Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
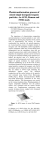
Pediatr Clin N Am 50 (2003) 717 – 731 The delivery of inhaled medication to the young child Bruce K. Rubin, MD, MEngr, FRCPC, FAARC, FCCPa,*,1, James B. Fink, MS, RRT, FAARCb,2 a Wake Forest University School of Medicine, Medical Center Boulevard, Winston Salem, NC 27157, USA b Aerogen, Inc., 2071 Stierlin Court, Mountain View, CA 94043, USA For more than 150 years, attempts have been made to deliver therapeutic aerosols directly to the airways. The modern era of aerosol therapy began with the introduction of the Wright nebulizer (no longer manufactured, was Wright) in 1958 [1] and the Medihaler Epi (no longer manufactured, was 3M) in 1956 [2]. Significant advances in aerosol technology have made this mode of medication delivery much more efficient so that it is now the most widely used form of therapy for chronic airways diseases such as asthma. The advantage of aerosol delivery is that the medication is administered directly to the site of disease in the airway providing topical effect while reducing the risk of systemic side effects and decreasing medication costs. For an aerosol device to deliver medication efficiently to the lower respiratory tract, it must be able to generate a cloud of medication particles with most of these particles being of a size allowing efficient inhalation and deposition in the airway [3]. The patient must be willing to inhale the aerosol with a slow, deep inspiratory maneuver to maximize aerosol deposition in the airway, followed by a breath hold to allow sedimentation of the medication particles. Information regarding inhaled particle mass, lung deposition, and regional distribution of aerosols is more limited in neonates, infants, and young children than in adults. Aerosol delivery is substantially less efficient for this population. Pulmonary deposition of aerosol to neonates may be less than 1% of the nominal dose of drug being nebulized, compared with 8% to 22% in adults. Although little is known about delivered dose, it seems that in many cases adult doses of * Corresponding author. E-mail address: [email protected] (B.K. Rubin). 1 Dr. Rubin is a consultant to GlaxoSmithKline, Inhale, Aerogen, Monaghan Medical, AstraZenica, AIR/Alkemes, and Forest Labs. 2 Mr. Fink is an employee of Aerogen, Inc. 0031-3955/03/$ – see front matter D 2003 Elsevier Inc. All rights reserved. doi:10.1016/S0031-3955(03)00049-X 718 B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 Fig. 1. Typical respiratory flow-time traces for an adult or older child, young child, and infant under 6 months, showing the hypothetical differing effects of air entrainment on the proportion of nebulizer output inhaled at a compressed flow rate of 6 L/minute. TI = inspiratory time for a single breath; Ttot = total time for a single respiratory cycle. (From Collis GG, Cole CH, Le Souef PN. Dilution of nebulized aerosols by air entrainment in children. Lancet 1990;336:341 – 3; with permission.) aerosolized bronchodilator have comparable safety and efficacy profiles in infants and children. The reduced deposition seems to reduce the deposited dose sufficiently [4]. Rationales to reduce dosages for infants and small children have not been well substantiated in the literature. Although the fetus has a fully defined conducting airway early in its development, airway size changes dramatically in the first years of life. In addition, breathing patterns, flow, and volumes all change with growth and development (Fig. 1). The resting respiratory rate decreases with age, and tidal volume and minute ventilation increase. In the first year of life, tidal volume increases by 300% and then remains at approximately 7 mL/kg for the next several years. Aerosol size and particle deposition Aerosol size and particle deposition are important variables in the therapeutic effect of an aerosolized medication. An aerosol is a group of particles that remains suspended in air for a relatively long time because of low terminal settling velocity. The terminal settling velocity of a particle is the velocity at which the particle will fall in air because of gravity. This terminal settling velocity is related to the size and density of the particle. Aerosol particle size is usually reported as the mass median aerodynamic diameter (MMAD). For a uniform and spherical particle, the MMAD is defined as the particle diameter multiplied by the square root of the particle density, which, for water, is 1. Because particles are non-uniform in density and shape, particles are usually sized by their settling B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 719 behavior on a series of baffles in a cascade impactor. This yields information about the MMAD and also about the particle size distribution or geometric standard