Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
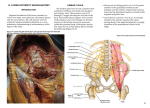
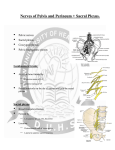
Ischiorectal fossa Lumbosacral plexus Arteries Nerves 11/07/2016 BAAB@2016 The ischiorectal fossa (also called ischioanal fossa) is the fat-filled space located lateral to the anal canal and inferior to the pelvic diaphragm. It is somewhat prismatic or wage shaped, with its base directed to the surface of the perineum, and its apex at the line of meeting of the obturator and the anal fasciae. Fig: Pelvic organs and spacial arrangement Boundaries ANTERIOR: ◦ fascia of Colles covering the Transversus perinei superficialis ◦ inferior fascia of the urogenital diaphragm POSTERIOR: ◦ gluteus maximus ◦ sacrotuberous ligament LATERAL: ◦ tuberosity of the ischium ◦ obturator internus muscle ◦ obturator fascia MEDIAL: ◦ levator ani ◦ sphincter ani externus muscle ◦ anal fascia SUPERIOR: ◦ levator ani INFERIOR: ◦ skin Contents The contents include: - Ischiorectal pad of fat with numerous fibrous bands extend from side to side allows distension of the anal canal during defecation - Inferior rectal nerve and vessels. - Posterior scrotal / labial nerve and vessels. - Pudendal canal (Alcock's canal) on the lateral wall and its contents which are: internal pudendal artery internal pudendal vein pudendal nerve Perineal branch of fourth sacral nerve. Perforating cutaneous branch of S2 , S3 nerve . Applied Anatomy 1. The two Ischiorectal fossae allow distension of rectum and anal canal during passage of faeces. 2. [a] Both the Perianal and Ischiorectal spaces are common site of abscesses. This is due to poor blood supply and coarse lobulated fat which predispose it for infection. [b] The Ischiorectal abscess may be the result of spread of infection from the nearby area - skin, lumen of bowel or perirectal tissue above the levator ani or through the blood or lymphatic. [c]They can be excised fearlessly because of the poor vascularity of the fossa. [d]Abscesses in this region are - (i) Perianal abscess (ii) Ischiorectal abscess (iii) Supra levator abscess (iv) Sub mucous abscess. [e]When making incision for drainage of abscesses care must be taken to avoid injury to inferior rectal neuromuscular bundle to prevent paralysis of external sphincter. 3. The Ischiorectal fat acts as a cushion like support of rectum and anal canal. Loss of this fat in debilitating diseases like diarrhea in children may results in prolapse of the rectum. 4. The occasional gap between the origin of levator ani and the Obturator fascia is known as the hiatus of Schwalbe. Rarely pelvic organs may herniate through this gap resulting in an Ischiorectal hernia. 5. Tension in gluteus maximus as during standing compresses fat of the fossa around anal canal contributing to fecal continence. 6. Fournier's Gangrene - An uncommon but potentially lethal complication of Ischiorectal abscess. This is a type of necrotizing fasciitis usually affecting the perineum. It is commonly occuring in elderly men, but also in women and children, more likely in diabetes, alcoholics, or immune compromised cases. 7. Through the inter Sphincteric longitudinal fibers the inter Sphincteric abscess tracks down and gives rise to Perianal abscess. 8. Pudendal Nerve - (a) Sphincteric Incontinence - Injury to the inferior rectal branch of the pudendal nerve causes Sphincteric incontinence. ( b) Pudendal Block - The pudendal nerve is infiltrated with local anaesthetic solution where it crosses the ischial spine. The ischial spine is palpated through the vagina / rectum and the needle is inserted through the perineum, medial to the ischial tuberosity to anaesthetize the perineum. Further sensory branches of the perineum are derived from the ilio inguinal nerve, the perineal branch of the posterior cutaneous nerve of the thigh and the genital branch of the genito femoral nerve. This means that when complete perineal anesthesia is required an injection of local anaesthetic must be given around the anus. This is plexus of nerves formed from the anterior divisions of the lumbar nerves, sacral nerves, and coccygeal nerve, the first lumbar nerve being frequently joined by a branch from the twelfth thoracic. For descriptive purposes this plexus is usually divided into three parts: ◦ lumbar plexus ◦ sacral plexus ◦ pudendal plexus Fig: Lumbosacral plexus of nerves The lumbar plexus is a web of nerves (a nervous plexus) in the lumbar region of the body which forms part of the larger lumbosacral plexus. It is formed by the divisions of the first four lumbar nerves (L1-L4) and from contributions of the subcostal nerve (T12), which is the last thoracic nerve. Additionally, the ventral rami of the fourth lumbar nerve pass communicating branches, the lumbosacral trunk, to the sacral plexus. ◦ The lumbosacral trunk comprises the whole of the anterior division of the fifth and a part of that of the fourth lumbar nerve; it appears at the medial margin of the psoas major and runs downward over the pelvic brim to join the first sacral nerve. The nerves of the lumbar plexus pass in front of the hip joint and mainly support the anterior part of the thigh. The plexus is formed lateral to the intervertebral