Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
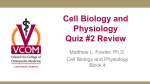
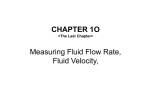
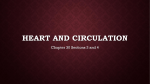
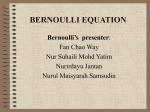
Cardiopulmonary Physiology Millersville University Dr. Larry Reinking Chapter 3 - Physical Properties of the Blood and Circulation Pressure Units In medical practice a variety of units are used for pressure, that is, force applied per area. These units include mm Hg, torr, cm H2O, atmospheres, mbars, pascal, newton/m2, dynes/cm2 and kPa. In most physiological research journals, as well as in clinical practice in Europe, SI (Système Internationale) units are used. In clinical practice in the U.S. however, mm Hg remains in common use, especially for the expression of blood pressure. For this reason, mm Hg will be the most used unit in this course. The following are conversion factors for these units: Unit atmospheres mbars cm H2O dynes/cm2 newton/m2 kilopascal torr (at 0°C) mm Hg unit mm Hg ÷ 760 mm Hg x 1.333 mm Hg x 1.36 mm Hg x 1333 mm Hg x 133.3 mm Hg x 0.133 same unit mm Hg atm. x 760 mbars ÷ 1.333 cm H2O ÷ 1.36 dynes/cm2 ÷ 1333 N/m2 ÷ 133.3 kPa ÷ 0.133 same Table 3.1 Pressure Conversions Pressure Differences The term 'pressure' is often used very loosely (as will be the practice in this course). Remember that pressure measurements are usually relative to some benchmark. When we say that the average arterial blood pressure is 100 mm Hg, more correctly we mean that the average arterial blood pressure is 100 mm Hg greater than atmospheric pressure. 'Pressure difference', 'pressure head' or ‘driving pressure’ are technically more precise terms. Effect of Gravity (Hemostatics) Pascal, in the 17th century, developed three laws applying to fluids at rest (hydrostatics). One of these laws essentially states that in a column of fluid, at rest under the influence of gravity, the pressure will increase with depth under the free surface. This pressure will depend on the density of the fluid. You can envision this law by imagining a plastic garbage can full of water. If you poke a hole in the side of the can near the bottom, water will spray out with more force than if you poke a hole near the top. In quantitative terms this relationship can be stated as follows: P = gh Equation 3.1 Where P is pressure, (rho) is density (in kg/l), g is gravitational acceleration (9.8 m/sec2) and, h is the depth (in m) below the free surface. Thus, the pressure at the base of a column of water, one meter high is: 1.0 kg/l x 9.8 m/sec2 x 1 m = 9,800 N/m2 = 73.5 mm Hg Chapter 3 1 If you check the math, recall that a liter of water is 0.001 m3 and that a newton is a kg.m/sec2. N/m2 was converted to mm Hg using the factor in Table 3.1. In the above example, 73.5 mm Hg refers to the pressure encountered at the bottom of a column of mercury 73.5 mm high. When using the 'column of' type pressure unit (cm H2O, mm Hg, etc.) we can convert from one measure to another by using a ratio of the densities. In the above situation the ratio of 1.0 densities is (densityO = 1.0 kg/l; densityHg = 13.6 kg/l). Thus, the mm Hg pressure 13.6 at the base of one meter column of water is: 1.0 1 meter H2O 1,000 mm H2O x = 73.5 mm Hg 13.6 If we changed the fluid to saline (density = 1.04 kg/l), the pressure would be 1.04 1,000 mm saline x = 76.5 mm Hg 13.6 and if the column was filled with blood (density = 1.056 kg/l, see p.1, chapter 2), then 1.056 1,000 mm blood x = 77.6 mm Hg. 13.6 The first measure of blood pressure was performed by inserting a long vertical tube into the crural artery of a horse. This famous experiment was reported in 1733 by Reverend Stephen Hales in his book Haemostaticks. Let us now consider the gravitational effects, on pressure, in the cardiovascular system. If we were to measure pressure (using Hales' technique), in a supine individual, at three different levels, say the heart, head and feet, we would obtain the same average arterial value of 100 mm Hg (which is equal to a 130 cm column of blood): 100 mm Hg 130 cm 100 mm Hg pressure loss to head Figure 3.1 130 cm pressure gain to feet Hydrostatic Columns In an erect individual, however, the different gravitational effects will cause a drop in pressure to the brain and an increase in pressure at the level of the feet. Suppose that we measure pressure in an cerebral artery 40 cm (400 mm) above the heart. At the level of this artery, 1.056 pressure will be reduced by 400 mm blood x = 31 mm Hg. In other words, the average 13.6 blood pressure at this level will only be 69 mm Hg (i.e., 100-31). If the feet are 130 cm below the heart, the average pressure in an artery at this level will be increased by 1300 mm blood x 1.056 = 100 mm Hg, that is, the total pressure will be 200 mm Hg (i.e., 100 + 100). 