Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
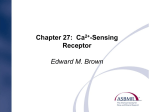
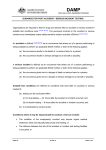
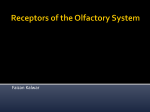
0021-972X/00/$03.00/0 The Journal of Clinical Endocrinology & Metabolism Copyright © 2000 by The Endocrine Society Vol. 85, No. 4 Printed in U.S.A. A Large Homozygous or Heterozygous In-Frame Deletion within the Calcium-Sensing Receptor’s Carboxylterminal Cytoplasmic Tail That Causes Autosomal Dominant Hypocalcemia* ANNE LIENHARDT, MICHÈLE GARABÉDIAN, MEI BAI, CHRISTIANE SINDING, ZAIXIANG ZHANG, JEAN-PIERRE LAGARDE, JEAN BOULESTEIX, MICHEL RIGAUD, EDWARD M. BROWN, AND MARIE-LAURE KOTTLER Service de Pédiatrie 2 (A.L., J.B.), Centre Hospitalier Universitaire, 87042 Limoges, France; Centre National de la Recherche Scientifique Unité Proper de Recherche 1524 (M.G., C.S.), Hôpital Saint Vincent de Paul, 75014 Paris, France; Endocrine-Hypertension Division (M.B., Z.Z., E.M.B.), Department of Medicine, Brigham and Women’s Hospital, and Harvard Medical School, Boston, Massachusetts 02115; Unité de Biologie Moléculaire (J.-P.L., M.-L.K.), Service de Biochimie Médicale, AP-HP, Hôpital Pitié-Salpétrière, 75013 Paris, France; and Service de Biochimie (A.L., M.R.), Faculté de Médecine, 87025 Limoges, France ABSTRACT Autosomal dominant hypocalcemia (ADH) can result from heterozygous missense activating mutations of the calcium-sensing receptor (CaSR) gene, a G-protein-coupled receptor playing key roles in mineral ion metabolism. We now describe an ADH kindred of three generations caused by a novel CaSR mutation, a large in-frame deletion of 181 amino acids within its carboxylterminal-tail from S895 to V1075. Interestingly, the affected grandfather is homozygous for the deletion but no more severely affected than heterozygous affected individuals. Functional properties of mutant and wild-type (WT) CaSRs were studied in transiently transfected, fura-2-loaded human embryonic kidney (HEK293) cells. The mutant receptor exhibited a I SOLATED hypoparathyroidism is a disorder of calcium metabolism characterized by hypocalcemia associated with a low level of serum PTH. Although most cases are sporadic, some have autosomal dominant, autosomal recessive or Xlinked modes of inheritance (1). Linkage analysis performed in large families with autosomal dominant hypoparathyroidism mapped a candidate gene to the locus 3q13, corresponding to the region of chromosome 3 harboring the gene encoding the human calcium-sensing receptor (CaSR) (2– 4). The bovine receptor was first cloned in 1993 (5) and then the human CaSR in 1995 (6); it belongs to a new subfamily of the G-protein-coupled receptors (GPCR) that includes the metabotropic glutamate receptors (7, 8), gamma aminobutyric acid (GABAB) receptors (9), putative pheromone receptors (10 –12), and other recently cloned taste receptors (13). This subfamily of GPCRs is charReceived October 1, 1999. Revision received January 5, 2000. Accepted January 6, 2000. Address correspondence and requests for reprints to: Dr. Anne Lienhardt, Service de Pédiatrie 2, Centre Hospitalier Universitaire Dupuytren, 2 avenue Martin Luther King, 87042 Limoges cedex, France. E-mail: [email protected]. * Generous grant support for this work was provided by The Faculté de Médecine de Limoges, L’Assistance Publique-Hôpitaux de Paris, France and by The St. Giles Foundation (to E.M.B.) and NIH Grants DK52005 (to E.M.B.), DK48330 (to E.M.B.), and DK54934 (to M.B.). gain-of-function, but there was no difference between cells transfected with mutant complementary DNA alone or cotransfected with mutant and WT complementary DNAs, consistent with the similar phenotypes of heterozygous and homozygous family members. Therefore, this activating deletion may exert a dominant positive effect on the WT CaSR. The mutant receptor’s cell surface expression was greater than that of the WT CaSR, potentially contributing to its gain-offunction. This novel mutation in the CaSR gene provides the first known examples of a large naturally occurring deletion within a G-protein-coupled receptor’s carboxylterminal-tail and of a homozygous, affected individual with ADH. (J Clin Endocrinol Metab 85: 1695–1702, 2000) acterized by very large (⬃600 amino acids) extracellular domains and long carboxylterminal (C) intracellular tails. Soon after the cloning of the CaSR, heterozygous activating mutations within its gene were reported as a cause of familial hypoparathyroidism (14). The elucidation of the molecular basis for this form of familial hypoparathyroidism with a dominant inheritance pattern identified a distinct clinical entity among the various forms of hypoparathyroidism, autosomal dominant hypocalcemia (ADH) (15). ADH is a rare inherited disease that can come to clinical attention at any time of life. The clinical presentation is variable, ranging from asymptomatic forms to severe neonatal seizures. However, the biochemical features of the condition are more uniform, showing mild-to-moderate or, occasionally, more severe, hypocalcemia and hyperphosphatemia accompanied by low or normal serum levels of PTH and normal or elevated levels of urinary calcium excretion despite low serum calcium concentrations (15–17). We now report a family with mild hypocalcemia inherited as a dominant trait that is caused by an unusual mutation in the CaSR gene (a