deviation (GSD). By definition, a GSD of less than 1.22 defines a monodisperse aerosol. Nearly all therapeutic aerosols are heterodisperse, but the smaller the GSD, the greater is the proportion of particles clustering around the MMAD. In general the respirable fraction of a therapeutic aerosol is defined as the volume of particles between 0.5 to 5 mm MMAD. Particles larger than 5 mm tend to impact in the oral pharynx leading to swallowing, systemic effects, and loss of medication. Oral pharyngeal deposition has been associated with thrush or laryngeal dysfunction with inhaled corticosteroids (ICS). Very large particles deposit in the device itself. Extremely fine particles, on the other hand, do not settle in the airway and can be exhaled. The three major mechanisms of aerosol deposition are inertial impaction, gravitational sedimentation, and diffusion. Each mechanism theoretically affects aerosol delivery to infants and small children. Inertial impaction is the primary mechanism for deposition of particles larger than 3 mm. The smaller diameters of upper and lower airways in infants and children result in a greater percentage of particles in this size range impacting in the structures of the upper airway. In addition, preferential nose breathing further filters aerosol from inspired gas, reducing the mass of drug available for pulmonary deposition. Inertial impaction is highly flow dependent, so during high inspiratory flow there is a greater tendency for even smaller particles to impact and deposit in the airway. In contrast, slow inspiratory flow allows larger particles to pass through the upper airways and into the lungs. Gravitational sedimentation describes the effect of gravity on particles that are not influenced by inertia. Gravitational sedimentation is the primary mechanism of deposition for particles smaller than 2 mm and also affects larger particles under low-flow situations. The longer particles reside in the lungs, the greater is their rate of deposition. Breath holding for 5 to 10 seconds is recommended after inhalation of an aerosol to maximize sedimentation time and to increase deposition in the lung periphery. The low tidal volume and relatively small vital capacity (VC) and functional residual capacity (FRC) and short respiratory cycles of infants result in lower resident time for small particles in the lungs, decreasing pulmonary deposition. Diffusion primarily affects particles so small that Brownian motion is a greater influence on particle movement than gravity. Random Brownian movement results in both collision and coalescence of particles with airway structures and with other particles. Particles tend to coalesce or to be attracted by the mass of other objects when they are within a distance of less than 25 times their diameter. The ability of a device to produce appropriately sized particles is a function of how the device is designed and how the device is used. For example, spontaneous breathing results in greater deposition of aerosol from a jet nebulizer than positive pressure breaths delivered by intermittent positive pressure ventilation which reduces aerosol deposition by more than 32% compared with spontaneously inhaled aerosols [5]. Potential problems and challenges of aerosol 720 B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 delivery are both patient- and device-specific [6,7]. The following sections review the appropriate use of each of these devices and common factors that limit aerosol delivery. Nebulizers The earliest aerosol devices used a bulb atomizer similar to those used for some perfume sprays. The bulb atomizer is an extremely inefficient means of nebulization producing only coarse particles. Nebulizers used today include ultrasonic nebulizers, Venturi type jet nebulizers, and other modern nebulizers including breath-activated, vibrating mesh, and breath-enhanced nebulizers. In some cases computer circuitry is used to regulate the particle size and initiation of aerosol delivery to time delivery with patient inhalation. Ultrasonic nebulizers generate an aerosol by means of a rapidly vibrating piezoelectric crystal. Although large volumes of solution can be nebulized by ultrasonic nebulizers, this process tends to produce coarser particles that are too large for efficient inhalation, the heat of the crystal can denature some medications (particularly proteins), and the crystal can develop coating or cracking that can be difficult to detect [8]. In ultrasonic nebulizers producing small particles, delivery of suspensions can be problematic; when the aerosol particle is smaller than the particles in suspension, nebulization is inefficient. Currently available ultrasonic nebulizers have medication volumes of up to 1.2 mL remaining in the reservoir after nebulization is complete. Ultrasonic nebulization delivers