Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
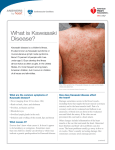
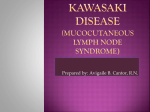
KAWASAKI DISEASE Learning about Kawasaki Disease and How It Affects Children Kawasaki disease is a frightening and rare condition in children. Amount of cases reported monthly in the duration of 10 years since 1988-1998 What is Kawasaki Disease? Kawasaki disease is a group of specific symptoms and physical signs. Kawasaki disease is associated with swelling and damage of the blood vessels, or arteries. This swelling and damage is called inflammation. Kawasaki disease often affects the arteries that supply the heart with blood. These are called the coronary arteries. Children who get the disease are usually less than 5 years old. It is very rare to get the disease after a child is 10 years old. The risk of other children in the same family getting Kawasaki disease is very low. The risk of a child getting Kawasaki disease for the second time is very rare. What Causes Kawasaki Disease? At present, no one actually knows what causes Kawasaki disease. Research is being done into the possible causes. Researchers now think that the disease may be caused by an infection. Normally, the body's immune system quickly recognizes germs and destroys them. But in the case of Kawasaki disease, a poison or toxin may be formed by the infection. This poison, or toxin, or perhaps the infection itself, makes certain individuals have an unusual, or abnormal reaction from the immunity system to the infection. However, we do not know what the infection or toxin is. We also do not know what makes some individuals more likely to get this disease than others. There is a slight chance that the brothers and sisters of a child with Kawasaki disease may also get the disease. But this is very rare. Unfortunately, there is no way we know of to prevent a child from getting the disease. Kawasaki Disease: Symptoms and Diagnosis All patients have a continuous fever lasting 5 days or more. 4 out of 5 of the following symptoms are also necessary before the doctor can know for sure, if a child has this disease. Symptoms Red eyes Redness of the lips, tongue or mouth Redness or swelling of the hands and feet A body rash Swelling of the glands in the neck Kawasaki Disease Symptoms: Red Eyes The below photo shows what the child’s eyes look like with Kawasaki disease. Kawasaki Disease Symptoms: Changes in the Lips, Tongue and Mouth Some changes which occur in the mouth and lips may be seen in the pictures below. These changes of the mouth and lips include such things as: redness, drying with cracking of the lips, and a red strawberry-like tongue. Kawasaki Disease Symptoms: Changes to the Hands and Feet The palms, or inside flat part of the hands, and the soles, or bottoms of the feet may turn red in colour. They may also appear swollen. About a week after the fever breaks, the skin from the fingers and toes may peel off, sometimes in large pieces. When this happens, new, normal skin shows below the peeling skin. Kawasaki Disease Symptoms: Body Rash A body rash usually first appears with the fever. The skin appears red and will feel 'bumpy' to the touch. A red rash can be seen in the groin or diaper area, particularly in young infants. This can also peel off later. Kawasaki Disease Symptoms: Swelling of the Glands in the Neck The picture below shows a child with swollen lymph nodes. You can sometimes feel these, just under the skin in the neck. Usually, they are soft, painless and about the size of a pea. In a child with Kawasaki disease, these lymph nodes may become swollen or enlarged. They become easier to feel. What is the Treatment for a Child with Kawasaki Disease? There is no single medicine, which can treat or cure Kawasaki disease. There are two medicines, which can be given to reduce the effects of Kawasaki disease Aspirin. Gamma Globulin. What are the Possible Serious Problems for a Child with Kawasaki Disease? 1. Changes in the Coronary Arteries: The most serious problems from Kawasaki disease have to do with its effects on the heart. During the disease, the arteries, which supply the heart with blood, called coronary arteries, can become inflamed and damaged 2. Formation of Aneurysms: Inflammation and damage to the coronary arteries could weaken their walls and cause the walls to develop pouches or sacs, called aneurysms. This is just like a weak spot in a tire or hose, that swells up with water or air. What is an Aneurysm? Normally, the walls of blood vessels are smooth and even. In Kawasaki disease, the muscular walls of the coronary arteries may become weakened. The pressure of the blood flowing through the arteries may cause these weak spots to balloonout, just like a weak spot in a tire or inner tube. Abnormal Angiogram: Aneurysm This is an angiogram of a heart with abnormal coronary arteries. The arrows point to some of the abnormalities. Here, the blood vessels are not smooth; they have ballooned out to form aneurysms. This can happen to a few children who have had Kawasaki disease. Tests to Monitor Heart Complications The following tests are used by a cardiologist to find out what possible effects Kawasaki disease has had on the heart and coronary arteries: 1. Echocardiography 2. Electrocardiography 3. Angiography Long Term Effects of Kawasaki Disease About 95 out of every 100 children who have had Kawasaki disease recover completely. If no damage in the coronary arteries is seen on the echo tests, then complete recovery is most likely. This means that there is little chance of future problems. If small aneurysms or dilations of the coronary artery are found, this is not serious. Small aneurysms tend to go away in about a year or two. Large or giant aneurysms do not tend to go away, and may lead to clots or narrowings. Although these children with severe coronary damage need to be followed closely, even these children tend to lead relatively normal lives LINK TO CORONARY ARTERY DISEASE There have been 74 reported cases of adult coronary artery disease attributed to childhood Kawasaki disease. The mean age at onset of symptoms of carditis and ischaemia was 25 (range 12 to 39) years with symptoms precipitated by exercise in 82% of these patients. LABORATORY FINDINGS Laboratory findings include neutrophilia, anaemia, thrombocytosis, elevated erythrocyte sedimentation rate, elevated serum transaminase levels, hypoalbuminemia and an elevated serum alpha1-antitrypsin level. Unlike atherosclerosis, no fatty streaks or macrophage accumulations occur. Other Significant Clinical and Laboratory Findings Cardiovascular: On auscultation, gallop rhythm or distant heart sounds; ECG changes (arrhythmias, abnormal Q waves, prolonged PR and/or QT intervals, occasionally low voltage, or ST-T wave changes); chest X-ray abnormalities (cardiomegaly); echocardiographic changes (pericardial effusion, coronary aneurysms, or decreased contractility); mitral and/or aortic valvular insufficiency; and rarely, aneurysms of peripheral arteries (e.g., axillary), angina pectoris, or myocardial infarction Gastrointestinal: Diarrhea, vomiting, abdominal pain, hydrops of gallbladder, paralytic ileus, mild jaundice, and mild increase of serum transaminase levels Blood: Increased erythrocyte sedimentation rate, leukocytosis with left shift, positive Creactive protein, hypoalbuminemia, and mild anemia in acute phase of illness (thrombocytosis in subacute phase) Urine: Sterile pyuria of urethral origin and occasional proteinuria Skin: Perineal rash and desquamation in subacute phase and transverse furrows of fingernails (Beau's lines) during convalescence Respiratory: Cough, rhinorrhea, and pulmonary infiltrate Joint: Arthralgia and arthritis Neurological: Mononuclear pleocytosis in cerebrospinal fluid, striking irritability, and rarely, facial palsy Prepared by Roshen John Group 27 of the 3rd course of medicine Ternopil State Medical University