13.6 Chapter 3 2 Gravity Effects and Aviation Physiology The effects of gravity on static pressures are of prime interest in aviation physiology. As an aircraft pulls out of a dive, the pilot is subjected to a centripetal force at the bottom of the loop. This force may be several times gravity. Consider blood pressure to the head as a pilot experiences a 3g pullout. The gravitational influence is three times as large so that in our previous example the pressure to the head is reduced by 3 x 31 = 93 mm Hg. If the average pressure generated by the heart remains at 100 mm Hg, it is obvious that the brain will receive little blood. Blackout, caused by brain anoxia, occurs at around 3-4g in pilots. If the centripetal force is in the opposite direction, the blood pressure in the brain increases above normal. In this case, the retina becomes engorged with blood and a visual effect called red-out occurs. Transducer Placement and Gravity Effects The position of the measuring device has an effect on the apparent value of the arterial blood pressure (or pulmonary pressure, venous pressure, etc.). If the transducer is not at the same height as the heart (or other organ) a false high or low reading will be the result. This is especially important with low pressure recordings (such as venous pressure) because a small misplacement of the transducer can result in a large percent error. Hemodynamics Hemodynamics deals with the physical properties of flowing blood. This discipline borrows heavily from hydrodynamics, which is the study of moving fluids. By definition, a fluid cannot permanently resist a shearing force, that is, a force that causes layers within the fluid to slide over one another. If we use a stack of papers to represent a fluid, a shearing force would cause the papers to slide over one another and scatter across a table. Viscosity is a measure of a fluid’s ability to temporarily resist a shearing force. Principle of Bernoulli The pressure in a tube can be measured in different ways. It can be measured from the side of a tube (called side pressure, wall pressure or lateral pressure) or it can be measured from the end (end pressure): wall pressure difference due to kinetic energy end pressure wall pressure X Figure 3.2 end pressure End and Wall Pressures Note, in the above diagram, that end pressure is greater when the fluid is moving but drops, and is equivalent to the wall pressure, when the flow is stopped. The end pressure is a reflection of total energy and the difference between wall and end pressure, seen with flow, is due to kinetic energy (i.e., energy associated with motion). This kinetic component of pressure can be expressed as: Equation 3.2 P kinetic = 12 v2 where is the density of the fluid and v is the velocity. Bernoulli’s principle states that the total energy in a tube will remain constant with a given flow rate. Thus, if the velocity increases in a Chapter 3 3 tube (and the total energy is constant), the wall pressure will drop (note that doubling the velocity results in four times the kinetic pressure). In other words, more of the total energy will then be represented as kinetic pressure and the difference between the two tubes will be greater. The following diagram further illustrates this principle: Figure 3.3 low velocity high velocity low velocity Wall Pressure and Velocity of Flow The dotted line represents the pressure drop that would occur in a tube due to normal resistance to flow. At the constricted portion of the tube, velocity increases (principle of flow continuity, p. 5, chapter 1) and the wall pressure drops significantly. This is because more energy is converted to the kinetic component and since total energy is constant, the wall pressure must drop. In essence, the higher the velocity, the lower the wall pressure. Physiological Significance of the Bernoulli Principle Some arteries start as 90°, lateral branches from larger arteries, a situation similar to the wall pressure manometers depicted above. Coronary arteries, the nutritional source for the heart, are one example; they arise laterally from the aortic sinuses (Sinus of Valsalva) at the root of the aorta. Thus, the coronary circulation is fed by side pressure. Now consider the situation in aortic valve stenosis. The narrowed valve surface results in an increased velocity of blood movement (again, flow continuity) and, as a consequence, coronary artery pressure drops substantially. Fluid Flow in a Tube (Poiseuille’s Law) Suppose that we were able to inject a small amount of dye, at various points along the cross section, into water flowing through a glass tube. We would see the following type of results: Figure 3.4 Laminar Flow The velocity of water movement in the center, as shown by the dye movement, is greatest and becomes progressively slower near the wall of the vessel. These findings suggest that the fluid has a number of layers (or lamina), each moving at a different velocity. If we envision infinitely thin layers, the layer closest to the wall is impeded by cohesive