Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
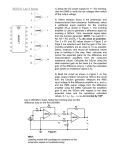
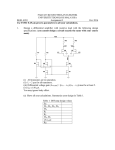
From www.bloodjournal.org by guest on June 11, 2017. For personal use only. RAPID COMMUNICATION Measurement of Basal Levels of Factor VIIa in Hemophilia A and B Patients By Peter Wildgoose, Yale Nemerson, Lisbeth Lyng Hansen, Finn E. Nielsen, Steven Glazer, and Ulla Hedner Previous results, presented in abstract form, indicate that replacement of thromboplastin with a mixture of phospholipid and truncated soluble tissue factor apoprotein results in a coagulation assay that can directly measure plasma factor Vlla levels without interference from zymogen factor VI1 (Atherosclerosis Thromb 11:1544a, 1991 [abstr]). We have exploited the specificity and sensitivity of such a factor Vlla specific coagulation assay to directly assess the in vivo relationship of factor Vlll and factor IX on the production of factor Vlla levels under nonthrombotic and nonstimulatory conditions. Normal individuals (n = 20) were found to possess an average circulating factor Vlla level corresponding to 4.34 f 1.57 ng/mL, or approximately 1% of their total factor VI1 antigen. Severe factor Vlll deficient patients (n = 13) F ACTOR VI1 is a trace vitamin K-dependent glycoprotein that participates in initiation of the extrinsic pathway of blood coagulation. Under normal conditions factor VI1 circulates in blood mainly as a precursor to its activated form, factor VIIa. However, on vascular injury factor VI1 forms a bimolecular complex with its high affinity cell surface cofactor, tissue factor, which is presented on many cell types. Once bound to tissue factor, factor VI1 is rapidly converted to its activated two-chain form, factor VIIa. Precisely which protease is responsible for the conversion of factor VI1 to VIIa under in vivo conditions is unknown. However, it is known that factor IXa,’ factor Xa? factor XIIa?g4 thrombin: and factor VIIa6 are all efficient activators of factor VI1 in the test tube. Once activated, the factor VI1a:tissue factor complex rapidly activates its protein substrates factors IX and X by limited proteolysis, which eventually leads to thrombin formation and a fibrin clot. Despite major advances into the biochemistry and in vitro behavior of the coagulation factors, little is known about the coagulation mechanism as it functions in vivo under basal (ie, in the absence of thrombosis or provocative stimuli) activation levels. The development of immunoassays for the activation peptides of human factor IX,7 human factor X,8 and human prothrombin9 have provided tools for the indirect measurement of coagulation activation. Based on these assay systems it has been suggested that the basal activity of the hemostatic system is primarily caused by factor VI1a:tissue factor function, which is responsible for the continuous generation of factor IXa, factor Xa, and thrombin. To investigate more closely the role of factor VIIa under basal conditions, we have used a factor VIIa specific coagulation assaylOJ1 to measure and directly compare the circulating factor VIIa levels in normal plasma as well as plasma from severe hemophilia A and B patients. In this report we provide direct evidence that basal factor VIIa levels in factor IX deficient patients is greatly reduced in comparison with normal individuals. These results are consistent with the hypothesis that factor IXa is the principal in vivo activator of factor VI1 under basal conditions. Blood, Vol80, No 1 (July 1). 1992: pp 25-28 possesseda slightly lower but statisticallysignificant (P < .01) decrease in their basal factor Vlla levels (2.69 f: 1.52 ng/mL), corresponding to 360% of that observed in normal individuals. On the other hand, severe factor IX deficient patients (n = 7) were found to possess even lower levels of factor Vlla correspondingto 0.33 k 0.15 ng/mL, or less than 10% of that observed in normal individuals. Measurement of total factor VI1 antigen levels shows that the variation in basalfactor Vlla levels stems from differences in the degree of factor VI1 activation as opposed to differences in factor VI1 antigen levels. Our present data are consistent with the hypothesis that factor IXa is the principal in vivo activator of factor VI1 under basal conditions. 