foramina and passes through psoas major. Its smaller motor branches are distributed directly to psoas major, while the larger branches leave the muscle at various sites to run obliquely down through the pelvis to leave under the inguinal ligament, with the exception of the obturator nerve which exits the pelvis through the obturator foramen. Fig: This is a lumbar plexus Distribution of the lumbar plexus lumbar plexus gives out the ◦ iliohypogastric giving the lateral cutaneous branch anterior cutaneous branch ◦ ilioinguinal giving the anterior scrotal ♂/labial ♀ ◦ genitofemoral giving the femoral branch genital branch ◦ lateral cutaneous giving the patellar ◦ obturator giving the anterior branch which also gives cutaneous posterior accessory ◦ Femoral giving the anterior cutaneous branches Saphenous giving infrapatellar and medial crural cutaneous The Sacral plexus is a nerve plexus which provides motor and sensory nerves for the posterior thigh, most of the lower leg and foot, and part of the pelvis. It is part of the lumbosacral plexus and emerges from the lumbar vertebrae and sacral vertebrae (L4-S4). A sacral plexopathy is a disorder affecting the nerves of the sacral plexus, usually caused by trauma, nerve compression, vascular disease, or infection. Symptoms may include pain, loss of motor control, and sensory deficits. ◦ Plexopathy is a disorder affecting a network of nerves, blood vessels, or lymph vessels. The region of nerves it affects are at the brachial or lumbosacral plexus. Fig: sacral and pudendal plexuses Distribution of the sacral plexus Sacral plexus gives out the ◦ Sciatic common peroneal lateral sural cutaneous communicating branch deep peroneal lateral terminal branch medial terminal branch dorsal digital superficial peroneal medial dorsal cutaneous intermediate dorsal cutaneous dorsal digital Sacral plexus ◦ Tibial medial sural cutaneous medial calcaneal medial plantar common plantar digital nerves proper plantar digital lateral plantar ◦ Sural deep branch superficial branch common plantar digital proper plantar digital lateral dorsal cutaneous lateral calcaneal ◦ Other Muscular lateral rotator group to quadratus femoris to obturator internus to the piriformis cutaneous: posterior cutaneous of thigh inferior cluneal perineal branches perforating cutaneous Fig: Schematic diagram of the sacral plexus The Pudendal or coccygeal plexus originates from S4, S5, and Cx1 spinal nerves. It is interconnected with the lower part of sacral plexus. The only nerve of the plexus is the anococcygeal nerve, which serves sensory innervation of the skin in the coccygeal region (tail and around the anus) Distribution of the Pudendal plexus ◦ Pudendal Inferior branch Anal branch ◦ Perineal Deep scrotal/labial Posterior scrotal/labial ◦ Dorsal nerve of the penis/clitoris ◦ Anococcygeal cutenous of the lower limb. Vessels, and Nerves of the pelvis. Oxygenated blood begins its course down the chest through the thoracic aorta, then it becomes the abdominal aorta in the abdomen then in the pelvis, the abdominal aorta forks into two branches called common iliac arteries. These travel down each leg, where they branch into internal and external iliac arteries. A pair of internal iliac arteries , superior rectal arteries , ovarian arteries and un paired median sacral artery, supply the pelvic region. Ovarian arteries from abdominal aorta, supply blood to the reproductive organs, such as the ovaries, fallopian tubes, and uterus. Internal iliac arteries through their anterior and posterior branches supply blood to the pelvic viscera, perineum, pelvic wall, and the buttocks superior rectal arteries are direct continuations of the inferior mesenteric arteries supply the mucosa of the rectum and upper half of the anal canal median sacral artery arises at the birfucation of the aorta. It descends over the anterior surface of the sacrum and the coccyx. Veins typically follow the same path as arteries. Similar to the arteries in the pelvis, veins form plexuses within the legs. As blood returns to the heart the tributaries -- the internal and external iliac veins -- the common iliac vein -- the inferior vena cava, the large vessel that runs parallel to the abdominal aorta. Common iliac vein also receives inferior epigastric and the deep circumflex iliac veins. Nerves branch from the spinal cord. There are three types of nerves: ◦ Autonomic nerves: These control involuntary or partially voluntary actions such as heartbeat. ◦ Motor nerves: These signal muscles to move. ◦ Sensory nerves: These relay information from the skin and muscles, such as heat and pain. In the pelvis, the vertebral column ends in the sacrum, (five fused vertebral bones) that form the back of the pelvis. Behind it is the sacral plexus, a collection of nerves that serve the pelvic area, genitals, buttocks, and parts of the legs and feet. The sciatic nerve is the largest nerve, and originates from the sacral plexus. This large nerve fiber begins in the lower back at the vertebral column, runs through the buttocks (beneath the gluteus maximus muscle), and extends down the back of the thigh. There is one sciatic nerve in each leg, and each is about one inch wide in the pelvis.