forces and has no velocity. The next layer has a small velocity, the third’s velocity is a little larger, and so on, to the center of the tube. This type of flow is characteristic of viscous fluids moving at low velocities and is referred to as laminar flow or streamlined flow. Chapter 3 4 Poiseuille-Hagen Formula The following formula describes the rate of streamlined flow in a tube: 4 1 r Flow Rate = PA - PB 8 l or Flow Rate = P r 4 8 l Equation 3.3 P is pressure (dynes/cm2), the viscosity (poise), r the radius (cm) and l (cm) is the length. If the indicated units are used, the rate of flow will be in cm3/sec (i.e., ml/sec). Some of the terms in this equation are common sense, others are quite surprising. PA-PB is the driving pressure between point A and point B in the tube (also indicated as P). The greater the driving pressure, the greater the rate of flow. /8 is a geometrical term related to the circular cross section of the tube. 1/ indicates the inverse proportionality to the fluid viscosity. A more viscous fluid, such as molasses, will flow slower than water given the same driving pressure. r4/l - illustrates, first, that flow rate is decreased in long tubes, that is, resistance to flow increases with tube length. If you have ever tried to run water through several connected garden hoses, you have seen this principle at work. The relationship to r4 is a surprising and profound part of this formula. The significance of r4 is expanded in the next section. Flow Rate and Vessel Radius The r4 relationship is a very powerful part of the Poiseuille formula and is quite important to cardiovascular physiology. Local regulation of blood flow is regulated by vasoconstriction and vasodilation and this formula indicates that only small changes in a vessel’s radius are needed to bring about huge changes in blood flow. If a vessel were to double in diameter, the flow rate would increase 16x (i.e., 2x2x2x2). A vessel changing from a diameter of 1 mm to 0.8 mm will have only 41% (0.84) of the original flow. Perhaps you have heard of someone with a 90% occlusion in a coronary artery. This means that the flow in that artery (and the nutrition to that part of the heart) is only 0.01% (0.14) of normal! Newtonian Fluids vs. Blood A Newtonian fluid closely approximates the behavior predicted by Poiseuille’s law (Sir Isaac Newton derived some of the first principles involved with streamlined flow). Water and many other simple fluids have good Newtonian properties. On the other hand, blood is a nonNewtonian fluid. The presence of suspended cells and, perhaps, large protein molecules cause significant deviations from ideal Newtonian behavior. In addition, the circulation is not composed of rigid, straight tubes; rather they are elastic and branched. Quite unlike rigid tubes, when the pressure drops below a certain pressure (the critical closing pressure) blood vessels will collapse. Despite these problems, Poiseuille’s Law is a reasonable and useful approximation for blood flow in the circulation under normal physiological conditions. The following section deals with some of the non-Newtonian aspects of blood. Viscosity of Blood Chapter 3 5 Blood is a complex, colloidal solution with a viscosity about three times higher than water (water has a viscosity of 1 centipoise at 37°C). The apparent viscosity of blood is greatly affected by hematocrit, temperature and blood vessel diameter. Hematocrit - As the packed cell volume increases, the viscosity of blood rises in an almost exponential fashion: 14 12 Rela tive Viscosity 10 Figure 3.5 8 6 Hematocrit and Blood Viscosity 4 2 0 0 20 40 60 80 10 0 Hem atocrit (%) Above a hematocrit of 60%, viscosity rapidly rises (recall polycythemia vera, p. 3, chapter 2) and the work of the heart becomes extreme. Temperature - Like molasses, blood viscosity has a significant change with temperature. Blood cooled from 37°C to ≈0°C will increase viscosity by about 2.5x. This temperature effect is an important factor in frostbite and other cold injuries. As the affected tissue is cooled, perfusion is reduced, compounding the situation. Viscosity in Small Vessels (Fahraeus-Lindquist Effect) - A Newtonian fluid, such as water, has a viscosity that is independent of tube size. The apparent viscosity of blood does not follow this pattern and, surprisingly, greatly decreases in small (<0.05 mm diameter) tubes. This odd behavior may be attributed to the colloidal properties of blood. Chemists have described a similar phenomenon in colloidal solutions that is called the Sigma Effect. Recall that Poiseuille’s law is based on the assumption that numerous, small layers slide over one another. In blood and other colloids, the thickness of each layer is determined by the size of the colloid particle (i.e., an erythrocyte for blood). Thus, in a very small tube only a limited number of layers would be able to form and, therefore, a large deviation