deletion within its C-terminal tail), resulting in a substantially shortened C-tail. Furthermore, we demonstrate that the mutant receptor exhibits a gain-of-function, showing a reduction in the level of the extracellular calcium 1695 1696 LIENHARDT ET AL. concentration (Ca2⫹o), producing half-maximal CaSR-elicited increases in the cytosolic calcium concentration (Ca2⫹i), presumably caused by receptor-mediated activation of phospholipase C (18). This naturally occurring deletion in the CaSR’s C-tail provides insights into the normal structurefunction relationships of this part of the receptor and affords direct, in vivo support of previous in vitro observations that truncations within the CaSR’s C-tail can lead to increased cell surface expression and activity of this receptor (19). Finally, to our knowledge, the mutation in the CaSR gene in this family provides the first example of a homozygous, affected individual in a kindred with ADH. Subjects and Methods Patients Seven members from the same kindred were studied (five males and two females). Informed consent was obtained from all subjects, according to the guidelines of the French consultative committee for the protection of human studies. Amplification of genomic DNA and sequence analysis Samples of venous blood were obtained, and genomic DNA was extracted from leukocytes using a proteinase K-phenol-chloroform procedure (20). Exons 2–7 of the CaSR gene, encompassing the entire coding sequence, were amplified using the PCR with previously reported primers (21, 22), except for exon 7, which was amplified in two segments: 1) segment A, the 5⬘ portion; and 2) segment B, the remainder of the exon. The sequences of the primers were as follows: 7B: 5⬘-GTCTGGATCTCC TTCATTCCA-3⬘ (nucleotides 2449 –2469); 7BR: 5⬘-TCTGGGGGATTCCTCAT CCC-3⬘ (within the 3⬘ non-coding, flanking region of the gene); and 7BDR: 5⬘-TTTCTGTAACAGTGCTGCCTC-3⬘ (nucleotides 3220 – 3200). Primers 7B, 7BR, and 7BDR were designed to amplify the segment B, based on the DNA sequence deposited in GenBank (accession number X81086). The primer pair 7B and 7BR amplifies all of B, whereas the primer pair 7B and 7BDR amplifies a portion of B from the wild-type (WT) CaSR gene. PCR products were electrophoresed on 1% agarose gels, visualized with ethidium bromide, and then purified on Microcon-100 columns (AMICON, Beverly, MA). Both strands of the products were directly sequenced using the Amplitaq dye Terminator Cycle Sequencing kit and an AB PRISM 377 DNA sequencer (PerkinElmer Corp., Roissy, France). Construction of the Flag-tagged mutant CaSR The mutation identified in this family’s CaSR gene (a large deletion within the C-tail) was engineered into a reconstructed WT CaSR complementary DNA (cDNA) by using the PCR as follows: cassette 6 (23) of the reconstructed CaSR cDNA, containing the deletion in this family’s CaSR, was amplified using a pair of primers with the sequences, 5⬘CGGGGTACCTCGAGGATGAGATCATCTTCAT-3⬘ and 5⬘-GCTCTAGATTATG AATTCACTACGTTGCTGCGGCGCAG-3⬘. The PCR product was subsequently digested with XhoI and XbaI and ligated to the larger of the digested fragments of the reconstructed, Flag-tagged, WT receptor in pcDNA3 to produce the mutant receptor in a form suitable for expression studies (23). The presence of the mutation was confirmed by direct sequencing. Transient expression of the WT CaSR and the mutated CaSR harboring the deletion within the C-tail in HEK293 cells DNA was prepared using the Midi Plasmid kit (QIAGEN, Chatsworth, CA). Lipofectamine (Life Technologies, Gaithersburg, MD) was employed as the DNA carrier for transfection. Human embryonic kidney (HEK293) cells (provided by NPS Pharmaceuticals, Inc., Salt Lake City, UT) were cultured in DMEM (Life Technologies). Transient transfection was performed, as previously described, by adding a DNA-lipofectamine mixture diluted with OPTI-MEM 1 Reduced Serum Medium JCE & M • 2000 Vol 85 • No 4 (Life Technologies) to 90% confluent HEK293 cells plated in 13.5 ⫻ 20.1-mm glass coverslips for measurement of CaSR-mediated changes in Ca2⫹i or in six-well plates for preparation of cellular proteins for Western analysis using 0.625 g cDNA (23). After 5 h incubation at 37 C, an amount of OPTI-MEM 1 Reduced Serum Medium with 20% FCS equal to that present in the wells was added to the transfected cells, which was then replaced with fresh DMEM and 10% FCS at 24 h after the start of transfection. The expressed CaSR protein was assayed at 48 h after transfection. To perform coexpression of the WT and mutant receptors, 0.625 g of each cDNA were mixed and used to transfect HEK293 cells, as described above. Measurement of Ca2⫹i by fluorimetry in cell populations Coverslips with nearly confluent HEK293 cells previously transfected with the appropriate CaSR cDNAs were loaded for 2 h at room temperature with fura-2/AM (Molecular Probes, Inc., Eugene, OR) in 20 mmol/L HEPES (pH 7.4) containing 125 mmol/L NaCl, 4 mmol/L KCl, 1.25 mmol/L CaCl2, 1 mmol/L MgSO4, 1 mmol/L NaH2PO4, 0.1% BSA, and 0.1% dextrose and were washed once with bath solution (20 mmol/L HEPES (pH 7.4) containing 125 mmol/L NaCl, 4 mmol/L KCl, 0.5 mmol/L CaCl2, 0.5 mmol/L MgCl2, 0.1% dextrose, and 0.1% BSA) at 37 C for 20 min. The coverslips were then placed diagonally in a thermostatted quartz cuvette containing the bath solution using a modification of the technique