0 1992 by The American Society of Hematology. MATERIALS AND METHODS Bovine serum albumin (BSA) (fatty-acid free) was obtained from Sigma (St Louis MO). Bovine brain phospholipids (Thrombofax) were purchased from Ortho Diagnostics (Raritan, NJ). Factor VI1 deficient plasma (< 1% factor VI1 antigen), obtained from a hereditary factor VI1 deficient patient, was generously provided by Dr Walter Kisiel (University of New Mexico, Albuquerque). Recombinant human factor VIIa was purified from BHK cell culture medium as described previously.12 Recombinant soluble tissue factor apoprotein (residues 1through 218) was purified from the culture media of transfected BL-21 (DE3) Escherichia coli cells by a combination of ammonium sulphate precipitation and S-Sepharose and Q-Sepharose ion exchange ~hromatography.’~ Total factor VI1 antigen levelswere determined using a solid-phase double-antibody enzyme-linked immunoassay (ELISA) kit obtained from Novo Nordisk (Bagsvaerd, Denmark).14This assay is a two-site monoclonal antibody assay in which a sandwich is formed between a solid-phase catching antibody, the factor VIIIVIIa sample, and a peroxidase-conjugated anti-factor VI1 detecting antibody. Total factor VIIIVIIa levels are determined by comparison to a standard curve constructed with known amounts of recombinant factor VIIa. Coagulation assays. All plasma factor VIIa levels were measured in a one-stage clotting assay using an ACL300R automated coagulation instrument purchased from Instrumentation Laboratories (Ascoli Piceno, Italy). Test samples were diluted fivefold in 0.1 molIL NaC110.05 molIL Tris-HC1/0.1% BSA pH 7.4 (TBSIBSA) and mixed with an equal volume of hereditary factor VI1 deficient plasma to yield a total volume of 100 pL. Each aliquot was From Novo Nordisk AIS, Biophaimaceuticals Division, Gentofte, Denmark; and the Division of Thrombosis Research, the Deparhent of Medicine, Mount Sinai School of Medicine of the City University of New York, New York Submitted March 16,1992; accepted April 18, 1992. Address reprint requests to Peter wildgoose, PhD, Novo Nordisk AIS, Niek Steensens Vej 1, DK-2820 Gentofte, Denmark. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C.section 1734 solely to indicate this fact. 0 1992 by TheAmerican Society of Hematology. 0006-4971f 9218001-0046$3.00/0 25 From www.bloodjournal.org by guest on June 11, 2017. For personal use only. WILDGOOSE ET AL 26 subsequently incubated for 5 minutes at 37°C with 50 KLof bovine phospholipids (Thrombofax). Coagulation was then initiated by the addition of a 1OO-kL aliquot of 10 nmol/L TF1.218 diluted in 12.5 mmol/L CaC12/0.1 mol/L NaCl/O.O5 mol/L Tris/l% BSA pH 7.4. Coagulation times were subsequently converted to factor VIIa concentration (nanograms per milliliter) by comparison to a standard curve constructed with varying concentrations (0.05 to 50 ng/mL) of purified recombinant factor VIIa diluted in TBS/BSA. Collectwn and processing of blood samples. Venipunctures were performed autraumatically and blood samples drawn into citrated vacutainers. The citrated samples were centrifuged for 15 minutes at 1,200g after which time the plasma was removed with a plastic pipette and stored at -80°C. Normal plasma samples were collected from 10 fasting and 10 nonfasting individuals who had a negative history for bleeding as well as thrombosis and were not taking any medications at the time of sample collection. Patient samples were obtained from 13 severe hemophilia A and seven hemophilia B patients ( < 1% FV1II:C and < 1%FIXC). Patients were excluded from the study if they had received factor concentrates, cryoprecipitate, and/or antifibrinolytics within the previous 48 hours. Informed consent Informed consent was obtained from all patients before drawing of blood samples. RESULTS Results by Macik and Morrissey indicate that replacement of thromboplastin with a mixture of phospholipid and truncated soluble tissue factor apoprotein results in a coagulation assay that can directly measure plasma factor VIIa levels without interference from zymogen factor VII.lo,ll Use of a similar assay system has enabled us to compare the circulating factor VIIa levels of normal individuals to that of individuals afflicted with hemophilia A or B. In preliminary experiments we tested the effect of adding increasing amounts of purified recombinant factor