medication less effectively and efficiently than other devices, and the authors do not now recommend the use of ultrasonic nebulizers for delivering therapeutic aerosols [9]. Venturi type jet nebulizers deliver medication by the Bernoulli principle. Compressed gas passed through a narrow orifice draws a drug solution into the aerosol jet where it is sheared and driven into a series of baffles; larger particles impact the baffles and return to the medication reservoir, while smaller particles exit the nebulizer. Traditional jet nebulizers introduce compressed gas into the lower part of the reservoir, whereas more modern devices incorporate an additional vent on top of the reservoir. Nebulizer efficiency is fairly low (usually less than 10%), and there are significant differences between individual nebulizers, between different nebulizer brands, and between different compressors [10,11]. In general, the greater the pressure and flow of compressed air, the smaller and more consistent is the particle delivered. For patients in hospital, jet nebulizer therapy is generally administered using compressed air or oxygen at 50 pounds per square inch (psi) to generate a flow through the nebulizer of 6 to 8 L/minute. This pressure produces an acceptable particle size and an acceptable nebulization time of approximately 5 to 10 minutes for a 4-mL fill volume. The compressed air flow in home compressors and ventilator circuits can vary greatly; those that deliver less than 6 L/minute (often at 10 – 15 psi) are extremely inefficient at generating particles of appropriate size for inhalation and should not be used [12]. B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 721 Most of the available medication in the nebulizer cup is nebulized in the first few minutes [10]. All nebulizer cups have some amount of medication remaining near the end of therapy, when aerosol generation becomes intermittent. This intermittent nebulization is referred to as sputtering; it has been documented that aerosol delivery to the patient declines by half within 20 seconds of the onset of sputtering [13]. At this time it is appropriate to discontinue therapy. The residual volume remaining in the nebulizer cup is unavailable to the patient. The residual volume of medicine that remains in commercial smallvolume nebulizers varies from 0.5 to 2.0 mL depending on the specific device. By increasing the fill volume, usually by adding saline as a diluent, a greater proportion of the medication can be nebulized at the cost of increased administration time [6,14]. For example, with a 1-mL residual volume, a fill of 2 mL would only leave 50% of the nebulizer charge available for nebulization, whereas a fill of 4 mL would make 75% of the medication available for nebulization. Because the nebulizer is now aerosolizing 3 mL instead of 1 mL, treatment time is increased threefold. Many unit-dose medication vials contain just 2 or 3 mL of solution, and the authors find that patients are rarely advised to add additional saline to increase the nebulizer fill volume to a full 4 mL. Breath-enhanced jet nebulizers have an inspiratory valve system that allows the patient to entrain additional air with inhalation and recycles the medication within the nebulizer cup when the patient is not inhaling. This system is far more efficient than that in older nebulizers with no recycling system (continuous nebulization), in which up to 70% of the medication was lost to the environment during patient exhalation. A disadvantage with all recycling systems is that they increase nebulization times. The longer the nebulization time, the less likely it is that the patient will consistently take deep breaths to allow maximal aerosol delivery to the lower respiratory tract. Dr. Harm Tiddens in Rotterdam has identified nebulizer mouthpieces that have been chewed on by bored patients leaving a small narrow orifice (Fig. 2). This narrowing markedly changes the nebulizer output and significantly reduces the amount of medication available to the patient. Because medication is available to the patient only on inhalation and delivery is most efficient with quiet inhalation, almost no medication is deposited into the airway of a crying infant or child [15,16]. In essence, crying is a very long exhalation followed by a rapid and brief inhalation. During exhalation, medication is unavailable, and during a very fast inhalation the inertia of the inhaled medication makes it more likely to be deposited in the oral pharynx than in the airway. Patient agitation makes achieving a good seal on either the mouthpiece or the mask used to deliver medication less likely. When any form of aerosol therapy is administered to an infant or small child (generally under the age of 5 years), a mask is often used to permit effective aerosol deposition. The mask must be