Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
77 Fungal Diseases
Jenny O Sobera
Boni E Elewski
Key features
Cutaneous fungal infections are broadly divided into those that are
limited to the stratum corneum, hair and nails, and those that involve
the dermis and subcutaneous tissues
Superficial fungal infections of the skin are due primarily to
dermatophytes and Candida spp.
'Subcutaneous' mycoses are often the result of implantation, while
systemic or 'deep' mycoses of the skin usually represent
hematogenous spread or extension from underlying structures
In the immunocompromised host, opportunistic fungi, e.g. Aspergillus
and Mucor, can lead to both cutaneous and systemic infections
This chapter reviews common cutaneous fungal infections, and they are subdivided into three
major groups: (1) 'superficial'; (2) 'subcutaneous'; and (3) 'deep' or systemic (see Table 77.1).
SUPERFICIAL MYCOSES
Introduction
The superficial mycoses are due to fungi that only invade fully keratinized tissues, i.e. stratum
corneum, hair and nails. They can be further subdivided into those that induce minimal, if any,
inflammatory response, e.g. pityriasis (tinea) versicolor, and those that do lead to cutaneous
inflammation, e.g. dermatophytoses (Table 77.2). The former are discussed first.
Non-inflammatory superficial mycoses
Synonyms
Tinea nigra: tinea nigra palmaris et plantaris, superficial
phaeohyphomycosis
Piedra: molestia de Beigel, trichomycosis nodularis
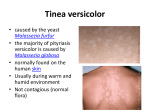
Pityriasis (tinea) versicolor: tinea versicolor, dermatomycosis
furfuracea, tinea flava
Table 77-1. Organization of cutaneous mycoses.
Superficial
Subcutaneous
ORGANIZATION OF CUTANEOUS MYCOSES
Invade stratum corneum, hair and nails
Involve dermis or subcutaneous tissue
Often due to implantation
Systemic
Dermal or subcutaneous involvement
Deep (true
pathogens)
Usually reflects hematogenous spread or extension from
underlying structures
Opportunistic
Primary or secondary skin lesions in immunocompromised hosts
Table 77-2. Superficial mycoses of the skin.
SUPERFICIAL MYCOSES OF THE SKIN
Cutaneous disorder
Pathogen(s)
Minimal, if any,
inflammation
Pityriasis (tinea) versicolor
Tinea nigra
Black piedra
White piedra
Malassezia furfur
(Pityrosporum ovale)
Exophiala werneckii
Piedraia hortae
Trichosporon beigelii
Inflammatory
response common
Tinea capitis, barbae, faciei,
corporis, cruris, manuum, pedis
Cutaneous candidiasis
Trichophyton, Microsporum,
Epidermophyton spp.
Candida albicans
History
In 1846, Eichstedt first noted the disease known today as pityriasis (tinea) versicolor. Over the
ensuing 150 years, Malassezia furfur, came to be recognized as the causative organism.
Recently, however, studies have pointed to M. globosa as the causative agent1. In 1865, Beigel
first described piedra after isolating a fungus from a wig. While the fungus he isolated was likely a
contaminant, his clinical description is still valid. Tinea nigra was first described several decades
later (1890s) by Cerqueira, who named it 'keratomycosis nigricans palmaris'2.
Epidemiology
Tinea nigra and piedra typically occur in tropical climates such as Central and South America,
Africa, Asia and, occasionally, in the southeastern US. While any race, age or gender may be
infected, the typical patient is a young adult. Additionally, Trichosporon beigelii, the cause of white
piedra, is also recognized as an opportunistic pathogen.
The geographic distribution of Malassezia spp. is worldwide. In fact, it is part of the normal flora of
human skin (predominantly M. sympodialis). Although pityriasis (tinea) versicolor occurs most
frequently in tropical climates with high ambient temperatures and high humidity, it is also a
common disorder in temperate climates. No racial or gender difference has been established.