VIIa on the coagulation time of factor VI1 deficient plasma in the presence of phospholipid and a soluble truncated form of recombinant tissue factor apoprotein (residues 1 through 218). By performing a log-log transformation of the coagulation data followed by a linear regression it was possible to construct a standard curve from which one could readily compare coagulation time with factor VIIa content (Fig 1). We found that this assay system could reproducibly measure factor VIIa levels over a wide range covering several orders of magnitude between 100 pg/mL to 1 mg/mL (data not shown). In our initial experiments we measured the circulating factor VIIa levels of normal individuals under fasting and nonfasting conditions (n = 10 per group). The basal factor VIIa levels ranged from 2.21 to 7.85 ng/mL with an average of 4.34 c 1.57 ng/mL (Fig 2). No statistical significancewas observed between the plasma of fasting and nonfasting individuals. To determine the role of factor VI11 or factor IX deficiency on basal factor VIIa levels, we also tested the functional factor VIIa level of 13 severe hemophilia A patients and seven severe hemophilia B patients. The hemophilia A patients possessed a basal factor VIIa level that varied between 1.32 and 6.24 ng/mL with an average of 2.69 5 1.52 ng/mL (Fig 2). Thus, factor VI11 deficiency significantly decreases (P < .01) basal factor VIIa levels to approximately 60% of that observed in normal individuals. 0.1 1 10 Factor VIIa Concentration (ndml) Fig 1. Factor Vlla standard coagulation curve. Varying amounts of recombinant factor Vlla were added to hereditaryfactor VI1 deficient plasma in the presence of phospholipid and soluble tissue factor apoprotein(residues 1 through 218). Coagulation was initiated by the addition of CaCI, and the decrease in coagulation time measured on an automated coagulation apparatus as described in Materials and Methods. Repetitive measurement of basal factor VIIa levels in several hemophilia A patients over a time period of months indicates that basal factor VIIa levels remain essentially constant (data not shown). Measurement of factor VIIa levels in hemophilia B patients shows a drastically lower factor VIIa level in comparison with both normal and hemophilia A patients (P < .01). The seven hemophilia B patients tested in this study were found to possess a circulating factor VIIa level that varied between 0.19 and 0.59 ng/mL with an average of A A E 8 8 U n=7 0 Nmalt Factor Vlll Deficient $- Factor IX Dendent Fig 2. Factor Vlla levels in the plasma of patients with severe factor Vlll deficiency, severe factor IX deficiency, and normalcontrols. The horizontalbar representsthe mean factor Vlla level in each group. From www.bloodjournal.org by guest on June 11, 2017. For personal use only. BASAL FACTOR Vlla LEVELS 0.33 2 0.15 ng/mL. Because the functional factor VIIa level in normal and hemophilic plasma was not influenced by prolonged incubation at room temperature or by such harsh treatment as repetitive freeze thawing, it is highly unlikely that any of the observed differences in factor VIIa levels are caused by ex vivo events. In control experiments all plasma samples were subjected to factor VI1 antigen testing. As expected there was no significant (P > .1) difference in factor VI1 antigen levels between the hemophilia A (445 2 93 ng/mL) and B patients (430 2 89 ng/mL) and that of the normal control group (455 2 72 ng/mL). Control experiments were also conducted to assess the recovery of factor VIIa activity after the addition of trace amounts of rFVIIa (5 to 10 ng/mL) to normal, factor VI11 deficient, and factor IX deficient plasmas. As expected, there was virtually a 100% recovery of factor VIIa activity in each of the plasmas tested. DISCUSSION Measurement of the ratio of factor VI1 coagulant activity to amidolytic activity has previously been used as a crude measure of factor VIIa levels in hemophi1ia~s.l~ Unfortunately this technique is rather imprecise because zymogen factor VI1 undergoes activation during the coagulation assay and thus contributes to the observed coagulant activity.16 However, this problem has recently been circumvented by the observation that a soluble form of tissue factor apoprotein, lacking the cytoplasmic and transmembrane domains, retains cofactor activity toward