Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
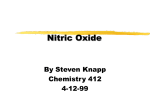
NEURAL SENSITIZATION: THE MEDICAL KEY TO TREATMENT INTRODUCTION Chemically-induced reactive airway disease (upper and lower respiratory tract, and migraines have the mechanism of neural sensitization. Respiratory effects can include sinus congestion/pain; ear pain from eustachian tube blockage (swelling), burning/sore tongue and throat, hoarseness, bronchial symptoms of coughing, chest tightness and sometimes wheezing, and shortness of breath/ difficulty getting enough air. Neural sensitization also affects the gastrointestinal (sometimes called “irritable bowel”) and genital urinary tracts (sometimes called “irritable bladder”, etc.) the blood vessel linings (endothelium), conjunctiva and skin. Burning is a common sensation in neurogenic inflammation. This widespread inflammation results in aching, fatigue, adrenal and other endocrine disturbance, and resultant depletion of amino acids, minerals and other nutrients. Inflammation and the free radicals from neural sensitization damage lipid membranes, with disproportionate damage and loss of omega 3 essential membrane lipids, because these are very vulnerable to free radical damage. This lipid damage impairs the brain and nerve cell coating (myelin). It also damages function of cell membranes and membranes of mitochondria (energy production), ribosomes (which make proteins, enzymes) DNA (genetic material), and membrane receptor sites (hormones, etc.) cell messenger sites to communicate with other cells and body organs. The blood vessel neurogenic inflammation causes reduced blood flow, and thus reduced supply of oxygen and nutrients to body organs. The red blood cell is 7 microns, the capillary only 3 microns, so inflammation reduces the blood cell’s ability to pass through. The brain is a high oxygen-demanding organ: it is only 3% of body weight but uses 20% of body oxygen at rest. Reduced blood flow in the brain in toxic encephalopathy is documented1 and impairs brain functions, since all body functions depend on oxygen supply. BIOCHEMISTRY VICIOUS CYCLE Neural sensitization occurs by activation of brain and nerve cell N-methyl-D-aspartate (NMDA), which then increases brain nitric oxide (NO).2,3,4 Several vicious biochemical cycles are then set in motion. Nitric oxide forms a tissue damaging free radical known as peroxynitrite.3,5,6,7 Peroxynitrite depletes energy ATP,8,9 which then further increases the sensitization of NMDA.10,11 Increased peroxynitrite forms excess hydroxyl radical, which in turn depletes mitochondrial (energy metabolism).12 Mitochondria are structures in body cells that generate energy by producing ATP. Mitochondria damage has been documented in the vast majority of patients with chronic illness from chemical injury.13 Peroxynitrite is a highly potent free radical that damages proteins (including enzymes), lipids (brain and, cell walls, mitochondrial membranes, ribosomal membranes and genetic DNA membranes). 14 Antioxidants such as tocopherols (natural Vitamin E), ascorbic acid (vitamin C), and glutathione help protect against these effects.14 Cofactors for superoxide dismutase (zinc, copper and manganese) and glutathione peroxidase (selenium) can also protect against damage.14 Neural sensitization is thus associated with self-perpetuating neuroexcitation and excessive response to further chemical exposure.22, 15 This NMDA activation with increased nitric oxide and peroxynitrite can cause brain cell death and neurogenerative disease.3,7,11,16,17,18 Peroxynitrite also weakens the blood-brain barrier, allowing chemicals to enter the brain more readily.19 Nitric oxide also damages the first detoxification step involving the cytochrome p450 system,20 allowing chemicals (and many drugs) to build up more in the body, further perpetuating the vicious chemical inflammation (neural sensitization) cycle. CHEMICAL