employed previously in this laboratory (23). Extracellular calcium was increased stepwise to give the desired final concentrations with additions of Ca2⫹o in increments of 1 mmol/L, which were followed by 5 mmol/L increments after achieving a level of 5.5 mmol/L Ca2⫹o. Excitation monochrometers were centered at 340 nm and 380 nm, and emitted light was collected at 510 ⫾ 40 nm through a wide-band emission filter. The 340/380 excitation ratio of emitted light was used to evaluate changes in Ca2⫹i, as described previously (23). Western analysis of CaSRs expressed on the cell surface and in whole cell lysates Before preparing whole-cell lysates, intact HEK293 cells transiently transfected with the Flag-tagged WT or mutated CaSR were labeled with ImmunoPure Sulfo-NHS-Biotin (Pierce Chemical Co., Rockford, IL) (23). The whole cell lysate was prepared in a nondenaturing buffer [1% Triton X-100, 0.5% NP-40, 150 mmol/L NaCl, 10 mmol/L Tris-HCl (pH 7.4), 2 mmol/L EDTA, 1 mmol/L EGTA, 100 m iodoacetamide, and a cocktail of protease inhibitors including 83 g/mL aprotinin, 30 g/mL leupeptin, 1 mg/mL pefabloc, 50 g/mL calpain inhibitor, 50 g/mL bestatin, and 5 g/mL pepstatin]. Flag-tagged CaSRs were solubilized and immunoprecipitated with anti-Flag M2 monoclonal antibody (VWR Scientific, Bridgeport, NJ), resolved by SDS-polyacrylamide gel electrophoresis (PAGE, 5%–9% gradient gel) under reducing conditions, and blotted on nitrocellulose membranes. After blocking with 5% milk, the forms of the receptor present on the cell surface were detected using an avidin-horseradish peroxidase conjugate (Bio-Rad Laboratories, Inc., Rockville Center, NY), followed by visualizing the biotinylated bands with an enhanced chemiluminescence system (Amersham Pharmacia Biotech, Piscataway, NJ). After removal of the avidin, using the recommended procedure for stripping the blots (Amersham Pharmacia Biotech), all forms of the CaSR on the same blot were detected using anti-CaSR antiserum, 4641, a polyclonal antiserum raised against a peptide within the extracellular domain of the CaSR (corresponding to residues 214 –236 of the human CaSR; kindly provided by Drs. Forrest Fuller and Rachel Simin at NPS Pharmaceuticals, Inc.), followed by a secondary, horseradish peroxidase-conjugated goat antirabbit antibody and then an enhanced chemiluminescence system (Amersham Pharmacia Biotech). Statistical analysis The mean EC50 (the effective concentration of Ca2⫹o giving one half of the maximal response) for the WT or mutant receptors in response to increasing concentrations of Ca2⫹o were calculated from the EC50 s for all of the individual experiments and were expressed with the sem as the index of dispersion. Comparison of the EC50 s was performed using ANOVA. A P value of less than or equal to 0.05 was considered to indicate a statistically significant result. LARGE DELETION WITHIN THE CaSR TAIL Results Clinical features of affected and unaffected family members Seven members of the family were studied, and the family pedigree is shown in Fig. 1A: two family members are normal, with respect to calcium metabolism (II1 and III3), and five are affected (I2, II2, III1, III2, and III4). Pertinent clinical features of the affected patients are reported in Table 1, and Table 2 summarizes the biological data including those of subject III3. None had severe clinical signs or symptoms of hypocalcemia. The oldest was discovered to have hypocalcemia during a hospitalization after an accidental fall; later, he reported mild muscle cramps of many years duration. After the discovery of this individual’s hypocalcemia, no further family studies were carried out at that time. Eight years later, his daughter (subject II2) presented with muscle cramps during her second pregnancy and was found to be hypocalcemic. Both of these family members felt otherwise well. A family survey was then performed. A total of four affected individuals have experienced transient signs of neuromuscular irritability. All affected members had, before treatment, total and ionized hypocalcemia and showed normal or elevated rates of urinary calcium excretion despite their low serum calcium concentrations. PCR and DNA sequence analysis of the mutation An initial screening was performed of the PCR products amplified from the various regions of the coding sequence of FIG. 1. A, Pedigree of the family with dominant hypocalcemia. Patients I2, II2, III1, III2, and III4 are affected; hatching indicates affected family members with the heterozygous state, and the filled symbol denotes a family member with the homozygous state. B, Analysis of PCR products amplified from the distal half of Exon 7 from affected and unaffected family members. PCR products amplified from genomic DNA, using primers 7B/7BR, were analyzed by electrophoresis on a 1% agarose gel. M, Molecular weight markers generated by digestion of DNA from bacteriophage ⌽X174 with HaeIII (Bioprobe, Quantum, Montreuil, France); T, PCR control without added DNA. 1697 TABLE 1. Clinical features of the 5 hypocalcemic patients in the untreated state Patient Age at diagnosis (years) I2 II2 III1 50 28 5 III2 III4 Mode of presentation at diagnosis Muscle cramps, general fatigue Muscle cramps during pregnancy Febrile neuromuscular irritability (Normocalcemic at birth) Birth (familial survey) Asymptomatic neonatal hypocalcemia Paresthesias