factor VIIa but is incapable of supporting the activation of zymogen factor VII.” A study by Morrissey et a1 indicates that this soluble form of tissue factor can be used in a modified factor VI1 coagulation assay to specifically measure circulating factor VIIa levels.lOJ In the present study we have developed a similar assay system based on the use of a truncated tissue factor molecule spanning residues 1through 218. We find that this assay system is exquisitely sensitive to trace amounts of factor VIIa and can reproducibly measure recombinant factor VIIa levels between 0.01 ng/mL to 1 mg/mL. In this communication we have exploited the specificity and sensitivity of this factor VIIa specific coagulation assay to directly assess the in vivo levels of factor VIIa under nonthrombotic and nonstimulatory conditions. Previous attempts to assess the role of factor VIIa under basal conditions have centered on measuring the activation peptide that is released from factor IX on activation by either factor VI1a:tissue factor or factor XIa.7 In this regard it has recently been shown that factor VI1 deficient patients have reduced plasma levels of factor IX activation peptide, whereas FXI deficient individuals possess normal levels of factor IX activation ~ e p t i d eIn . ~ related experiments it has been observed that factor VI1 deficient patients also possess lower levels of factor X activation peptide as compared with factor VI11 and factor IX deficient patients who possess essentially normal levels of factor X activation peptide.8 Although these data indicate that the generation of factor IXa and factor Xa under basal conditions is primarily caused by the action of factor VI1a:tissue factor, 27 nothing is known about the role that these coagulation factors play on the activation of factor VI1 under basal conditions. To investigate this question we initially measured the basal factor VIIa levels of normal individuals under fasting and nonfasting conditions. We found that normal individuals, regardless of fasting condition, possessed an average functional factor VIIa level corresponding to 4.3 ng/mL or approximately 1%of their total factor VI1 antigen (assuming an average factor VI1 antigen level of 400 ng/mLls). To assess the in vivo role of factor VI11 and factor IX on basal factor VIIa levels we also measured the factor VIIa levels of severe ( < 1%activity) hemophilia A and B patients. Factor VI11 deficiency was found to have a small but statistically significant effect on circulating factor VIIa levels, with patients on the average possessing a functional factor VIIa level ~ 6 0 % of that observed in normals. Factor IX deficiency, on the other hand, was found to have a far greater effect with factor IX deficient patients on the average possessing a basal factor VIIa level corresponding to 10% of that observed in normal individuals. Although previous in vitro studies indicate that factor Xa is a far more efficient activator of factor VI1 than factor IXa,*9J0our present data are consistent with the notion that factor IXa is responsible for basal activation of factor VI1 under in vivo conditions. Of course, it may be argued that the decrease in basal factor VIIa levels that we have observed in the hemophilia B patients is caused by a concomitant decrease in the functional levels of other serine proteases capable of activating factor VII, such as thrombin and factor Xa. However, this explanation is quite unlikely in view of previous observations that factor IX deficient and factor VI11 deficient individuals possess normal levels of factor X activation peptide and prothrombin fragmentl+z. Precisely what role factor VI11 plays in the activation of factor VI1 is less certain. However, one can readily envision that the reduced factor VIIa levels observed in the factor VI11 deficient patients results from a concomitant decrease in basal factor IXa levels. Whether this hypothesis holds true or not will require measurement of basal factor IXa levels in factor VI11 deficient patients. In conclusion, we have developed a simple and highly specific coagulation assay that can reproducibly measure functional levels of factor VIIa in plasma. Using this assay system we have been able to assess the in vivo role of factor VI11 and factor IX on the production of circulating factor VIIa levels