The typical patient is a young adult, but people of any age may develop the disease. Interestingly,
Malassezia has an oil requirement for growth, accounting for the increased incidence in
adolescents and preference for sebum-rich areas of the skin. Malassezia has been implicated in
many other skin diseases, including seborrheic dermatitis and atopic dermatitis, but this remains
controversial. Neonatal cephalic pustulosis (neonatal acne) is associated with Malassezia spp. in
newborn babies, particularly M. sympodialis, according to a recent study3.
Pathogenesis
page 1171
page 1172
Exophiala werneckii and Piedraia hortae are both environmental pathogens. E. werneckii (tinea
nigra) can be found in soil and sewage and even in shower stalls under humid conditions. The
source of exposure to P. hortae (black piedra) is thought to be the soil. There is no known
transmission of these organisms from human to human. T. beigelii (white piedra) is also acquired
from the environment; however, it may occasionally be part of the normal flora of the skin and
mucous membranes4, particularly the groin and axillary skin.
M. furfur (and other species) normally lives on human skin in amounts so minute as to be
undetectable on KOH examination of stratum corneum 5. Pityriasis (tinea) versicolor occurs when
the round yeast form transforms to the mycelial form. In tropical climates, this change is a result
of high temperatures and high humidity. In temperate climates, various factors have been
implicated, including oily skin, excessive sweating, immunodeficiency, poor nutrition, pregnancy
and corticosteroid use. Because this yeast is lipophilic, use of bath oils and skin lubricants may
increase the risk of disease. Risk factors for pityrosporum folliculitis include chronic antibiotic use,
immunosuppression and local occlusion.
Clinical features
Piedra Piedra is a superficial infection of the hair shaft. 'Piedra' actually translates as 'stone', and
fungal elements adhere to one another to form nodules, or 'stones', along the hair shaft. There
are two major forms - black piedra and white piedra - and they are distinguished by clinical
appearance plus microscopic examination (Table 77.3). Patients with black piedra typically
present with asymptomatic brown to black nodules along the hair shaft. Infection usually
commences under the cuticle of the hair shaft and extends outward. Hair breakage may occur as
a result of shaft rupture at the site of the nodules. As the nodules enlarge they can even envelope
the hair shaft (Fig. 77.1).
In white piedra, the infection also begins beneath the cuticle and grows through the hair shaft,
causing weakening and breaking of the hair. The soft, less adherent nodules of white piedra are
generally white but may also be red, green or light brown in color. The incidence of white piedra
in the pubic region has increased since the start of the HIV epidemic. In immunosuppressed
patients, T. beigelii can cause trichosporosis, a serious systemic infection with fungemia, fever,
pulmonary infiltrates, skin lesions (papulovesicular and purpuric, often with central necrosis) and
renal disease4.
Add to lightbox
Figure 77.1 Causes of nodules on hair shafts.
Table 77-3. Comparison of black and white piedra6.
COMPARISON OF BLACK AND WHITE PIEDRA4
White piedra
Black piedra
Nodule color
White (may be red, green or
light brown)
Brown to black
Nodule firmness
Soft
Hard
Nodule adherence
to the hair shaft
Loose
Firm
Typical location
Face and axillae (occasionally in Scalp and face (occasionally in
pubic region)
pubic region)
Climate
Tropical
Temperate
Causative
organism
Trichosporon beigelii
Piedraia hortae
KOH
Non-dematiaceous hyphae with
blastoconidia and arthroconidia
Dematiaceous hyphae with asci
and ascospores*
Culture
Moist, creme-colored, yeast-like Slow-growing, dark brown to
Treatment
colonies
black colonies
Clip affected hairs, wash
affected hairs with antifungal
shampoo
Clip affected hairs, wash
affected hairs with antifungal
shampoo
* Sexual reproduction.