comfortable and fit tightly on the face for aerosol to be efficiently delivered (Fig. 3). The correct mask size must be chosen for each patient. Even small leaks around the mask can profoundly compromise aerosol delivery [17]. The airway deposition of aerosol obtained 722 B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 Fig. 2. Nebulizer mouthpiece that was chewed out of boredom substantially decreasing nebulizer output. (Courtesy of Dr. Harm Tiddens, Sophia Children’s Hospital, Rotterdam, The Netherlands.) with a well-fitting mask seems to be similar to that of a properly used mouthpiece [18]. Blow-by delivery of medication using mask or tubing held near the child’s face delivers a negligible amount of medication to the child [19]. The authors therefore strongly recommend that aerosol medications never be given by a blow-by technique or administered to a crying child. It is far more efficient to administer Fig. 3. A properly fitted mask is essential for efficient aerosol delivery to infants and small children. (Courtesy of Pari Respiratory Equipment, Monterey, CA.) B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 723 medications by nebulization to a sleeping child with a mask held tightly on the face [20]. The performance of nebulizers can vary, even among those made by the same manufacturer [21]. If they are not scrupulously cleaned, nebulizers can become colonized by microorganisms [22,23]; even with good care, nebulizer performance can decline over time [24,25], and nebulizers should be frequently replaced. In general, nebulizer therapy is less convenient for patients than medication delivered by devices such as pressurized metered dose inhalers (pMDIs) or dry powder inhalers (DPIs) because the amount of time needed to deliver medication is greater and the apparatus, including the nebulizer, a compressor, and unit doses of medication, is more complex. Because medication unit doses are more expensive than multidose inhalers, and because the patient requires significantly greater nominal amounts of medication than with other aerosol techniques, medication costs tend to be greater as well. The limitations in terms of cost, convenience, portability, and efficiency make nebulization a poor choice for aerosol delivery in most circumstances [26]. Some medications are poorly soluble and must be nebulized as a suspension rather than as a solution. Most inhaled corticosteroids are lipophilic; inhaled corticosteroids delivered by jet nebulizers are effective but inefficient because these agents must be administered as suspensions. Therefore, costs are greater, deposition is less, and delivery time may be longer. The authors do not recommend administering inhaled corticosteroids by nebulization when other less expensive and more efficient devices can be used. Newer and more efficient nebulizers are currently being clinically tested. These devices include breath-activated nebulizers that trigger nebulization only when the patient inhales, breath-enhanced nebulizers that provide most of the inhaled therapeutic aerosol at the beginning of inhalation (thus maximizing lower airway deposition), and particle size – enhanced nebulizers (such as vibrating mesh nebulizers) that are more efficient in producing a greater proportion of particles within the respirable range. In recent years, newer vibrating mesh technology has been introduced that uses a piezo element (operating at frequencies lower than those in ultrasonic nebulizers) to vibrate an aperture plate or mesh to create an electronic pumping action; particle size is dictated by the diameter of the apertures (Fig. 4). These nebulizers produce consistent particle sizes with a relatively high output (0.2 – 0.6 mL/minute) and low residual volumes of less than 0.2 mL. Unlike the ultrasonic nebulizers, the vibrating mesh nebulizers do not heat or denature medications and can efficiently nebulize suspensions [27]. These nebulizers are silent and portable but are more expensive than standard compressor nebulizer systems. Although the MMAD of particles produced by most jet nebulizers is less than 5 microns and these particles therefore are in the respirable range, the GSD is greater than with other devices, so a much smaller proportion of particles are available for inhalation. Although the authors rarely use jet nebulizers for the delivery of therapeutic aerosols except when medication is not available in other aerosol delivery forms (eg, Pulmozyme, dornase alfa [Genentech, San Francisco, 724 B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 Fig. 4. Example of aerosol generator (upper left) using vibrating mesh technology. The aerosol generator uses a piezo element to vibrate an aperture plate (lower left) containing 1000 funnel-shaped orifices (magnified view, upper right) to create an electronic micropump (lower