CAUSATION Chemical exposure can induce neural sensitization. Pesticides such as organophosphates inhibit acetylcholine, activating muscarinic receptors, which increase nitric oxide. When muscarinic receptors are activated it releases intracellular calcium, which 092205 Page 1 of 6 activates NMDA receptors. As discussed above, NMDA activation increases nitric oxide and can induce neural sensitization. Pyrethroids slow closing of sodium channels, lowering membrane potential and thus activating NMDA receptors.21 Formaldehyde activates NMDA.2,22 Formaldehyde also stimulates the brain vanilloid receptor.23 This receptor induces sensitization by increasing nitric oxide and activating the NMDA receptor,24 which then increases peroxynitrite and sets in motion neural sensitization. Vanilloid stimulation also increases release of immune substance P. 25 Increased substance P is associated with reactive airway disease.26 Petrochemicals (VOC’s, solvents) disrupt energy production in the mitochondria, increase superoxide which increases peroxynitrite.27 This can then increase tissue-damaging free radicals in the brain.28 Peroxynitrite impairs energy metabolism by attaching proteins in the mitochondria.29,30 Exposure to carbon monoxide can increase nitric oxide and NMDA.31 Carbon monoxide induces increased activity of nitric oxide and its byproducts.32 Carbon monoxide is released in all combustion: coal, gas, gasoline/diesel, wood, tobacco, and even natural products (beeswax and other candles) and “aromatherapy”. Irritants. Petrochemicals and many other chemicals are irritants33 that with exposure can cause inflammation. Inflammation of sufficient duration can lead to chronic neurogenic inflammation.34 Inflammation results in increased cytokines, free radicals and further elevated nitric oxide. This ongoing inflammation increases artherosclerosis, increased risk of neurodegenerative (Parkinsons, Altzeimers, ALS) and other degenerative disease (osteoporosis, arthritis, etc.) and autoimmune disease. THE SCIENCE OF TREATING NEURAL SENSITIZATION This vicious cycle MUST therefore be interrupted to the maximum extent feasible. Because the resulting symptoms of sensitization are warnings that other more silent toxic-induced organ damage of the liver, pancreas, immune system, adrenals, mitochondria and other organs can be also occurring,34,35,36 masking/blocking symptoms of this cycle is not recommended without healing the disturbed biochemical mechanism. (This would be like turning off a battery warning light without fixing the battery.) Vitamin C acts to quench free radicals in water based body fluids.37 Selenium is essential in glutathione peroxidase and free radical control.37 It is critical to have a broad range of antioxidants, because they act at different locations, on different types of free radicals and complement the action of each other. 37 Major targets of free radical damage are lipid membranes37 This damages permeability, receptor function and many other membrane functions.37 This affects membranes of cells and cell structures that make energy (mitochondria), proteins (ribosomes), protect genetic material (DNA) etc. Hydroxycobalamine (B12) is a nitric oxide scavenger and deficient in the majority of chemically ill patients. 38 The cyano form is not recommended (patients don’t need cyanide and the hydroxy and methyl forms work much better in brain and nerve cells). Superoxide dismutase (SOD) is deficient in a significant portion of chemically ill patients and its cofactors, copper, zinc, and manganese must be adequate (to stop peroxynitrite from forming more nitric oxide) and other antioxidant actions of SOD.37 These SOD cofactors are often reduced in chemically injured patients and should be tested and replaced in well absorbed and transported forms, for example, picolinates. Antioxidant function is usually inadequate in chemically ill patients,35 and increased lipid peroxides and