from expected behavior could occur. Axial Streaming of Blood Cells A final non-Newtonian property of blood is a of great interest; axial streaming. In a blood vessel, the red blood cells tend to cluster along the axis, leaving a layer near the wall that is primarily plasma: Figure 3.6 Axial Streaming of Red Blood Cells Note the smaller vessel branching laterally from the wall. This smaller vessel will have blood with a lower percent of red blood cells due to ‘plasma skimming’. Thus, the hematocrit in Chapter 3 6 various parts of the circulation can be quite different (‘finger prick’ blood can yield a hematocrit that is ≈25% lower than that in ‘large vessel’ blood from the same person). Also consider the placement of a needle when a blood sample is taken. A needle that just penetrates a vessel wall can produce a very different sample from one in which the needle extends into the axial stream of cells. Turbulent Flow Poiseuille’s Law indicates that as the driving pressure increases there will be a proportion increase in the rate of flow. Since the cross sectional area of the tube is constant, there will also be a proportional increase in velocity of blood movement. However, beyond a critical velocity this relationship will no longer hold true: Figure 3.7 Critical Velocity for Turbulent Flow Above this critical point the fluid no longer flows as sliding layers, but rather forms a series of chaotic swirls and eddies. Note that turbulent flow is much less efficient than laminar flow; for a given increase in driving pressure, there is a rather small increase in the rate of flow during turbulence. Reynolds first demonstrated that the critical velocity (Vc, cm/sec) depends on the radius of the tube (r, cm), density of the fluid (, g/ml) and viscosity (, poise) in the following fashion: K Equation 3.4 Vc = r K, the Reynold's number, is a constant that has a value of about 1000 for blood (and many other fluids) when flowing in a long straight tube. K is much smaller (as will be Vc) for branches, constrictions, bends and rough walls. In the normal circulatory system, turbulent flow occurs only periodically in the heart (see problem #3 at the end of the chapter). Turbulence and Circulatory Sounds While laminar flow is silent, the eddies and swirls of turbulent flow create vibrations; turbulent flow is noisy. The heart sounds are a result of turbulence caused by the opening and closing of the heart valves. Abnormal sounds can be heard with valvular defects (heart murmurs) or over atherosclerotic arteries (bruits). Turbulent sounds occur more often with anemia due to lowered blood viscosity (consider this in terms of the Poiseuille equation, flow continuity and the effect on Vc). The sounds used to determine indirect blood pressure (Karotkoff's sounds) are the result of compressing vessels with the blood pressure cuff and creating a momentary turbulent blood flow. Chapter 3 7 Resistance to Blood Flow Another way to look at the relationship between the rate of flow and pressure is by way of an analogy to Ohm’s law of electricity. Recall that this law involves voltage (E), current (I) and resistance (R) and states that I = E/R. In a similar fashion we can make a statement about the circulation if we consider the concept of resistance to blood flow. Thus the analogous relationship is: . P P and R = . Equation 3.5 Q = R Q A symbol topped by a dot implies a rate of flow (see Appendix I), Q. is used for blood flow, P is the driving pressure and R the resistance to blood flow. Incorporating the above relation ship with Poiseuille’s equation (Equation 3.3), R = P combined with . Q R = P l r4 . Q= 8 r 4 8 l gives an expression for vascular resistance: Vascular Resistance Equation 3.6 This value has units of dynessec/cm5 and is a commonly used measure in cardiovascular studies. The units, however, are not very intuititive so, for our purposes, a simpler approach will be used. The Peripheral Resistance Unit (PRU) is the vascular resistance when the mean arterial pressure is 100 mm Hg and the rate of blood flow is 100 ml/sec (100 ml/sec = 6 liters/min): R = P . Q = 100 mm Hg = 1PRU 100 ml/sec Peripheral Resistance Unit Equation 3.7 Thus, an individual with an average arterial pressure of 93 mm Hg and a cardiac output of 110 ml/sec has a peripheral resistance of 0.845 PRU. Series Resitance In a fashion analogous to electrical resistance, vascular resistances, in series, simply add to form a total resistance (RT): Equation 3.8 R T = R1 + R2 + R3 Series Resistance In the above situation, if R1 = 2 PRU, R2 = 1 PRU and R3 = 3 PRU then RT = 6 PRU. Parallel Resistance In a set of parallel resistances, the reciprocal of the total resistance is equal to the sum of the reciprocals of the individual resistances: Chapter 3 8 Equation 3.9 1 1 1 1 = + + RT R1 R2 R3 Parallel Resistance Cardiac Output, Resistance and Arterial Blood Pressure We can convert the above analogy to Ohm's