under nonthrombotic and nonstimulatory conditions. Our results are consistent with the hypothesis that factor IXa is the principal in vivo activator of factor VI1 under basal conditions. ACKNOWLEDGMENT The authors thank Dr Lilian Tengbom, Sahlgren’s Hospital, Gothenburg, Sweden, and Dr Sam Schulman of Karolinska Sjukhuset, Stockholm, Sweden, for providing us with samples of factor IX deficient plasma. We also thank Dr Walter Kisiel, University of New Mexico, Albuquerque, for providing us with the hereditaly factor VI1 deficient plasma and Carsten Christofferson for excellent technical assistance. From www.bloodjournal.org by guest on June 11, 2017. For personal use only. WILDGOOSE ET AL 28 REFERENCES 1. Seligsohn U, Osterud B, Brown SF, Griffin JH, Rapaport SI: Activation of human factor VI1 in plasma and purified systems. J Clin Invest 641056,1979 2. Bajaj SP, Rapaport SI, Brown SF: Isolation and characterization of human factor VI1 by factor Xa. J Biol Chem 256:253,1981 3. Kisiel W, Fujikawa K, Davie E W Activation of bovine factor VI1 (proconvertin) by factor XIIa (activated Hageman factor). Biochemistry 16:4189,1977 4. Radcliffe R, Bagdasarian A, Colman R, Nemerson Y Activation of bovine factor VI1 by Hageman factor fragments. Blood 50:611,1977 5. Radcliffe R, Nemerson Y: Activation and control of factor VI1 by activated factor s X and thrombin. J Biol Chem 250:388, 1975 6. Nakagaki T, Foster DC, Berkner KL, Kisiel W: Initiation of the extrinsic pathway of blood coagulation: Evidence for the tissue factor dependent autoactivation of human blood coagulation factor VII. Biochemistry3010819,1991 7. Bauer KA, Kass BL, ten Cate H, Hawiger JJ, Rosenberg RD: Factor IX is activated in vivo by the tissue factor mechanism.Blood 76731,1990 8. Bauer KA, Kass BL, ten Cate H, Bednarek MA, Hawiger JJ, Rosenberg RD: Detection of factor X activation in humans. Blood 74:2007,1989 9. Teitel JM, Bauer KA, Lau HK, Rosenberg RD: Studies of the prothrombin activation pathway utilizing radioimmunoassay for the F Z / F ~fragment +~ and the thrombin-antithrombin complex. Blood 59:1086,1982 10. Macik BG, Morrissey JH: Determination of activated factor VI1 (FVIIa) levels in plasma using a clotting assay specific for FVIIa. Blood 78:61a, 1991 (abstr) 11. Morrissey JH, Macik BG: Novel clotting assay that factor VIIa in plasma using a tissue factor mutant that does not support activation of factor VII. Atherosclerosis Thromb 11:1544a, 1991 (abstr) 12. Thim L, Bjoem S, Christensen M, Nicolaisen EM, LundHansen T, Pedersen AH, Hedner U Amino acid sequence and posttranslational modifications of human factor VIIa from plasma and transfected baby hamster kidney cells. Biochemistry 701947, 1988 13. Waxman E, Ross JBA, Laue TM, Guha A, Thiruvikraman SV, Lin TC, Konigsberg WH,Nemerson Y Tissue factor and its extracellular soluble domain: The relationshipbetween intermolecular association with factor VIIa and enzymatic activity of the complex. Biochemistry (in press) 14. Lund-Hansen T, Olsen AA, Selmer J: A double monoclonal ELISA for human coagulation factor VII. Thromb Haemost 6255, 1989 (abstr) 15. Miller BC, Hultin MB, Jesty J: Altered factor VI1 activity in hemophilia. Blood 65:845,1985 16. Wildgoose P, Berkner K, Kisiel W: Synthesis, purification and characterization of an Arg152-Glu152site directed mutant of recombinant human blood clotting factor VII. Biochemistry 29: 3413,1990 17. Morrissey JH: Alterations to tissue factor that abolish activation of factor VII, but maintain cofactor activity toward factor VIIa. Blood 781096,1991 (abstr) 18. Fair DS: Quantitation of factor VI1 in the plasma of normal and warfarin-treated individuals by radioimmunoassay. Blood 62784,1983 19. Masys DR, Bajaj SP, Rapaport SI: Activation of human factor VI1 by activated factors IX and X. Blood 6:1143,1982 20. Wildgoose P, Kisiel W Activation of human factor VI1 by factors IXa and Xa human bladder carcinoma. Blood 73:1888,1989 From www.bloodjournal.org by guest on June 11, 2017. For personal use only. 1992 80: 25-28 Measurement of basal levels of factor VIIa in hemophilia A and B patients [see comments] P Wildgoose, Y Nemerson, LL Hansen, FE Nielsen, S Glazer and U Hedner Updated information and services can be found at: http://www.bloodjournal.org/content/80/1/25.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.