other free radicals are common. Intervention to help reduce this vicious biochemical cycle includes: hydroxycobalamine (nitric oxide scavenger) by nebulizer and nasal for rapid action in exacerbations (not oral due to poor absorption), general antioxidants (C, E, selenium), glutathione by nebulizer due to poor oral absorption, and ample alpha lipoic acid and riboflavin as cofactors to reactivate the glutathione in the many damaged lipid tissues Page 2 of 6 (cell membranes, mitochondria, lymph, brain, etc.). Sublingual cobalamine is also absorbed and effective therapy, 39 although adding to nebulizer just prior to nebulizer use works faster and better. Trimethyl glycine is recommended as a methyl donor to reduce the effects of peroxynitrite. Magnesium should be ample because deficiency is very common with toxic injury and adequate magnesium decreases NMDA activation. Peroxynitrite scavengers such as a mixture of caretenoids are also recommended. Caretenoids tend to be more organ-specific. An inclusion of gingko (brain), silimarin (liver), bilberry (collagen stabilizing, capillary permeability, vision), cranberry (urinary) and other mixed caretenoids is recommended. Mineral levels should be measured and followed by intracellular (eg. RBC) or lipid functional (eg. lymphocyte mitogenesis, a SpectraCell technology). Functional lymphocyte evaluation and follow-up of glutathione, lipoic acid, total antioxidant function, C, E and zinc is also recommended. At this time this technology is only available through SpectraCell laboratory. Nasal hydroxycobalamine is rapidly absorbed, well tolerated,40,41 and increases body levels.41 Nasal hydroxycobalamine is also effective in reducing frequency and severity of migraines, acting as a nitric oxide scavenger.42 Alpha lipoic acid is a potent and lipophilic antioxidant, which protects lipid membranes 43 of cells, cell structures (including the energy-generating mitochondria) and myelin.43 It has been used in Germany for decades to treat neuropathy.44 Magnesium acts as a blocker of the NMDA nerve receptor, thus reducing neuropathic pain and its resultant inflammation.45 Bilberry is a potent anthiocyanoside flavinoid antioxidant that reduces capillary fragility and permeability46 and improves damaged neurologic function.47 REACTIVATION OF GLUTATHIONE Glutathione is the most important intracellular antioxidant in the body. Improving levels in the mid and lower respiratory tract can help reduce respiratory responses to irritants and help to reduce the severity and duration of the patient's reactions. A nasal form of glutathione may be used for reactions that harm brain function. A glutathione nasal spray has also reduced symptoms in people with chronic rhinitis.48 There is no blood- brain barrier between the nose and the brain. Scientific studies document that substances being breathed into the nose directly enter the brain. Glutathione can also be absorbed through the lungs (delivered to the lungs as an aerosol) and seems able to cross the blood-brain barrier.49 It is thus effectively delivered by nebulizer, avoiding need of IV/injection use. Nebulizer technology is developing to allow rapid efficient delivery without noticeable noise or vibration, eg AeronebGo (800-759-3038 or available at near cost through Key Pharmacy 800-8781322. The AeronebGo is polycarbonate: thus durable with minimal off gassing. It is small, easily portable, and has a small battery pack (eg for travel) and separate plug in for electric outlets. None of the above is a substitute for exposure controls at home, work and/or school: places where the person spends most of their time. Humans are social beings, and these measures above gradually increase the person’s ability to enjoy the company of others and use public places. When society is adequately informed and takes public health reasonable accommodation measures to reduce irritants and toxins in personal products and public