law into terms that are more commonly used in circulatory physiology. The rate of flow ( Q. ) is called the cardiac output (CO), the driving pressure (P) is the difference between the arterial pressure and the venous pressure (Pa-Pv), and resistance is referred to as total peripheral resistance (RT). Using these terms the equation will now be: P Pv Equation 3.10 CO = a RT or, when stated in terms of arterial pressure becomes: Pa = (CO RT ) + Pv Equation 3.11 This last formula will be very valuable when we examine controls of arterial blood pressure and mechanisms in hypertension. Vascular Compliance (also called Capacitance or Distensibility) Compliance (C) refers to the pressure change (P) that occurs with a change in volume (V): C = V P Equation 3.12 A vessel that can take on a large additional volume with a small change in pressure is said to be highly compliant,while a vessel that has a large increase in pressure with a small volume addition is said to be non-compliant. The following graph depicts short term vascular compliance for an artery and vein: Pressure s ymp. s tim. Figure 3.8 artery Vascular Compliance s ymp. s tim. vein Volume In general, the venous system is much more compliant than the arterial system. As indicated above, the vasoconstricting action of sympathetic stimulation decreases compliance. Chapter 3 9 This graph also confirms a previous statement (p.5, chapter 1) that the volume contained within the venous system is greater than that in the arterial system. Delayed Compliance The relationship depicted in the above graph is valid for only a short period of time. The compliance of the vascular system will actually change, over time, following an addition or removal of volume. The following graph depicts the pressure change that will occur in an isolated vessel following the addition and removal of blood: Pressure remo ve vo lume Figure 3.9 Delayed Compliance add vo lume Time This phenomenon is called delayed compliance and is caused by a change in tone of the smooth muscle in the vessel wall. Smooth muscle when stretched or relaxed readjusts its tension (this is called stress-relaxation). A stretched vessel, as shown above, will readjust by becoming more compliant while a relaxed vessel becomes less compliant. Delayed compliance occurs to a greater degree in veins than in arteries. Physiological Significance of Delayed Compliance In clinical cases of over infusion of fluids or in cases of blood loss a number of mechanisms either correct or moderate a change in arterial blood pressure. Delayed compliance is one of these mechanisms; we will encounter several others in later chapters. Many organs maintain a constant blood flow, even over a wide range of perfusion pressures (60-120 mm Hg). This phenomenon is known as autoregulation and will still occur after the autonomic nerve supply to the arterioles has been removed. Delayed compliance may play a role in organ autoregulation of blood flow. Chapter 3 10 Some Blood Flow Problems 1. The cardiac output = 5.6 l/min (= 93 ml/sec = 93 cm3/sec) and the radius of the aorta = 1 cm. What is the velocity of blood flow in the aorta? (this problem deals with flow continuity, Equation 1.2) 2. The total cross-sectional area of the systemic capillaries is 5000 cm2. Using the information from the previous question, determine the velocity of blood flow in the systemic capillaries. 3. Does turbulent flow normally occur in the circulatory system? (this problem also deals with flow continuity) The most likely spot is in the aorta since this vessel has the highest blood velocity. Use the following information to answer this question: critical velocity for turbulence in the aorta = 40 cm/sec radius of the aorta = 1 cm cardiac output = 93 cm3/sec 4. Normal blood pressure is 120/80 mm Hg. What is the equivalent in kPa? in dynes/cm2? 5. Hold your hand at the level of your heart so that you can see the veins on the posterior surface. Lift your hand until the veins collapse and measure the distance you have raised your hand (in mm). This distance is a measure of venous pressure (i.e. a column of xx mm of blood). Using the specific gravities of blood and mercury, convert this measurement to mm Hg. 6. Given a circulatory system with the following: three parallel vascular beds (#1, #2, #3) where R1 = 3 PRU R2 = 3 PRU R3 = 2 PRU cardiac output = 100 ml/sec What is the mean arterial pressure? (assume venous pressure = 0) What is the rate of blood flow in each vascular bed? What happens to the mean arterial pressure if vascular bed #1 vasoconstricts and the resistance in this bed increases to 5 PRU? (assume that total blood flow stays the same) (consult Equations 3.7 through 3.11 for this problem) Chapter 3 11 7. A person is informed that they have a coronary artery that is 50% occluded. What effect has this occlusion had on blood flow in this vessel? (consult Poiseuille Equation, Equation 3.1) Chapter 3 12