right), extruding aerosol droplets. Particle size is dictated by exit diameter of the aperture. (Courtesy of Aerogen, Inc., Mountain View, CA.) CA], TOBI [Chiron Corp, Emeryville, CA]), these newer nebulizers may prove to be an attractive alternative for some patients and may also improve the efficiency of administration of inhaled corticosteroid suspensions. Dry powder inhalers Dry powder inhalers generally produce fine particles of medication by scraping or milling from a larger reservoir of medication or by holding individual doses in capsules or blister packs. Because significant surface forces can cause small particles to clump together, increasing the particle size, many of these inhalers hold medications in humidity-protected blister packs or mixed with a carrier agent such as lactose to aid dispersion. When the patient inhales, the particles are deaggregated. In the earliest DPIs such as Rotahaler (GlaxoSmithKline, London, UK), Diskhaler (GlaxoSmithKline, London, UK), and Spinhaler (no longer manufactured, was Fisons), particle dispersion was critically dependent on high inspiratory flow, leading to inertial impaction of much of the aerosol in the upper airway. The first modern multidose DPI was the Turbuhaler (AstraZenica, B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 725 Crystal Lake, IL), in which medication is dispersed by a series of vanes within the device. This device is considered a moderate- to high-resistance inhaler because an inspiratory flow of less than 60 to 90 L/minute decreases the amount of medication available to the patient [28,29]. Although most healthy children over the age of 5 years are capable of generating a peak inspiratory flow of 60 L/minute or greater [30], the occasional child will have difficulty, especially during an acute asthma attack (Fig. 5). It has also been reported that medication output can be compromised for days if the Turbuhaler is subjected to humidity [31]. Changes in environmental humidity may be less important than the humidity generated when the child exhales into the device. High ambient humidity can also result from condensation forming inside the device when a DPI is brought into a warm indoor environment from the cold outdoors (or from inside a car on a very cold day) [32]. When this device is used appropriately by a well-trained patient, however, it delivers aerosol more effectively than most nebulizers and is as effective as a pMDI with a holding chamber. The Diskus (GlaxoSmithKline, Research Triangle Park, NC) is a lowerresistance multidose DPI; little difference is seen in the medication available to the patient even at a peak inspiratory flow as low as 30 L/minute. The medication is contained in individual blister packs that seem to be better protected from humidity. Novel DPI devices and medication preparations have also been developed to optimize deep lung deposition of very fine particles and are particularly well suited for systemic administration of proteins and peptides such as insulin and human growth hormone. A passive DPI device has been developed by Inhale Fig. 5. Peak inspiratory flow rate is age-dependent in groups of children trained to generate maximal inspiratory flow rates (diamond) and individual inexperienced children (circles). Data suggest that children under the age of 6 years may be poor candidates for dry powder inhalers requiring peak inspiratory flows of 60 L/minute or higher. (From Pederson S. Delivery options for the inhaled therapy in children over the age of 6 years. J Aerosol Med 1997:10:41 – 4; with permission.) 726 B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 Pharmaceuticals. In this device very fine powder particles (less than 1-mm MMAD) are produced and held within a chamber very similar to the valved holding chamber used with pMDIs. This device allows most of these fine particles to be inhaled deeply within the lungs, optimizing alveolar deposition. Using a different technology, the particles themselves can be engineered, preparing them with a coating of phosphatidylcholine surfactant (Pulmospheres, Inhale/Alliance Pharmaceuticals, San Carlos, CA) to enhance dispersion [33]. AIR/Alkermes (Cambridge, MA) has engineered porous particles of extremely low density so that larger-diameter particles behave like fine particles [34]. Both these technologies allow much smaller particles to be made and delivered with significantly lower surface forces, producing less particle cohesion and clumping. Therefore simple inhalation devices without dispersion baffles can be used with these engineered particles. The AIR/Alkemes particles and Pulmospheres are being evaluated primarily for the systemic delivery of proteins by means of the airway. In summary, with proper instruction, current DPIs offer an attractive alternative for aerosol delivery in children older than 5 