. 3, pp. 100- 108, 2005. S. Choi, J. Boston, and J. Antaki, “Hemodynamic controller for left ventricular assist device based on pulsatility ratio,” Artificial Organs, vol. 31, pp. 114- 125, 2007. M. Vollkorn, H. Schima, L. Huber, R. Benkowski, G. Morello, and G. Wieselthaler, ”Development of a reliable automatic speed control system for rotary blood pumps, ” Journal of Heart Lung Transplant, vol. 24, pp. 1878- 1885, 2005. T. Waters, P. Allaire, G. Tao, M. Adams, G. Bearnson, N. Wei, E. Hilton, M. Baloh, D. Olsen, and P. Khanwilkar,” Motor feedback physiological control for a continuous flow ventricular assist device,” Artificial Organs, vol. 23, pp. 480- 486, 1999. J. Zhou, G. P. Armstrong, A. L. Medvedev, W. A. Smith, L. A. Golding, and J. D. Thomas,” Numeric modeling of the cardiovascular system with the left ventricular assist device,” American Society of Artificial Internal Organs, vol. 45, pp. 83- 89, 1999. G. Giridharan, and M. Skliar, “Physiological control of blood pumps using intrinsic pump parameters: a computer simulation study,” Artificial Organs, vol. 30, pp. 301- 307, 2006. Y. Wu, P. Allaire, G. Tao, and D. Olsen, “Study of pressure estimation for a human circulatory system with a LVAD,” in Proceedings of the American Control Conference, 2006, pp. 713718. E. Bullister, S. Reich, and J. Sluetz, “Physiologic control algorithms for rotary blood pumps using pressure sensor input,” Artificial Organs, vol. 26, pp. 931- 938, 2002. N. Malagutti, D. M. Karantonis, S. L. Cloherty, P. J. Ayre, D. G. Mason, R. F. Salamonsen, and N. H. Lovell, ”Non-invasive average flow estimation for an implantable rotary blood pump: a new algorithm incorporating the role of blood viscosity” Artificial Organs, vol. 31, pp. 45- 52, 2007. P. J. Ayre, N. H. Lovell, and J. C. Woodard,”Non-invasive flow estimation in an implantable rotary blood pump: a study considering non-pulsatile and pulsatile flow,” Physiological Measurement, vol. 24, pp. 179- 198, 2003. L. Ljung, “System identification: theory for the user,” 2 nd ed., Englewood Cliffs, NJ: Prentice-Hall, 1999. G. A. Giridharan, M. Skliar, D.B. Olsen, and G. M, Pantalos, “Modeling and control of a brushless DC axial flow ventricular assist device,” American Society of Artificial Internal Organs, vol. 48, pp. 272- 289, 2002.