Tinea nigra After a 10- to 15-day incubation period, tinea nigra most commonly presents as a
single, sharply marginated, brown to gray to green macule or patch that can be velvety or have
mild scale. There are usually no associated symptoms (i.e. pruritus), and no predispositions have
been identified. While most frequently seen on the palms, tinea nigra can also appear on the
soles, neck and trunk. Although palmoplantar lesions are said to resemble acquired acral
melanocytic nevi, the former are usually larger, lighter in color and lack the linear striations of the
latter. Tinea nigra can also have darker pigmentation of the advancing border as compared to the
center. While the disease tends to be chronic, recurrence after effective treatment is infrequent
except in the case of re-exposure.
Pityriasis (tinea) versicolor Patients usually present with multiple oval to round patches or thin
plaques with mild scale. Demonstration of this associated scale may require scratching of its
surface. Centrally, within the areas of involvement, the lesions are often confluent and they may
be quite extensive. Seborrheic areas, in particular the upper trunk and shoulders, are the favored
sites of involvement. Less frequently, lesions are seen on the face (more so in children), scalp,
antecubital fossae and groin. When pityriasis (tinea) versicolor involves flexural areas, it is
sometimes referred to as 'inverse' pityriasis (tinea) versicolor.
page 1172
page 1173
Add to lightbox
Figure 77.2 Pityriasis (tinea) versicolor, hyperpigmented variant. Courtesy of Kalman
Watsky, M.D.
The most common colors are tan (hypopigmentation; see Chapter 66) and brown
(hyperpigmentation; Fig. 77.2); occasionally there is associated inflammation with a pink color.
Decreased pigmentation may be secondary to the inhibitory effects of dicarboxylic acids on
melanocytes (the latter result from metabolism of surface lipids by the yeast) or decreased
tanning, due to the ability of the fungus to filter sunlight. In general, pityriasis (tinea) versicolor is
asymptomatic and the major concern is its appearance.
Pityrosporum folliculitis This condition is most commonly seen in young women and is
characterized by pruritic follicular papules and pustules on the trunk, arms, neck and,
occasionally, the face. It is due to excessive growth of P. orbiculare (a culturally identical variant
of M. furfur) within the hair follicle with resulting inflammation (from yeast products and free fatty
acids produced from fungal lipase). Only yeast forms are observed, i.e. no hyphal forms as in
pityriasis (tinea) versicolor. Several Malassezia species have also been implicated in neonatal
cephalic pustulosis ('neonatal acne'; Chapter 36).
Pathology and fungal culture
For both black and white piedra, cut hair shafts are placed in KOH and a 'crush preparation' is
examined microscopically. In a black piedra nodule, dematiaceous hyphae are seen around an
organized cluster of asci, each of which contains eight ascospores. The ascospores represent the
sexual phase of P. hortae. P. hortae grows very slowly when cultured and yields a green to black
colony with velvety texture (asexual phase)7.
KOH preparation of a crushed white piedra nodule reveals nondematiaceous hyphae,
blastoconidia and arthroconidia, representing the asexual state. When cultured, T. beigelii grows
rapidly forming moist, cream-colored, yeast-like colonies that some have likened to butter cream
frosting. On Mycosel® agar, the organism will be inhibited by the presence of cycloheximide. T.
beigelii is often isolated from skin and nail specimens, and the significance of this must be
correlated with clinical findings.
Add to lightbox
Add to lightbox
Figure 77.3 Potassium hydroxide preparations. A Superficial skin scrapings from pityriasis
(tinea) versicolor demonstrating yeast and short mycelial forms. B A dermatophyte, in this case