at 8 Birth (familial survey) Asymptomatic neonatal hypocalcemia the CaSR gene using agarose gel electrophoresis. Within the distal half of the seventh exon, affected family members exhibited a PCR product that differed from that amplified from unaffected members, as shown in Fig. 1B. One band at the predicted size of 868 bp was detected in the products amplified from the 2 unaffected members of the family (II1 and III3), whereas 2 bands were detected in 4 of the affected individuals (II2, III1, III2, and III4). The larger of the 2 bands was of the expected size, and the smaller was about 325 bp in length. Only the smaller band was amplified from genomic DNA of patient I2. Direct sequencing of the smaller band revealed a deletion of 543 bp within exon 7, beginning at nucleotide 2682 and ending at nucleotide 3224 (Fig. 2). The messenger RNA species generated as a result of the deletion is predicted to encode a protein of only 897 amino acids, with a deletion of 181 residues within the cytoplasmic tail, from Serine 895 to Valine 1075, and then terminating with the 3 residues normally present at the end of the CaSR’s C-tail (also see Fig. 3). The smaller band observed on gel electrophoresis corresponds to the PCR product amplified from the mutant allele, whereas the larger band corresponds to that amplified from the normal allele. The deletion was inherited as a heterozygous trait in affected family members II2, III1, III2, and III4, which is compatible with the diagnosis of ADH in this family. Using primers 7B (designed within the seventh exon) and 7BDR (designed within the deletion), only one band at the predicted size of 771 bp was found after PCR amplification of the DNA extracted from all members of the family, normal and affected, except patient I2. No band was visualized for patient I2, confirming his homozygous genotype, with respect to the deletion (data not shown). Moreover, we screened DNA from 50 normal unrelated individuals using gel electrophoresis of PCR products amplified from the second part of the seventh exon; all had a single band at the expected size for a product amplified from the normal CaSR gene (data not shown). Functional study of the mutant CaSR containing the deletion in the C-tail Figure 4 shows typical dose-response curves for the WT and mutated receptors, with respect to the elevations in Ca2⫹i elicited by increasing levels of Ca2⫹o when expressed transiently in HEK293 cells. Compared with the WT CaSR, the mutant receptor exhibited a statistically significantly leftshifted dose-response curve with a reduced EC50 for Ca2⫹oinduced changes in Ca2⫹i (2.2 mmol/L vs. 3.3 mmol/L). 1698 JCE & M • 2000 Vol 85 • No 4 LIENHARDT ET AL. TABLE 2. Biological features of the patients before treatment Patient I2 II2 III1 III2 III3 (Unaffected) III4 Serum calcium (mg/dL) b 6.6–7.6 [9.0–10.2] 6.5–7.1b [9.0–10.2] 7.1–7.3b [9.0–10.2] 7.1–7.6b [8.8–10.4] 8.7–9.9 [8.8–10.4] 7.4– 8.8b [8.8–10.4] Ionized Ca (mg/dL) Serum PO4 (mg/dL) Serum PTHa (pg/mL) Urinary Ca (mg/kg䡠day) ND 3.6– 4.2 [2.5– 4.6] 4.1– 4.9 [2.5– 4.6] 7.0–7.6b [3.7–5.3] 6.3–7.0 [5.6– 6.8] 5.8– 6.1 [5.6– 6.8] 5.4– 6.8 [5.6– 6.8] 0.5 ng/mlb [1– 6] 5–12b [15– 60] 7b [15– 60] 8b [15– 60] 17–22 [15– 60] 2– 6b [15– 60] 245 mg/dc [⬍250] 148 mg/dc [⬍250] 1 –5b [⬍4] 4 – 6b [⬍4] 0.69 [⬍4] 4 [⬍4] 3.4–3.6b [4.6–5.2] 3.3–3.9b [4.8–5.4] 3.4– 4.2b [4.8–5.4] ND 3.7b [4.8–5.4] ND, Not determined. Reference values according to age are given in brackets for each parameter. a An immunoradiometric assay specific for intact PTH (1– 84) was used for patients in the 2nd and 3rd generations, whereas a C-terminal PTH assay was used for patient I2. b Abnormal values. c Urinary calcium excretion is given as mg/d for the adult patients. FIG. 2. Direct sequencing of the mutated CaSR allele shows a large deletion within the distal portion of exon 7 from nucleotide (NT) 2682 to 3224. The corresponding amino acid (AA) sequence is indicated below. International abbreviations have been used for the nucleotides and amino acids. When the mutant receptor was cotransfected with the WT CaSR, to mimic the in vivo heterozygous state, the resultant EC50 did not differ statistically from that of the mutant receptor expressed by itself. Western analysis of the transiently expressed WT and mutant CaSRs Figure 5A shows that the mutant receptor was expressed on the cell surface at a substantially higher level than that of the WT CaSR. In addition, the ratio of the mature species of the receptor (the higher of the two bands in the doublet at 140 –160 kDa) (23) to the immature one (the lower band of the doublet) is much greater for the mutant than for the WT CaSR (Fig. 5B), suggesting that the mutant receptor CaSR is processed much more efficiently than the WT receptor. Discussion In the present study, we have identified a novel mutation in the CaSR gene associated with familial ADH. The clinical and biochemical features of the affected members of this LARGE DELETION WITHIN THE CaSR TAIL 1699 FIG. 3. Schematic diagram of the human CaSR. The shaded areas depict the transmembrane domains (TM); gainof-function mutations previously described are identified by asterisks, and carboxylterminal truncations that have been produced by directed mutagenesis are also indicated. The two arrows show the location within the receptor’s C-tail of the present deletion. family are