places, this further promotes health and reduces sensitization. Without adequate antioxidant protection, there is increased risk of inflammation and degenerative diseases37, lung damage50, 51 and other cellular injury.52 Page 3 of 6 Neural Sensitization Cycle Carbon Monoxide Solvents, VOC’s Formaldehyde, Isocyanates NMDA RECEPTOR Pesticides (Organophosphates, Carbamates) Nitric Oxide SOD Superoxide Peroxynitrite Tissue Injury Inflammation Respiratory, GI, GU, endothelial, skin) P Gregersen, “Chronic Toxic Encephalopathy in Solvent-exposed Painters in Denmark 1976-1980: Clinical cases and social consequences after a 5-year follow-up”, Am J of Ind Med , 11: 399-417, 1987. 2 JE Haley etal., “Evidence for spinal N-methyl-D-aspartate receptor involvement in prolonged chemical nociception in the rat”, Brain Res 518:218-226, 1990. 3 M Lafon-Cazal etal., “Nitric oxide, superoxide and peroxynitrite: putative mediation of NMDA-induced cell death in cerebellar cells”, Neuropharmacology 32:1259-1266, 1999. 1 Page 4 of 6 IJ Reynolds and TG Hastings, “Glutamate produces production of reactive oxygen species in cultured forebrain neurons following NMDA receptor activation”, J. Neurosci 15:3318-3327, 1995. 5 JS Beckman, “The double edged role of nitric oxide in brain function and superoxide-mediated injury”, J. Dev Physiol 15:53-59, 1991. 6 M Lafon-Cazal etal., “NMDA-dependent superoxide production and neurotoxicity”, Nature 364:535-537, 1993. 7 JT Coyle and P Puttfarken, “Oxidative stress, glutamate and neuro generative disorders”, Science 262:689-695, 1993. 8 JS Beckman and JP Crow, “Pathologic implications of nitric oxide, superoxide and peroxynitrite formation”, Biochem Soc Trans 21:330-333, 1993. 9 WA Pryor and GL Squadrito, “The chemistry of peroxynitrite: a product of the reaction of nitric oxide and superoxide”, Am J. Physiol 268:L699-L722, 1995. 10 A Novelli etal., “Glutamate becomes neurotoxic via the NMDA receptor when intracellular energy levels become reduced”, Brain Res 451:205-212, 1988. 11 JB Schultz etal., “The role of mitochondrial dysfunction and neuronal nitric oxide in animal models of neurodegenerative diseases”, Mol Cell Biochem 174:171-184, 1997. 12 M Hayakawa etal “Age-related oxygen damage and mutations in mitochondrial DNA in human hearts”, Biochem Biophys Res Commun 189: 979-985, 1992. 13 G Ziem, “Profile of patients with chemical injury and sensitivity”, Int J Toxicol 18:401-409. 14 AY Sun YM Chen, “Oxidative stress and neurodegenerative disorders”, J Biomed Sci, 5: 401-14, 1998. 15 WD Willis, Role of neurotransmitters in sensitization of pain responses,” Ann NY Acad Sci 933;175184, 2001. 16 A Doble, “NMDA and neurodegenerative conditions (reviews)”, Pharmacol Ther 81:163-221, 1999. 17 VL Dawson and TM Dawson, “Nitric oxide neurotoxicity”, J Chem Neuroanat 10:179-190, 1996. 18 BC Albenzi, “Models of brain injury and alterations in synaptic neuroplasticity”, J. Neurosci Res 65:279-283, 2001. 19 WG Mayhan, “Nitric oxide donor-induced increase in permeability of the blood-brain barrier”, Brain Res 866;101-108, 2000. 20 OG Khatsenko etal., “Nitric oxide is a mediator of the decrease in cytochrome p450-dependent metabolism caused by immunostimulants”, Proc Nat Acad Sci USA 90:11147-11151, 1993. 21 A Wu and Y Lin, Brain Res Mol Brain Res 110: 147, 2003. 22 SB McMahon etal., “Central excitability triggered by noxious inputs”, Current Opin Neurobiol 3:602610, 1993. 23 A Beiruth etal, “Spinal and supraspinal antinociceptive action of dipyrone in formalin, capsaicin and glutamate tests. Study of the mechanism of action, “Env J Pharmacol 345: 233-245, 1998. 24 E Palazzo etal, “Interaction between vanilloid and glutamate receptors in the central modulation of nociception:, Env J Pharmacol 439- 69-75, 2002. 25 H Kimata etal, “Effect of exposure to volatile organic compounds on plasma levels of neuropeptides, nerve growth factor and histamine in patients with chemical sensitivity”, Int J Hyg Environ Health 159-63, 2004. 