years. Pressurized meter dose inhalers In 1954, the daughter of an executive of the Riker Company complained to her father that her asthma atomizer kept breaking, and she suggested that he make an asthma spray similar to the hair sprays that were popular at that time. This suggestion led to the development of the first metered dose inhaler, the Medihaler EpiTM containing 0.5% epinephrine [2]. The classic pMDI contains a formulation of medication and propellant, either as a suspension for inhaled corticosteroids or a solution with mixture of chlorofluorocarbon (CFC) propellants and surfactant. The drug/propellant mixture is charged into a metering valve and is expelled under pressure by compression of the canister into the actuator (or boot). These devices are compact and inexpensive and reliably deliver medication with MMAD in the respirable range. Because of the high velocity of medication exiting the actuator, the authors recommend always administering the medication with an accessory device. Available accessory devices include spacers, which are simply tube containers that permit the aerosol plume to develop and lose velocity, and valved holding chambers that capture the aerosol behind a valve and release medication only when the patient inhales [35]. At the Wake Forest University School of Medicine, the authors use only pMDIs with valved holding chambers because these devices reduce the importance of timing actuation with inhalation and prevent loss of medication should the child exhale into the device. Valved holding chambers allow the evaporation of carrier, decreasing the effective MMAD and, more importantly, decrease pharyngeal deposition, reducing side effects which can include oral thrush or laryngeal myopathy with inhaled corticosteroids. For a valved holding chamber to work efficiently, it must be comfortable to use. A comfortable and well-sealed mask is required for smaller children, and the child must be able to develop sufficient inspiratory flow B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 727 to open the chamber valve easily with tidal breathing. Valve design can compromise the efficiency of holding chambers; a pegged valve design eg, the Optihaler (Respironics1 Healthscan Asthma and Allergy Products, Cambridge, MA) can occasionally fail to open and close. The number of breaths needed for the patient to clear the chamber of medication depends on the size of the chamber, the child’s tidal volume, and the amount of dead space between the valve and the child’s mouth. In general, larger dead-space volumes eg, in the Babyhaler (GlaxoSmithKline, London, UK) decrease deposition efficiency [36]. Occasionally patients will contrive to actuate the pMDI into the valved holding chamber several times before inhaling. The authors strongly discourage this practice because a significant amount of medication is lost within the chamber and, with CFC-based pMDIs, the chilling of the device immediately following actuation and expansion of the CFC may reduce output. This loss that occurs with multiple actuations into a valved holding chamber largely results from static charge. Static charge can be reduced either by first washing the valved holding chamber with a small amount of liquid dish detergent and then air drying (not rinsing) it or perhaps by priming the chamber by firing several pMDI actuations into the valved holding chamber before use (Fig. 6). Theoretically this process should work for CFC-based pMDIs because of the surfactant in the canister; however, to the authors’ knowledge, this technique has not been well studied. A major problem that the authors have had with the use of currently available pMDI devices is patient unawareness of when the canister is empty. Most patients that the authors have interviewed who have not received specific training have Fig. 6. Static electricity in plastic spacers reduces the amount of budesonide available to the patient from a chlorofluorocarbon pressurized metered dose inhaler for the first 40 doses, compared with a metal spacer that delivers consistent dose throughout the life of the canister. (From Berg E. In vitro properties of pressurized metered-dose inhalers with and without spacer devices (review). J Aerosol Med 1995;8:S3 – 11; with permission.) 728 B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 continued to use their pMDI as long as they can hear the noise of the propellant with each actuation. Although companies will typically overfill the canister with medication by about 15%, the authors have found that commercially available pMDIs typically contain enough propellant to produce more than two times the number of actuations indicated by the nominal dose, suggesting that half of the actuations contain no significant amount of medication (Durotoye L, Rubin BK, unpublished data). Thus most of these patients refill their canisters half as often as needed, obtain medication only half the time, and yet think that they are using the medications appropriately. The authors refer to this situation as ‘‘pseudo nonadherence.’’ The Food and Drug Administration has recommended that all aerosol devices introduced in the future should contain a dose counter. Other problems that have been noted with pMDIs include failure to shake the canister thoroughly before actuating, use of too rapid an inspiratory flow, which increases the flow velocity and oral deposition of the medication, failure to take a deep-enough breath, failure to breath hold, and, at times, even failure to remove the cap from the actuator boot. The traditional CFC propellant used in pMDIs has the potential for ozone depletion. As part of the Montreal protocol, an agreement reached by many of the world’s developing countries in 1986 to reduce and eliminate emissions harmful Fig.7. Diagram of Autohaler (3M) breath-actuated pressurized metered dose inhaler. The lever loads the spring, pressing the canister. As the patient inhales, the triggering mechanism is activated, allowing the canister to be pressed down, firing into the actuator. (Coutesy of Autohaler, 3M, St. Paul, MN.) B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 729 to the ozone layer, it is mandated that CFC-containing pMDIs eventually be phased out of use. The hydrofluoroalkane (HFA) 134a has been successfully developed as a replacement for the most commonly used CFC. These new pMDI canisters contain medication, propellant, a co-solvent, and no surfactant [37]. Some inhaled corticosteriods, notably beclomethasone and flunisolide, are soluble in HFA 134a, and this solution produces particles approximately 1.1 to 1.2-mm MMAD. The smaller particles increase airway deposition three- to fourfold allowing significantly lower doses of medication to be administered and potentially improving distribution of the inhaled corticosteroid to smaller airways. Other inhaled corticosteroids such as budesonide and fluticasone remain as larger particle – sized suspensions even in HFA 134a. The Maxair Autohaler (3M, St. Paul, MN) is a flow-triggered pMDI designed to reduce the need for hand/breath coordination by firing in response to the patient’s inspiratory effort and by presenting a lower-velocity aerosol plume. To use the Autohaler, the patient cocks the lever on the top of the unit that springloads the canister against a vane mechanism (Fig. 7). When the patient’s inspiratory flow exceeds 30 L/minute, the vane moves, allowing the canister to be pressed into the actuator and thus firing the pMDI. Although the flow required to actuate the device may be too great for some young children to generate during acute exacerbations of asthma, most older children and adults are able to use this device effectively. To date, the Autohaler has been developed to administer only the b-agonist bronchodilator, pirbuterol. Summary The effective and efficient delivery of aerosol medications involves physician factors (correct diagnosis and correct prescription of appropriate medications), device factors, and patient factors. For nearly all infants and children, the authors administer asthma medications either using a pMDI with a valved holding chamber or a DPI. Regardless of the device chosen, parent and patient education is critical for the appropriate use of the device, and frequent reinforcement of the educational message will often improve adherence and correct use [38,39]. References [1] Wright BM. A new nebulizer. Lancet 1958;2:24 – 5. [2] Freedman T. Medihaler therapy for bronchial asthma: a new type of aerosol therapy. Postgrad Med 1956;20:667 – 73. [3] Rubin BK, Fink JB. Aerosol therapy for children. Respir Care Clin N Am 2001;7:175 – 213. [4] Anhoj J, Thorsson L, Bisgaard H. Lung deposition of inhaled drugs increases with age. Am J Respir Crit Care Med 2000;162:1819 – 22. [5] Dolovich MB, Killian D, Wolff RK, et al. Pulmonary aerosol deposition in chronic bronchitis: intermittent positive pressure breathing vs. quiet breathing. Am Rev Respir Dis 1977;115: 397 – 402. 