similar to those reported previously in ADH, including transient signs of neuromuscular irritability and asthenia, as well as hypocalcemia associated with inappropriately low serum levels of PTH and inappropriately normal or elevated levels of urinary calcium excretion, given their hypocalcemia. All cases of ADH identified to date have been caused by missense activating mutations of the CaSR gene. After the first report of such a CaSR mutation in a family with ADH, 13 additional, unique mutations in the CaSR gene have been described associated with either familial or sporadic hypocalcemia (14, 17, 23–28). All of these mutations have been missense mutations, and most (9 of 13) are localized within the CaSR’s extracellular domain, which is the ligandbinding domain (29). The other mutations are present within the first extracellular loop or in the fifth or sixth transmembrane domains (see Fig. 3). We have now identified a large, in-frame deletion of 181 amino acids within the CaSR’s C-tail between Serine 895 (S895) to Valine 1075 (V1075) that is followed by a short sequence of three amino acid residues that are normally present at the CaSR’s extreme C-terminus. In vitro functional expression of a mutant receptor, engineered to include this deletion, confirms that it exhibits the expected gain-of-function. That is, the dose-response curve for the mutant receptor showed a significant leftward shift for its activation by elevated levels of Ca2⫹o, the CaSR’s principal physiological agonist, which reduced the EC50 from 3.3 mmol/L for the WT to 2.2 mmol/L for the mutant receptor. In accord with previous results observed with a CaSR engineered to include a truncated C-tail (S892stop) (30), this large deletion of the tail is characterized by a higher biological activity (i.e. reduced EC50) than that of the WT receptor, which could readily account for the clinical and biochemical features of affected family members. Therefore, we can conclude that this family represents another example of ADH, although it represents one caused by a novel form of CaSR mutation that has not be described previously, i.e. a truncation within the C-tail. To date, gain-of-function mutations in GPCRs have been described in the heterozygous state, as is also the case for the previously described families with ADH and sporadic cases of activating mutations causing the same biochemical phenotype (14, 17, 23–28). The first-generation patient of the present family seems to be the first case of ADH caused by an activating mutation of the CaSR present in the homozygous state. Perhaps surprisingly, this patient’s clinical and biochemical features were no more severe than those of family members heterozygous for the same mutation. To explore further the basis for the similar clinical features in this ho- 1700 LIENHARDT ET AL. FIG. 4. High Ca2⫹o-evoked increases in Ca2⫹i in fura-2-loaded HEK293 cells transiently transfected with the WT or mutant CaSR alone or cotransfected with the WT and mutant receptors. Cells were transfected with the various receptor constructs, and Ca2⫹o-induced changes in Ca2⫹i were determined as described in Subjects and Methods. Each data point is the mean value of 4 – 6 measurements. The responses are normalized to the maximum response of the WT receptor. The SEM is indicated with a vertical bar through each point. The EC50 for each curve is presented as mean ⫾ SEM. The mean EC50 for the mutant receptor alone and those for the cotransfected WT and mutant receptors were not significantly different (P ⬎ 0.05). In this experiment, 0.625 g of each cDNA was employed to transfect HEK293 cells plated on rectangular coverslips (within individual wells of 12-well plates). mozygous individual and in heterozygous family members, we compared the EC50 for Ca2⫹o-evoked increases in Ca2⫹i in HEK293 cells transfected with 1) the WT CaSR cDNA alone; 2) the mutated CaSR cDNA receptor alone (to reproduce the homozygous state); or 3) both the WT and the mutated CaSR cDNAs (to mimic the heterozygous state). The EC50 of the M/M and the M/WT transfected cells were not significantly different (2.2 mmol/L vs. 2.2 mmol/L). Therefore, the homozygous state of this deletion mutation does not produce a greater gain-of-function than observed for the heterozygous state. Recent in vitro studies have shown that the CaSR is expressed on the cell surface principally as a dimer, and the cytoplasmic tail of the receptor is not required for dimerization (30). The dimerization of the CaSR, however, seems to be functionally significant, because heterodimeric CaSR comprising two different, individually inactive mutated CaSRs can reconstitute signal transduction (31). This result strongly suggests that the two monomers within the dimeric CaSR can interact in some manner to produce optimal activation of signal transduction. Moreover, one inactivating missense CaSR mutation (R185Q) exhibits a dominant negative effect on the cotransfected WT monomer, leading to substantial loss of function when coexpressed in HEK293 JCE & M • 2000 Vol 85 • No 4 FIG. 5. Western analysis of WT and mutant receptors. Proteins were isolated from HEK293 cells transiently transfected with the WT or mutant CaSR cDNAs and were subjected to SDS-PAGE on a linear gradient running gel of 5–9%, followed by analysis for cell surface expression of the CaSR (A) or Western blotting (B), as described in Subjects and Methods. In each panel, lane 1 represents WT receptor, and lane 2 shows the mutant CaSR. cells (23, 32). The mutant CaSR identified in the family with ADH described here is expressed at more robust levels on the cell surface than the WT CaSR. Moreover, functional studies in vitro showed that it exhibits similar Ca2⫹o-evoked Ca2⫹i responses when transfected alone or when cotransfected with the WT receptor. Therefore, this mutated allele may exert a dominant positive effect on the WT CaSR allele, just the opposite of the dominant negative action of R185Q (23, 32). This postulated mechanism is in accord with the similar clinical features of affected members of the family described here, despite differing gene dosages. That is, the homozygous patient remained asymptomatic into late adulthood, and his phenotype is no more severe than those of the other affected members of the family who are heterozygous for the mutation. What are the mechanisms through which this mutation could produce gain-of-function? The CaSR belongs to a recently identified and growing family of GPCRs (the family C GPCRs) characterized by very large extracellular domains and long cytoplasmic tails (218 residues in the case of the human CaSR). The introduction of truncations and point mutations within the CaSR’s C-tail have recently shown that the tail modulates several aspects of the receptor’s function, including signal transduction, intracellular receptor trafficking, and the level of cell surface expression (30, 33–35). Residues from 868 to 886 have been identified as crucial for normal signal transduction (30, 33–35). Receptors with deletions of more than 200 amino acids (e.g. those truncated at residues 863, 865, 874, or 877) are inactive despite exhibiting levels of cell surface expression equivalent to that of the WT receptor, if not more, whereas those with truncations of a lesser degree vary in their behavior (30, 33–35). Truncation LARGE DELETION WITHIN THE CaSR TAIL at residue 892 results in a CaSR that is not only functional but supranormal in its level of activity, as evidenced by its lowerthan-normal EC50 (3.2 ⫾ 0.1 mmol/L vs. 4 ⫾ 0.2 mmol/L for the WT CaSR) (30). A CaSR truncated at residue 903 also exhibits a greater level of cell surface expression than the WT CaSR (33), although its EC50 for Ca2⫹o-evoked increases in inositol phosphates are similar to that of the WT receptor. The naturally occurring deletion mutant identified in this study is located between residues 892 and 903. Similar to the latter two truncated receptors, the receptor studied here is also expressed on the cell surface at a greater level than the WT CaSR, as assessed by Western blot analysis and cell surface labeling. Therefore, one possible mechanism underlying its left-shifted EC50 could be a greater cell surface density of the mutant receptor. This mechanism is the converse of what is observed in mice heterozygous or homozygous for targeted disruption of the CaSR gene. Heterozygotes, in which there is about a 50% reduction in the level of the receptor in parathyroid gland (as assessed by immunohistochemistry), show a modest rightward shift in the set-point of the parathyroid gland for Ca2⫹o-induced inhibition of PTH secretion, whereas homozygotes, exhibiting an essentially complete loss of receptor from parathyroid gland, show a severe increase in set-point (36). The gain-of-function of this mutant receptor could also be explained by additional mechanisms. Indeed, two different mechanisms unrelated to cell surface expression might lead to a gain-of-function of a GPCR. First, numerous naturally occurring mutations of several different GPCRs are thought to mimic the conformational change(s) associated with normal ligand-induced activation of the GPCR and produce constitutively increased receptor activity that then modulates intracellular signaling pathways at lower-than-normal concentrations of agonist (37– 46). In contrast to these mutations localized along the extracellular, transmembrane, or loops domains, the CaSR mutation described here is a large deletion occurring in the cytoplasmic C-tail between S895 to V1075. Though it is not clear how this mutation would produce conformational changes similar to those caused by the CaSR’s agonists, we cannot rule out that such a mechanism occurs. Second, there might be deficient attenuation of signal transduction after initiation of signaling by the mutant CaSR, given that the C-tails of numerous GPCRs have been shown to play critical roles in attenuating signal transduction through diverse mechanisms, which include receptor desensitization, endocytosis, and down-regulation (47). For example, the rat gonadotropin releasing hormone receptor, which lacks a cytoplasmic tail, undergoes acute desensitization and accelerated internalization when a functional intracellular C-terminal tail is added (48). Thus, the in vivo and in vitro results in our study could also be consistent with a potential role for the portion of the CaSR’s C-tail between residues 895 and 1075 in endocytosis and/or down-regulation of this receptor, leading to its higher cell-surface expression and allowing more ligand-binding domains. Further in vitro studies will be necessary to explore the possible role of the CaSR’s C-tail in these processes. In summary, we have identified a family with