26 WJ Meggs, “The toxic induction of asthma and rhinitis”, Clinical Toxicol 32: 487-501, 1994. 27 TR Garbe and H Yukama, “Common solvent toxicity: auto oxidation of respiratory redox-cyclers enforced by membrane derangement”, Z Natur forsch 56:483-491, 2001. 28 CJ Mattia etal., “Toluene-induced oxidative stress in several brain regions and other organs”, Mol Chem Neurophysiol 18:313-328, 1993. 29 JS Bechman and JP Crow, “Pathological implications of nitric oxide, superoxide and peroxynitrite function”, Biochem Soc Trans 21: 330-334, 1993. 30 WA Pryor and G Squadrito, “The chemistry of peroxynitrite: a product of the reaction of nitric oxide and superoxide”, Am J Physiol 268:L 699-L722, 1995. 31 SR Thom etal “Neuronal nitric oxide synthase and n-methyl-d-aspartate neurons in experimental carbon monoxide poisoning”, Toxicol Applied Pharmacol 194: 280-295, 2004. 32 A Verma, etal., “Carbonless Monoxide: A Putative Neural Messenger”, Science 259: 381-384, 1993. 33 RE Lenga, Ed., Sigma-Aldrich Library of Chemical Safety Data. Sigma-Aldrich Corp, 1988. 34 GE Ziem, “Evaluation and Treatment of Patients with Chemical Injury and Sensitivity” presented to a conference sponsored by the National Institute of Environmental Health Sciences, August 2001. 35 GE Ziem, “Profile of Patients with Chemical Injury and Sensitivity”, Int J Toxicol 18:401-409, 1999. 36 GE Ziem, Invited presentation: Endocrine changes in Patients with Chronic Illness Following Chemical Overexposure. 37 LJ Machlin and A Bendich “Free radical damage: protective role of antioxidant nutrients. 4 Page 5 of 6 G Ziem, “Medical evaluation and treatment of patients with chemical injury and sensitivity”, Invited speaker at Aug 13-15, 2001 Conference sponsored by the National Institute of Environmental Health Sciences. 39 G Delpre etal, Sublingual therapy for cobalamin deficiency as an alternative to oral and parenteral cobalamin supplementation”. The Lancet Vol 354, Aug. 28, 1999. 40 D Z van Asselt etal., “Nasal absorption of hydroxycobalamine in healthy elderly adults”, Brit J Pharmacol 45: 8386, 1998. 41 W B Slot, etal., “Normalization of plasma vitamin B12 by intranasal hydroxycobalamine in vitamin B12 deficient patients”, Gastroenterology 113: 430-433, 1997. 42 P H van der Kuy etal., “Hydroxycobalamine, a nitric oxide scavenger in the prophylaxis of migraine”, Cephalgia 22: 513-519, 2002. 43 T Konrad etal, “Alpha-lipoic acid decreases serum lactate and pyruate and improves glucose effectiveness in lean and obese patients with type 2 diabetes”, Diabetes Care 22: 280-287, 1999. 44 D Ziegler etal, Alpha-lipoic acid in the treatment of diabetic polyneuropathy in Germany: current evidence from clinical trials”, Exp Clin Endocrinol Diabetes 107: 421-430, 1999. 45 M Jones, “Chronic neuropathic pain: pharmacological in the new millennium”, Internat J. Pharmaceurical Compounding, Jan-Feb 2000. 46 F Cohen-Boulakia et al, “In vivo sequential study of skeletal muscle capillary fragility in diabetic rats: effects of anthocyanosides”. Metabolism 49: 880-885, 2000. 47 M Perossini etal, “Diabetic and hypertensive retinopathy therapy with vaccinium myrtillus anthocyanosides: a double blind, placebo-controlled trial”, Ann Ofthalm Clin Ocul 113: 1173-1190, 1987. 48 Testa B, Mesolella M, Testa D. Glutathione in the upper respiratory tract. Ann Otol Rhinol Laryngol 1995;101:117-9. 49 R Buhl, etal. Oxidant-protease interaction in the lung. Prospects for anti oxidant therapy. Chest 110:267S-272S, 1996 50 IN Roehm etal, “The influence of vitamin E on the lung fatty acids of rats exposed to ozone”, Archiv Environ Health 24: 237-242, 1972. 51 H Sprince etal, “Comparison of protection by L-ascorbic acid, L-cysteine, formaldehyde toxicity”, agents and actions 9: 407-414, 1979. 52 GA Pascoe etal, “A role of vitamin E in protection against cell injury, Env J Biochem 166: 241-247, 1987. 38 Page 6 of 6