730 B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 [6] Hess D, Horney D, Snyder T. Medication-delivery performance of eight small-volume, handheld nebulizers: effects of diluent volume, gas flow rate and nebulizer model. Respir Care 1989; 34:717 – 23. [7] The Nebuliser Project Group of the British Thoracic Society Standards of Care Committee. Current best practice for nebulizer treatment. Thorax 1997;52:S4 – S16. [8] Newman SP, Pellow PG, Clarke SW. In vitro comparison of DeVilbiss jet and ultrasonic nebulizers. Chest 1987;92:991 – 4. [9] Nakanishi AN, Lamb BM, Foster CF, et al. Ultrasonic nebulization of albuterol is no more effective than jet nebulization for the treatment of acute asthma in children. Chest 1997;111:1505 – 8. [10] Dolovich MB, Fink JB. Aerosols and devices. Respir Care Clin N Am 2001;7:131 – 73. [11] Hess D, Fisher D, Williams P, et al. Medication nebulizer performance. Effects of diluent volume, nebulizer flow, and nebulizer brand. Chest 1996;110:498 – 505. [12] Hadfield JW, Windebank WJ, Bateman JRM. Is driving gas flow clinically important for nebulizer therapy? Br J Dis Chest 1986;80:550 – 4. [13] Malone RA, Hollie MC, Glynn-Barnhart AM, et al. Optimal duration of nebulized albuterol therapy. Chest 1993;104:1114 – 8. [14] Reisner C, Katial RK, Bartelson BB, et al. Characterization of aerosol output from various nebulizer/compressor combinations. Ann Allergy Asthma Immunol 2001;86:566 – 74. [15] Iles R, Lister P, Edmunds AT. Crying significantly reduces absorption of aerosolized drug in infants. Arch Dis Child 1999;81:163 – 5. [16] Murakami G, Igarashi T, Adachi Y, et al. Measurement of bronchial hyperreactivity in infants and preschool children using a new method. Ann Allergy 1990;64:383 – 7. [17] Amirav I, Newhouse MT. Aerosol therapy with valved holding chambers in young l children: importance of the face mask seal. Pediatrics 2001;108:389 – 94. [18] Lowenthal D, Kattan M. Facemasks versus mouthpieces for aerosol treatment of asthmatic children. Pediatr Pulmonol 1992;14:192 – 6. [19] Everard ML, Clark AR, Milner AD. Drug delivery from jet nebulisers. Arch Dis Child 1992; 67:586 – 91. [20] Janssens H. Aerosol therapy in young children [doctoral thesis]. Rotterdam (The Netherlands): Erasmus University; 2001. [21] Alvine GF, Rodgers P, Fitzsimmons KM, et al. Disposable jet nebulizers: how reliable are they? Chest 1992;101:316 – 9. [22] Department of Health and Human Services. Centers for Disease Control and Prevention: guidelines for prevention of nosocomial pneumonia. Part 1. Issues on prevention of nosocomial pneumonia. Part 2. Recommendations for prevention of nosocomial pneumonia: notice of comment period. Am J Infect Control 1994;2:247 – 92. [23] Craven DE, Lichtenberg DA, Goularte TA, et al. Contaminated medication nebulizers in mechanical ventilator circuits: a source of bacterial aerosols. Am J Med 1984;77:834 – 8. [24] Standaert TA, Morlin GL, Williams-Warren J, et al. Effects of repetitive use and cleaning techniques of disposable jet nebulizers on aerosol generation. Chest 1998;114:577 – 86. [25] Merkus PJ, van Essen-Zandvliet EE, Parlevliet E, et al. Changes of nebulizer output over the years. Eur Respir J 1992;5:488 – 91. [26] Rubin BK, Newhouse MH, Barnes PJ. Conquering childhood asthma. Hamilton (Canada): Empowering Press, Decker Publications; 1998. [27] Dhand R. Nebulizers that use a vibrating mesh or plate with multiple apertures to generate aerosol. Respir Care 2002;47:1406 – 18. [28] Pedersen S, Hansen OR, Fuglsang G. Influence of inspiratory flow rate upon the effect of a Turbohaler. Arch Dis Child 1990;65:273 – 81. [29] Engel T, Scharling B, Skovsted B, et al. Effects, side effects and plasma concentrations of terbutaline in adult asthmatics after inhaling from a dry powder inhaler device at different inhalation flows and volumes. Br J Clin Pharmacol 1992;33:439 – 44. [30] Pederson S. Delivery options for inhaled therapy in children over the age of 6 years. J Aerosol Med 1997;10:S41 – 4. B.K. Rubin, J.B. Fink / Pediatr Clin N Am 50 (2003) 717–731 731 [31] Meakin BJ, Cainey J, Woodcock PM. Effect of exposure to humidity on terbutaline delivery from turbohaler dry powder inhalation devices. Eur Respir J 1993;6:760 – 1. [32] Newhouse MT, Kennedy A. Rapid temperature change from + 25 C to – 15 C impairs powder deaggregation in Bricanyl Turbuhaler. J Aerosol Med 1999;12:113. [33] Bot AI, Tarara TE, Smith DJ, et al. Novel lipid-based hollow-porous microparticles as a platform for immunoglobulin delivery to the respiratory tract. Pharm Res 2000;17:275 – 83. [34] Edwards DA, Hanes J, Caponetti G, et al. Large porous particles for pulmonary drug delivery. Science 1997;276:1868 – 71. [35] Wilkes W, Fink J, Dhand R. Selecting an accessory device with a metered-dose inhaler: variable influence of accessory devices on fine particle dose, throat deposition, and drug delivery with asynchronous actuation from a metered-dose inhaler. J Aerosol Med 2001;14:351 – 60. [36] Mitchell JP, Nagel MW. In vitro performance testing of three small volume-holding chambers under conditions that correspond with use by infants and small children. J Aerosol Med 1997;10: 341 – 9. [37] Fink JB. Metered-dose inhalers, dry powder inhalers and transitions. Respir Care 2000;45: 623 – 35. [38] Lewis RM, Fink JB. Promoting adherence to inhaled therapy: building partnerships through patient education. Respir Care Clin N Am 2001;7:277 – 301. [39] Janssens H. Aerosol therapy in young children [doctoral thesis]. Rotterdam (The Netherlands): Erasmus University; 2001. p. 138.