ADH caused by a deletion of 181 amino acids within the C-terminal cytoplasmic tail of the CaSR. This large deletion leads to a 1701 greater cell surface expression of the CaSR and causes a gain-of-function that is responsible for the disease. Surprisingly, the presence of the mutation in the homozygous state in one affected family member does not cause a more severe phenotype, possibly because of a dominant positive effect of the mutant CaSR on the WT receptor when expressed together. This naturally occurring, large deletion of the CaSR’s C-tail confirms the conclusions drawn from several previous in vitro studies. That is, a large portion of the CaSR’s Cterminal tail is not indispensable for its biological activity but contains determinants that may constrain the receptor’s expression and/or its level of intrinsic activity or participate in the attenuation of signal transduction. To our knowledge, this is the first report of an activating mutation resulting from a large, naturally occurring deletion of the cytoplasmic tail of a GPCR. Acknowledgments We thank Dr. F. Bonnet-Boutillon (Sancheville, France) for her clinical support and L. Zekraoui (Service de Biochimie A, Hôpital Pitié Salpétrière, Paris, France) and Shu Yi Sun (Brigham and Women’s’ Hospital, Boston, MA) for their excellent technical assistance. References 1. Bilezikian JP, Thakker RV. 1997 Hypoparathyroidism. Curr Opin Endocrinol Diabetes. 4:427– 432. 2. Finegold DN, Armitage MM, Galiani M, et al. 1994 Preliminary localization of a gene for autosomal dominant hypoparathyroidism to chromosome 3q13. Pediatr Res. 36:414 – 417. 3. Lovlie R, Eiken HG, Sorheim JI, Boman H. 1996 The Ca2⫹-sensing receptor gene (PCAR1) mutation T151 M in isolated autosomal dominant hypoparathyroidism. Hum Genet. 98:129 –133. 4. Janicic N, Soliman E, Pausova Z, et al. 1995 Mapping of the calcium-sensing receptor gene (CASR) to human chromosome 3q13.3–21 by fluorescence in situ hybridization, and localization to rat chromosome 16. Mamm Genome. 6:798 – 801. 5. Brown EM, Gamba G, Riccardi D, et al. 1993 Cloning and characterization of an extracellular Ca2⫹-sensing receptor from bovine parathyroid. Nature. 366:575–580. 6. Garrett JE, Capuano IV, Hammerland LG, et al. 1995 Molecular cloning and functional expression of human parathyroid calcium receptor cDNAs. J Biol Chem. 270:12919 –12925. 7. Masu M, Tanabe Y, Tsuchida K, Shigemoto R, Nakanishi S. 1991 Sequence and expression of a metabotropic glutamate receptor. Nature. 349:760 –765. 8. Houamed KM, Kuijper JL, Gilbert TL, et al. 1991 Cloning, expression, and gene structure of a G-protein-coupled receptor from rat brain. Science. 252:1318 –1321. 9. Kaupmann K, Huggel K, Heid J, et al. 1997 Expression cloning of GABA(B) receptors uncovers similarity to metabotropic glutamate receptors. Nature. 386:239 –246. 10. Ryba NJ, Tirindelli R. 1997 A new multigene family of putative pheromone receptors. Neuron. 19:371–379. 11. Herrada G, Dulac C. 1997 A novel family of putative pheromone receptors in mammals with a topographically organized and sexually dimorphic distribution. Cell. 90:763–773. 12. Matsunami H, Buck LB. 1997 A multigene family encoding a diverse array of putative pheromone receptors in mammals. Cell. 90:775–784. 13. Hoon MA, Adler E, Lindemeier J, Battey JF, Ryba NJ, Zuker CS. 1999 Putative mammalian taste receptors: a class of taste-specific GPCRs with distinct topographic selectivity. Cell. 96:541–551. 14. Pollak MR, Brown EM, Estep HL, et al. 1994 Autosomal dominant hypocalcemia caused by a Ca2⫹-sensing receptor gene mutation. Nat Genet. 8:303–307. 15. Brown EM, Vassilev PM, Quinn S, Hebert SC. 1999 G-protein-coupled, extracellular Ca2⫹-sensing receptor: a versatile regulator of diverse cellular functions. Vitam Horm. 55:1–71. 16. Lelong M, Canlorbe P, Lagrue G, Bader JC. 1968 Familial hypoparathyroidism with hypercalciuria. Ann Pediatr (Paris). 16:253–268. 17. Watanabe T, Bai M, Lane CR, et al. 1998 Familial hypoparathyroidism: identification of a novel gain-of-function mutation in transmembrane domain 5 of the calcium-sensing receptor. J Clin Endocrinol Metab. 83:2497–2502. 18. Kifor O, Diaz R, Butters RR, Brown EM. 1997 The Ca2⫹-sensing receptor activates phospholipases C, A2, and D by high extracellular Ca2⫹ in bovine 1702 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. LIENHARDT ET AL. parathyroid and CaR-transfected, human embryonic kidney (HEK293) cells. J Bone Miner Res. 12:715–725. Bai M, Janicic N, Trivedi S, et al. 1997 Markedly reduced activity of mutant calcium-sensing receptor with an inserted Alu element from a kindred with familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism. J Clin Invest. 99:1917–1925. Sambrook J, Frisch EF, Maniatis T. 1989 Isolation of high-molecular-weight DNA from mammalian cells: protocol I. In: Sambrook J, Frisch EF, Maniatis T, eds. Molecular cloning. A laboratory manual. 2nd ed. New York: Cold Spring Harbor Laboratory Press; 916 –919. Pollak MR, Brown EM, Wu Chou YH, et al. 1993 Mutations in the human Ca2⫹-sensing receptor gene cause familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism. Cell. 75:1297–1303. Pearce SHS, Trump D, Wooding C, et al. 1995 Calcium-sensing receptor mutations in familial benign hypercalcemia and neonatal hyperparathyroidism. J Clin Invest. 