T. tonsurans, demonstrating branching hyphae. A, Courtesy of Ron Rapini, M.D.
Biopsies of pityriasis (tinea) versicolor and tinea nigra are usually not performed as the KOH
examination of associated scale is usually diagnostic. In the former, both hyphal and yeast forms
are seen; although likened to 'spaghetti and meatballs', the findings more resemble 'ziti and
meatballs' (Fig. 77.3A). In the latter, KOH examination reveals septate pigmented hyphae. When
biopsy specimens are obtained, similar findings are observed within the stratum corneum. In KOH
examination of expressed follicular contents or biopsy specimens of Pityrosporum folliculitis, only
yeast forms are seen. Cultures of E. werneckii first appear as pasty, green-black colonies with a
yeast-like appearance. However, after about two weeks the appearance changes to that of a
fuzzy, dematiaceous (dark in color) mold. Culture of Malassezia is generally not indicated, but if
necessary, the plate must be overlaid with sterile oil because of its lipophilic nature.
Differential diagnosis
Piedra is generally diagnosed by clinical and microscopic inspection of a hair shaft and must be
distinguished from pediculosis (nits), hair casts, trichorrhexis nodosa, trichomycosis axillaris (see
Chapter 74 and Fig. 77.1) and the scales of psoriasis and eczema. Unlike eczema and psoriasis,
the scalp will typically appear normal in piedra.
In most patients the diagnosis of tinea nigra is made clinically and confirmed via KOH
examination and/or fungal culture. Its distinction from acral melanocytic nevi has been discussed
previously (see above); occasionally, tinea nigra could be confused with a fixed drug eruption,
post-inflammatory hyperpigmentation, or staining from chemicals, pigments and dyes. Cutaneous
melanoma has even been misdiagnosed as tinea nigra, with unfortunate results.
page 1173
page 1174
Clinical examination often leads to the correct diagnosis of pityriasis (tinea) versicolor; however,
vitiligo, pityriasis alba and other forms of postinflammatory hypopigmentation (see Chapter 66),
seborrheic dermatitis, pityriasis rosea and secondary syphilis may mimic the disease. Wood's
light examination (revealing bright yellow fluorescence) and then direct microscopy establish the
diagnosis. Pityrosporum folliculitis must be differentiated from other causes of folliculitis (see
Chapter 40, Table 40.1), in particular itching folliculitis, as well as acne vulgaris.
Treatment
Clipping hairs with adherent nodules as well as shampooing the affected hairs with 2%
ketoconazole shampoo is usually effective treatment for piedra (Table 77.3). Oral terbinafine is
possibly of some therapeutic benefit. For treatment of tinea nigra, topical keratolytic agents such
as Whitfield's ointment (typically 6% benzoic acid plus 3% salicylic acid 8) are effective, as are
topical antifungal medications, e.g. the azole and allylamine families. Several weeks of therapy
may be required to prevent recurrence of disease. Systemic therapy is generally not indicated,
and griseofulvin is not effective.
Patients with pityriasis (tinea) versicolor usually respond to topical antimycotic treatments. We
instruct the patient to treat all the skin from the neck down to the knees, even if only a small area
is clinically involved. Ketoconazole (1 or 2%) or 2.5% selenium sulfide shampoo is quite
effective. Treatment is twice weekly for two to four weeks, the preparation is left on the skin for
10-15 minutes before it is removed. Other topical alternatives include azole/allylamine creams
and lotions, 50% propylene glycol in water (cosmetically pleasing), nystatin , salicylic acid and
a variety of over-the-counter dandruff shampoos. Post-inflammatory pigmentary changes may
respond to low potency topical corticosteroids but usually require tincture of time.
Systemic therapy with ketoconazole , fluconazole or itraconazole (see Chapter 128) may
provide simple and effective treatment for pityriasis (tinea) versicolor. A regimen of short duration
(3 to 7 days) is usually successful. The rate of recurrence of pityriasis (tinea) versicolor is very
high, especially in hot humid climates. Patients at high risk for recurrence may be helped by using
ketoconazole shampoo once weekly as 'soap'. Another preventative measure is once monthly
dosing of oral ketoconazole , fluconazole or itraconazole . Blood monitoring may be required,
however, especially in the case of ketoconazole .