96:2683–2692. Bai M, Quinn S, Trivedi S, et al. 1996 Expression and characterization of inactivating and activating mutations in the human Ca2⫹-sensing receptor. J Biol Chem. 271:19537–19545. Perry Y, Finegold D, Armitage M, Ferrell R. 1994 A missense mutation in the Ca sensing receptor causes familial autosomal dominant hypoparathyroidism. Am J Hum Genet. [Suppl] 55:A17. Pearce SHS, Williamson C, Kifor O, et al. 1996 A familial syndrome of hypocalcemia with hypercalciuria due to mutations in the calcium-sensing receptor. N Engl J Med. 335:1115–1122. Baron J, Winer KK, Yanovski JA, et al. 1996 Mutations in the Ca2⫹-sensing receptor gene cause autosomal dominant and sporadic hypoparathyroidism. Hum Mol Genet. 5:601– 606. De Luca F, Ray K, Mancilla EE, et al. 1997 Sporadic hypoparathyroidism caused by de novo gain-of-function mutations of the Ca2⫹-sensing receptor. J Clin Endocrinol Metab. 82:2710 –2715. Okazaki R, Chikatsu N, Nakatsu M, et al. 1999 A novel activating mutation in calcium-sensing receptor gene associated with a family of autosomal dominant hypocalcemia. J Clin Endocrinol Metab. 84:363–366. Brauner-Osborne H, Jensen AA, Sheppard PO, O’Hara P, Krogsgaard-Larsen P. 1999 The agonist-binding domain of the calcium-sensing receptor is located at the amino-terminal domain. J Biol Chem. 274:18382–18386. Bai M, Trivedi S, Brown EM. 1998 Dimerization of the extracellular calciumsensing receptor (CaR) on the cell surface of CaR-transfected HEK293 cells. J Biol Chem. 273:23605–23610. Bai M, Trivedi S, Kifor O, Quinn SJ, Brown EM. 1999 Intermolecular interactions between dimeric calcium-sensing receptor monomers are important for its normal function. Proc Natl Acad Sci USA. 96:2834 –2839. Bai M, Pearce SHS, Kifor O, et al. 1997 In vivo and in vitro characterization of neonatal hyperparathyroidism resulting from a de novo, heterozygous mutation in the Ca2⫹-sensing receptor gene: normal maternal calcium homeostasis as a cause of secondary hyperparathyroidism in familial benign hypocalciuric hypercalcemia. J Clin Invest. 99:88 –96. Ray K, Fan GF, Goldsmith PK, Spiegel AM. 1997 The carboxyl terminus of the human calcium receptor. J Biol Chem. 272:31355–31361. JCE & M • 2000 Vol 85 • No 4 34. Gama L, Breitwieser GE. 1998 A carboxylterminal domain controls the cooperativity for extracellular Ca2⫹ activation of the human calcium-sensing receptor. A study with receptor-green fluorescent protein fusions. J Biol Chem. 273:29712–29718. 35. Bai M, Trivedi S, Lane CR, Yang Y, Quinn SJ, Brown EM. 1998 Protein kinase C phosphorylation of threonine at position 888 in Ca2⫹o-sensing receptor (CaR) inhibits coupling to Ca2⫹ store release. J Biol Chem. 273:21267–21275. 36. Ho C, Conner DA, Pollak MR, et al. 1995 A mouse model for familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism. Nat Genet. 11:389 –394. 37. Gether U, Kobilkas K. 1998 G-protein-coupled receptors. II. Mechanism of agonist activation. J Biol Chem. 273:17979 –17982. 38. Shenker A, Laue L, Kosugi S, Merendino Jr JJ, Minegishi T, Cutler Jr GB. 1993 A constitutively activating mutation of the luteinizing hormone receptor in familial male precocious puberty. Nature. 365:652– 654. 39. Laue L, Chan WY, Hsueh AJW, et al. 1995 Genetic heterogeneity of constitutively activating mutations of the human luteinizing hormone receptor in familial male-limited precocious puberty. Proc Natl Acad Sci USA. 92:1906 – 1910. 40. Gromoll J, Partsch CJ, Simoni M, et al. 1998 A mutation in the first transmembrane domain of the lutropin receptor causes male precocious puberty. J Clin Endocrinol Metab. 83:476 – 480. 41. Parma J, Duprez L, Van Sande J, et al. 1993 Somatic mutations in the thyrotropin receptor gene cause hyperfunctioning thyroid adenomas. Nature. 365:649 – 651. 42. Parma J, Van Sande J, Swillens S, Tonacchera M, Dumont J, Vassart G. 1995 Somatic mutations causing constitutive activity of the thyrotropin receptor are the major cause of hyperfunctioning thyroid adenomas: identification of additional mutations activating both the cyclic adenosine 3⬘,5⬘-monophosphate and inositol phosphate- Ca2⫹ cascades. Mol Endocrinol. 9:725–733. 43. Duprez L, Parma J, Costagliola S, et al. 1997 Constitutive activation of the TSH receptor by spontaneous mutations affecting the N-terminal extracellular domain. FEBS Lett. 409:469 – 474. 44. Holzapfel HP, Führer D, Wonerow P, Weinland G, Scherbaum WA, Paschke R. 1997 Identification of constitutively activating somatic thyrotropin receptor mutations in a subset of toxic multinodular goiters. J Clin Endocrinol Metab. 82:4229 – 4233. 45. Führer D, Wonerow P, Willgerodt H, Paschke R. 1997 Identification of a new thyrotropin receptor germline mutation (Leu629Phe) in a family with neonatal onset of autosomal dominant nonautoimmune hyperthyroidism. J Clin Endocrinol Metab. 82:4234 – 4238. 46. Jüppner H, Schipani E. 1997 The parathyroid hormone/parathyroid hormone-related peptide receptor in Jansen’s metaphyseal chondrodysplasia. Curr Opin Endocrinol Diabetes. 4:433– 442. 47. Böhm SK, Grady EF, Bunnett NW. 1997 Regulatory mechanisms that modulate signaling by G-protein-coupled receptors. Biochem J. 322:1–18. 48. Heding A, Vrecl M, Bogerd J, et al. 1998 Gonadotropin-releasing hormone receptors with intracellular carboxylterminal tails undergo acute desensitization of total inositol phosphate production and exhibit accelerated internalization kinetics. J Biol Chem. 273:11472–11477.